Korean Journal of HBP Surgery
□ 원 저 □ Vol. 9, No. 2, June, 2005
113
서 론
특발성 혈소판 감소성 자반증(Idiopathic thrombocytopenic purpura, 이하 ITP) 환자에서 비장 절제술 후 완전 관해는 28%에서 90%로 다양하게 보고되고 있으며 Kojouri 등1에 의하면 그 평균은 66% 정도이다. 이렇게 다양하게 보고되 는 이유는 수술 후 추적 기간의 차이와 완전 관해에 대한 정의의 차이 때문인 것으로 생각한다. 또, 수술 후 어떤 환 자에서 비장 절제술 후 병이 호전되고, 호전된 상태로 유지 될 것인지에 대해서는 아직 정확하게 밝혀진 바가 없는 실 정이다.
이에 저자들은 비장 절제술을 시행한 ITP 환자의 예후 및 그 예측 인자에 대한 규명을 위해 본 연구를 시행하였다.
방 법 1. 대상
1997년 1월부터 2003년 12월까지 서울대학교병원에서 비 장 절제술을 시행 받고 외래 추적이 가능했던 ITP 환자 54 명의 의무 기록을 후향적으로 검토하여 연령, 성별, 진단부 터 수술까지의 기간, 진단 시 혈소판 수치, 수술 전 혈소판
Clinical Outcome and Predictive Factor of Splenec-
tomy in Patients with Idiopathic Thrombocytopenic Purpura
Seong-Yeop Kim, M.D., Jin-Young Jang, M.D., Seong-Sik Han, M.D., Yoo-Seok Yoon, M.D., Youn-Chan Park, M.D.1, Ho-Seong Han, M.D., Sun-Whe Kim, M.D. and Yong-Hyun Park, M.D.
Department of Surgery, Seoul National University College of Medicine, Seoul, 1Department of Surgery, Dankook University College of Medicine, Cheonan, Korea
Purpose: Splenectomy is an important treatment modality for
the patients with idiopathic thrombocytopenic purpura (ITP), but the response rate of splenectomy for ITP patients is vari- able and the predictive factors of the postoperative response are uncertain. The purpose of this study is to investigate the response rate of splenectomy and find the predictive factors of splenectomy in ITP patients.Methods: We reviewed the medical records of 54 consec-
utive patients who underwent splenectomy and were followed up. A positive response to splenectomy was defined as a postoperative platelet count greater than 50,000/μl without medication. We analyzed the following variables to find the predictive factors for splenectomy; age, gender, disease dura- tion, platelet count at diagnosis, preoperative platelet count, early response to steroid, IVIG response, operative method, accessory spleen and postoperative platelet count.Results: The response rate of splenectomy was 60% at the
1st postoperative month, 46% at the 3rd postoperative month and 37% at the 6th postoperative month. The age of the splenectomy responders at the 6th postoperative month was significantly lower than that of the non-responder (33.4±14.5 years versus 48.7±17.1 years, p<0.05). The platelet count at the time of discharge of the splenectomy responders was significantly greater than that of the non-responders (378,429특발성 혈소판 감소성 자반증 환자의 비장 절제술의 결과 및 예측인자
서울대학교 의과대학 외과학교실, 1단국대학교 의과대학 외과학교실 김성엽․장진영․한성식․윤유석․박윤찬1․한호성․김선회․박용현
±272,399/μl versus 191,731±151,435/μl, p<0.05). These results were significant on multivariate analysis.
