Prompt CT Diagnosis of Epicardial Coronary Abscess after Percutaneous Coronary Intervention Caused by Klebsiella Pneumoniae
2
0
0
전체 글
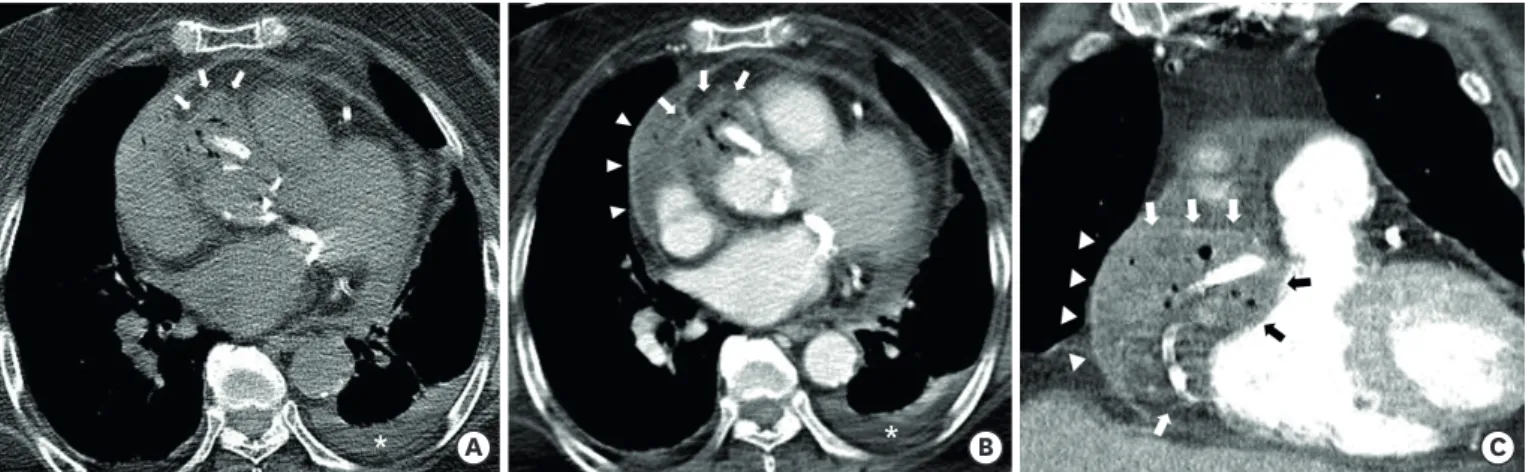
(2) Prompt CT Diagnosis of Epicardial Coronary Abscess. *. *. A. B. C. Figure 2. Chest CT images. (A) An air containing mass with high attenuation is noted on preconstrast CT around the proximal right coronary artery stent and along the right atrioventricular groove at the aortic sinus level (white arrows). Left pleural effusion is also seen (white asterisk). (B) On contrast enhanced axial CT image at the level of the left atrium, a low attenuation mass (arrows) with peripheral enhancement and multiple air-pockets is noted, consistent with air-forming epicardial coronary abscess (white and black arrows). Pericardial effusion (arrowheads) with linear pericardial thickening and enhancement is also demonstrated, indicating pericarditis (white arrowheads). (C) Coronal CT image at the level of the right ventricle shows similar findings. CT = computed tomography.. ORCID iDs Dongjun Lee https://orcid.org/0000-0003-2177-9212 Min Ji Son https://orcid.org/0000-0002-5602-8315 Seung Min Yoo https://orcid.org/0000-0002-1990-8145 Hwa Yeon Lee https://orcid.org/0000-0002-3643-4113 Charles S White https://orcid.org/0000-0002-9789-7648 Funding The authors received no financial support for the research, authorship, and/or publication of this article. Conflict of Interest The authors have no financial conflicts of interest. Author Contributions Conceptualization: Lee D, Kim IJ, Yoo SM; Formal analysis: Lee D, Kim IJ; Investigation: Lee D, Kim IJ, Son MJ, Yoo SM, Lee HY, White CS; Methodology: Lee HY, Son MJ, White CS; Supervision: Yoo SM; Writing - original draft: Lee D, Kim IJ, Son MJ, Yoo SM, Lee HY, White CS; Writing - review & editing: Lee D, Kim IJ, Son MJ, Yoo SM, Lee HY, White CS.. https://e-kcj.org. Coronary stent infection has several risk factors (i.e., virulence of the pathogen, host response, device properties, and procedural difficulty). The most common cause of coronary stent infection is procedure-related infection from the skin or catheters, often due to Staphylococcus aureus (80%) followed by Pseudomonas aeruginosa (20%).1-3) In previous reports, the primary tool to identify coronary stent infection was the identification of pseudoaneurysm formation on coronary angiography.1-3) However, coronary angiography only visualizes a portion of the overall abscess pocket. In contrast, CT can evaluate the overall extent of coronary stent infection, facilitating proper therapeutic planning. In this regard, the case shows the value of CT in diagnosing complications of coronary stent infection and providing appropriate treatment planning.. REFERENCES 1. Elieson M, Mixon T, Carpenter J. Coronary stent infections: a case report and literature review. Tex Heart Inst J 2012;39:884-9. PUBMED. 2. Del Trigo M, Jimenez-Quevedo P, Fernandez-Golfin C, et al. Very late mycotic pseudoaneurysm associated with drug-eluting stent fracture. Circulation 2012;125:390-2. PUBMED | CROSSREF. 3. Reddy K V C, Sanzgiri P, Thanki F, Suratkal V. Coronary stent infection: interesting cases with varied presentation. J Cardiol Cases 2018;19:5-8. PUBMED | CROSSREF. https://doi.org/10.4070/kcj.2020.0469. 282.
(3)
수치

관련 문서