Conclusion: The response rate of splenectomy is decreased
according to the passage of time during the early postopera- tive period, so long term follow up is important to investigate the predictive factors. Young age for the patients and high platelet count at discharge can be used as the predictive factors for splenectomy in ITP. (Korean J HBP Surg 2005;9:113-116)
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
Key Words: Purpura, Thrombocytopenic, Idiopathic
Splenectomy Prognosis
중심 단어: 비장 절제술, 특발성 혈소판 감소성 자반 증, 예후
책임저자:장진영, 서울시 종로구 연건동 28번지 ꂕ 110-744, 서울대학교 의과대학 외과학교실 Tel: 02-2072-2194, Fax: 02-766-3975
E-mail: jangjy4@snu.ac.kr
114
한국간담췌외과학회지:제 9 권 제 2 호 2005ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ 수치, 부신 피질 호르몬 제제에 대한 초기 반응, 면역글로불
린 투약 시 반응, 수술 방법, 부비장 존재 여부 및 수술 후 혈소판 수치의 변화 등을 조사하였다. ITP의 진단 기준은 말초 혈액에서 혈소판 감소증을 보이고, 골수 천자상 거핵 구 수가 정상이거나 증가되어 있으며, 혈소판 감소의 원인 이 되는 약제의 복용이나 패혈증, DIC 등의 원인 질환이 없 는 경우로 하였다. 비장 절제술 전에 부비장에 대한 검사로 수술 전 복부 초음파나 컴퓨터 단층 촬영, 비장 스캔 중 1개 이상을 시행하였으며 수술 후 비장 절제술에 대해 반응이 좋지 않은 환자들에 대해서는 상기 검사들 중 1개 이상을 다시 반복하여 부비장 존재 여부를 확인하였다.
2. 부신 피질 호르몬 제제, 면역글로불린에 대한 반응의 정의 및 비장 절제술 반응 양성에 대한 정의 수술 전 내과적 치료를 시행할 때 부신 피질 호르몬 제제 에 대한 초기 반응은 투약 시작 후 3개월간 매월 1회 이상 추적 검사한 혈소판 수치가 50,000/μl 이상으로 지속적으로 유지된 경우에 반응 양성으로 정의하였다. 면역 글로불린 에 대한 반응은 면역 글로불린 투약 종료 후에 검사한 혈소 판 수치가 50,000/μl 이상이고, 투약 시작 직전 검사한 혈소 판 수치의 2배 이상일 때 반응 양성으로 정의하였고, 면역 글로불린은 400 mg/kg/일로 4∼5일 간 정주하였다. 비장 절 제술에 대한 반응은 해당 기간까지 매월 1회 이상 추적 검
사한 혈소판 수치가 내과적 치료 없이 50,000/μl 이상으로 계속적으로 유지될 때 반응 양성으로 정의하였다.
3. 통계
통계 처리는 SPSS 12.0 프로그램을 이용하였으며 단변량 분석은 카이제곱 검정(chi square test)과 독립표본 T 검정 (independent-samples T-test)을 사용하였고, 단변량 분석에서 유의하였던 예측 인자로 다변량 분석을 시행하였다. 다변 량 분석의 방법은 이분형 로지스틱 회귀분석(binary logistic regression model)을 사용하였다.
결 과 1. 환자군
환자의 평균 연령은 42.7세(15∼74세)였으며 남자 13명, 여자 41명으로 남녀 성비는 1:3.2였다. 수술 후 외래 추적 기간은 평균이 32.0개월(1∼88개월)이었으며 진단부터 수 술까지의 기간은 평균이 44.6개월(1∼300개월)이었고, 이 중 진단 시부터 수술까지 1년 이상 경과하였던 환자는 56%
(n=30)였다. 수술 방법은 복강경 수술 26예, 개복술 28예였 다. 개복술 중 1예에서는 복강경 수술 시도 중 출혈로 개복 술로 전환한 경우였다.
2. 비장절제술 후 반응률 및 수술 전후 예측인자 수술 후 1개월째 비장절제술에 대한 반응 양성인 경우는 60% (n=32), 3개월째에는 46% (n=23), 6개월째에는 37% (n=
18)로 시간이 흐를수록 감소하는 양상을 보였다.
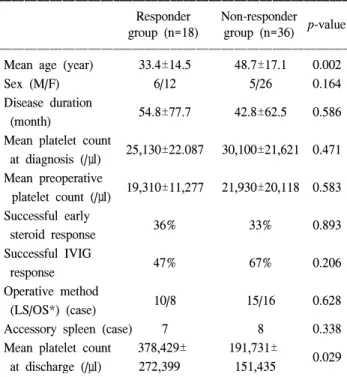
6개월까지 비장 절제술 반응 양성인 환자들과 반응 음성 인 환자들의 연령, 성별, 진단부터 수술까지의 기간, 진단 시 혈소판 수치, 수술 전 혈소판 수치, 부신 피질 호르몬 제 제에 대한 초기 반응, 면역 글로불린 투약 시 반응, 수술 방 법, 부비장 존재 여부 및 수술 후 혈소판 수치의 변화 등을 비교하였을 때 단변량 분석에서 통계적으로 유의한 차이를 보였던 것은 연령, 퇴원 시 혈소판 수치였으며(p<0.05) (Table 1), 이 두 가지 인자는 다변량 분석에서도 유의한 차 이를 보였다(p<0.05)(Table 2).
Table 1. Univariate analysis of perioperative variables of splenec- tomy responder and non-responder group at the 6th postoperative month
ꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚ Responder Non-responder
p-value group (n=18) group (n=36)
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ Mean age (year) 33.4±14.5 48.7±17.1 0.002
Sex (M/F) 6/12 5/26 0.164
Disease duration
54.8±77.7 42.8±62.5 0.586 (month)
Mean platelet count
25,130±22.087 30,100±21,621 0.471 at diagnosis (/μl)
Mean preoperative
19,310±11,277 21,930±20,118 0.583 platelet count (/μl)
Successful early
36% 33% 0.893
steroid response Successful IVIG
47% 67% 0.206
response Operative method
10/8 15/16 0.628
(LS/OS*) (case)
Accessory spleen (case) 7 8 0.338
Mean platelet count 378,429± 191,731±
0.029 at discharge (/μl) 272,399 151,435
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
*LS/OS = laparoscopic splenectomy/open splenectomy.
Table 2. Multivariate analysis of perioperative variables of splenec- tomy responder and non-responder group at the 6th postoperative month
ꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚ Responder Non-responder
p-value group (n=18) group (n=36)
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ Mean age (year) 33.4±14.5 48.7±17.1 0.002 Mean platelet count 378,429± 191,731±
0.031 at discharge (/μl) 272,399 151,435
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
김성엽 외:특발성 혈소판 감소성 자반증 환자의 비장 절제술의 결과 및 예측인자 115 ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
3. 합병증
수술 후 합병증은 4예 있었으며 복강경 수술에서 수술 후 출혈과 수술 부위 조직액 저류가 한 환자에서 병발하였고, 개복술에서 조직액 저류와 창상 감염이 각각 1예씩 있었다.
수술 후 출혈이 있었던 증례에서는 회복실에서 바로 출혈 이 발견되어 응급 개복술을 시행하여 비장이 있던 위치에 서 출혈중인 혈관을 결찰하였다. 수술과 관련한 사망은 발 생하지 않았다.
4. 수술 후 진단된 부비장
수술 전 부비장이 진단되지 않았던 3예의 환자에서 수술 후 부비장이 진단되었으며 이 중 1예는 환자와 보호자가 재수술을 거부하여 부신 피질 호르몬 제제와 Danazole을 투 약하여 혈소판 수치가 40,000/μl 전후로 유지되고 출혈 성 향이 없어 외래에서 추적 관찰 중이며 나머지 2예는 재수술 을 시행하여 부비장을 제거하였다. 이 중 1예는 부비장 제 거 후에도 계속 투약하였으나 혈소판 수치가 50,000/μl 이 상으로 유지되지 않고 있고, 나머지 1예는 투약을 계속할 경우, 혈소판 수치가 50,000/μl 이상으로 유지되나 투약을 중단하면 다시 혈소판 수치가 떨어져 계속 투약 중이다.
고 찰
비장 절제술 후 완전 관해의 정의는 보고자에 따라 다른 데, 대체로 수술 후 내과적 치료 없이 혈소판 수치가 150,000/μl 이상으로 유지되는 것을 기준으로 하거나,2-4 100,000/μl 내지5-9 50,000/μl 이상으로10 유지되는 것을 기 준으로 하고 있다. Schwartz 등4은 수술 후 완전 관해의 기준 을 내과적 치료 없이 혈소판 수치가 150,000/μl 이상으로 유지될 때로 하였으며, 수술 후 장기 추적 관찰(5∼10.5년) 하였을 때 57% (n=32)의 완전 관해율을 보였다고 보고하였 다. Radaelli 등7은 완전 관해의 혈소판 수치를 100,000/μl을 기준으로 하여 추적 관찰(13∼450개월)하였을 때 67.7%
(n=44)의 완전 관해율을 보고하였으며, Kumar 등10은 50,000/
μl을 기준으로 1년간 추적 검사하였을 때 완전 관해율을 73.5% (n=78)로 보고하였다.
이번 연구에서 비장 절제술 후 혈소판 수치를 추적 검사 하였을 때 1개월째에는 비장절제술 반응 양성이 60%, 3개 월째에는 46%, 6개월째에는 37%로 시간이 흐를수록 반응 률이 떨어지는 것이 확인되었다. Kumar 등10은 수술 후 투 약 없이 혈소판 수치가 50,000/μl 이상으로 유지되었던 환 자들 113명 중 19명이 3개월만에 재발하였고, 6개월만에 25 명이 재발하였다고 보고하였으며 대부분의 재발은 1년 이 내에, 평균 3개월만에 일어났다고 하였다. 이러한 결과는 저자들의 연구에서도 비슷한 양상을 보였다. 6개월째 재발 이 없었던 환자들 중 수술 후 1년째까지 외래에서 추적한
14명은 한 명도 재발이 없었고 3년까지 추적한 9명의 환자 중에도 재발이 없었다. 그러므로 ITP 환자의 수술 후 예측 인자를 확인하기 위해서는 최소한 1년 이상의 추적 관찰이 필요할 것으로 생각된다.
ITP 환자에서 비장 절제술 후 결과에 대한 예측 인자는 보고자들마다 다양한데 연령이 가장 많은 보고에서 받아들 여지고 있는 예측 인자이며,1,8 수술 전 혈소판 수치와 면역 글로불린에 대한 반응, 부신피질 호르몬 제제에 대한 초기 반응, 진단부터 수술까지의 기간 등이 보고되고 있다.6 이번 연구의 환자 군의 수술 전 혈소판 수치의 평균은 21,630/μl 으로 완전 관해율을 60∼90% 정도로 보고하였던 다른 보고 보다 낮았으며,5,6,10 진단부터 수술까지의 기간의 평균도 44.6개월로 더 길고,2,4,10,11 환자들의 평균 연령도 42.7세로 더
높았다.2,4,5,7,8 이번 연구의 환자 군이 다른 보고들의 환자 군
에 비해 수술 후 반응이 좋지 않은데 그 이유는 앞서 나열한 좋지 않은 예측 인자가 많았기 때문으로 생각한다.
비장 절제술 중 부비장이 발견될 확률은 15∼30%까지 보 고되고 있으며, 수술 후 재발의 중요한 원인 중 하나로 수술 중 발견하지 못한 부비장이 지적되고 있다.12,13 이번 연구에 서도 수술 중 발견하지 못한 부비장이 수술 후 발견된 경우 가 3예 있었는데 모두 수술 전 시행한 복부 초음파나 컴퓨 터 단층 촬영 또는 비장 스캔에서 부비장을 발견하지 못한 경우이며, 수술 후 혈소판 수치가 상승하지 않아 다시 시행 한 복부 초음파와 컴퓨터 단층 촬영 및 비장 스캔에서 부비 장을 발견하여 2예는 재수술을 시행하고 1예는 내과적 치 료로 혈소판 수치가 40,000/μl 정도로 유지되어 외래에서 추적 관찰 중이다. 상기 3예 중 수술 전 스캔을 시행하였던 경우가 2예였으며 복부 초음파를 시행하였던 경우가 1예였 다. 수술 중 부비장이 확인되고 조직학적 검사에서 확인되 었는데도 수술 전 시행한 검사에서 부비장을 발견하지 못 한 경우는 컴퓨터 단층촬영에서 16% (n=4), 비장 스캔에서 28% (n=8), 복부 초음파에서 15% (n=2)였다. 이번 연구의 결과에서는 복부 컴퓨터 단층 촬영이나 초음파가 수술 전 부비장을 진단하는 것에 있어 비장 스캔보다 효율적인 방 법일 수 있음을 시사하였으며 이에 대한 연구를 통해 부비 장의 존재 여부 및 위치를 수술 전에 정확하게 파악할 수 있는 진단 방법의 개발이 필요할 것으로 생각한다.
결론적으로 ITP 환자에서 비장 절제술 시 반응률 및 예후 에 대한 예측 인자를 평가하기 위해서는 1년 이상의 장기적 인 추적 관찰이 필요하다. 그리고 이번 연구에서는 적은 나 이와 퇴원 시 높은 혈소판 수치가 수술 후 좋은 예후를 예 측할 수 있는 인자로 규명되었다. 또한 환자에게 최소한의 침습으로 좋은 효과를 기대할 수 있는 복강경 비장 절제술 이 보편화된 현재 시점에서 반응이 없는 환자에게 스테로 이드를 포함한 장기적인 내과적 치료로 인해 비장 절제술 의 치료 시기를 늦추는 것은 바람직하지 않다고 생각하며, 향후 비장 절제술과 내과적 치료의 시기에 관한 전향적 연
116
한국간담췌외과학회지:제 9 권 제 2 호 2005ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ 구를 통해 이상적인 수술 시기를 찾는 연구가 필요할 것으
로 생각한다.
참 고 문 헌
1) Kojouri K, George JN, Terrel DR, Vesely SK. Splenectomy for adult patients with idiopathic thrombocytopenic purpura: a systematic review to assess long-term platelet count response, prediction of response, and surgical complications. Blood 2004;104:2623-2634.
2) Katkhouda N, Grant SW, Mavor E, et al. Predictors of re- sponse after laparoscopic splenectomy for immune thrombocy- topenic purpura. Surg Endosc 2001;15:484-488.
3) Meyer G, Wichmann MW, Rau HG, Hiller E, Schildberg FW.
Laparoscopic splenectomy for idiopathic thrombocytopenic purpura. 1-year follow-up study. Surg Endosc 1998;12:1348- 1352.
4) Schwartz J, Leber MD, Gillis S, Giunta A, Eldor A, Bussel JB. Long term follow-up after splenectomy performed for im- mune thrombocytopenic purpura (ITP). Am J Hematol 2003;
72:94-98.
5) Bourgeois E, Caulier MT, Delarozee C, et al. Long-term fol- low-up of chronic autoimmune thrombocytopenic purpura re- fractory to splenectomy: a prospective analysis. Br J Haematol 2003;120:1079-1088.
6) Duperier T, Brody F, Felsher J, Walsh M, Rosen M, Ponsky
J. Predictive factors for successful laparoscopic splenectomy in patients with immune thrombocytopenic purpura. Arch Surg 2003;139:61-66.
7) Radaelli F, Faccini P, Goldaniga M, et al. Factors predicting response to splenectomy in adult patients with idiopathic thrombocytopenic purpura. Haematologica 2000;85:1040-1044.
8) Fabris F, Tassan T, Ramon R, et al. Age as the major predic- tive factor of long term response to splenectomy in immune thrombocytopenic purpura. Br J Haematol 2001;112:637-640.
9) Lee BW, Ahn SI, Lee KY, et al. Laparoscopic splenectomy in patients with idiopathic thrombocytopenic purpura. J Korean Soc Endosc Laparosc Surg 2002;4:32-37.
10) Kumar S, Diehn FE, Gertz MA, Tefferi A. Splenectomy for immune thrombocytopenic purpura: long-term results and treatment of postsplenectomy relapses. Ann Hematol 2002;81:
312-319.
11) Gadenstatter M, Lamprecht B, Klingler A, Wetscher GJ, Greil R, Schmid T. Splenectomy versus medical treatment for idio- pathic thrombocytopenic purpura. Am J Surg 2002;184:606- 610.
12) Park JH, Choi GS, Sohn SK, Yun YK, Jun SH. Laparoscopic splenectomy for chronic idiopathic thrombocytopenic purpura.
J Korean Surg Soc 2000;59:101-107.
13) Morris KT, Horvath KD, Jobe BA, Swanstrom LL. Laparo- scopic management of accessory spleens in immune throm- bocytopenic purpura. Surg Endosc 1999;13:520-522.