Received December 3, 2013, Revised December 17, 2013, Accepted December 17, 2013 Corresponding author: Sungtae Koo
Division of Meridian and Structural Medicine, School of Korean Medicine, Pusan National University, Mulgeum-eup, Yangsan 626-870, Korea Tel: +82-51-510-8474 Fax: +82-51-510-8439, E-mail: [email protected]
This research was supported by Basic Science Research Program through the National Research Foundation of Korea(NRF) funded by the Ministry of Education, Science and Technology(2010-0003928).
*These authors contributed equally to this work.
CCThis is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/ by-nc/3.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Mutual Inhibitory Effects of Electroacupuncture Applied to Combination of ST36 and PC7
in the Rat Model of Arthritis
Yeojung Kim1*, Yunjung Jung1*, Chang-Hyung Lee2, Sungtae Koo1
1Division of Meridian and Structural Medicine, School of Korean Medicine, Pusan National University,
2Department of Rehabilitation Medicine, Pusan National University School of Medicine
흰쥐 관절염 모델에서 족삼리와 대릉 배오 전침의 상호억제 효과
김여정1*ㆍ정연정1*ㆍ이창형2ㆍ구성태1
1부산대학교 한의학전문대학원 경락구조의학부, 2부산대학교 의학전문대학원 재활의학과
Objectives : We examined mutual inhibitory effects of combined acupoints in arthritic pain induce by carrageenan(CA). Electro- acupuncture(EA) is considered a potentially useful treatment for arthritis. Although the analgesic effect of acupuncture is well documented, little is understood about its biological basis. There are many previous studies of positive effect of combined acupoint, this study was conducted to see the mutual inhibitory effects produced by combined acupoint(ST36 and PC7) on arthritic rats. Methods : For the induction of inflammatory pain rat model, CA was injected into the knee joint cavity. There are four groups;
EA was applied to bilateral PC7 acupoints(PC7 group), ST36 acupoints(ST36 group), and both PC7 and ST36 acupoints(ST36+PC7 group) except for the control group. The pain level were assessed to determine the change in weight bearing force. We also examined the COX-2 expression in dorsal horn using immunohistochemistry and western blot analysis. Results : The ST36+PC7 group data showed the significant reduction of weight bearing force and the induction of COX-2 protein expression compared with the ST36 group. Conclusions : Simultaneous EA applied to the ST36 and PC7 acupoints reduced the analgesic effect of the ST36 group on knee inflammatory pain.
Key words : carrageenan induced arthritis, electroacupuncture, weight bearing, COX-2
Introduction
Electroacupuncture is considered a potentially useful treat- ment for arthritis, also many studies have reported the effect of EA on inflammatory pain1-4). The EA analgesia is a com-
plicated neuronal process mediated by many different neuro- transmitters and mediators, such as endogenous opioids5,6), adenosine7), many inflammatory mediators and other bio- active substances.
EA at the ST36 acupoint is well used in inflammatory pain
model and the analgesic effect has been revealed7-9). In clinical situations electroacupuncture(EA) on ST36 acupoint is practiced for the treatment of osteoarthritic(OA) pain.
Traditionally, simultaneous acupuncture to two or more acu- points including ST36 acupoint has been used to improve acupuncture induced effects10-12). But, According to frequen- cy of EA, location of combined acupoints, number of com- bined acupoints10,11,13,14)
, studies showed various effect.
We asked whether there is mutual inhibitory effects of combined acupoints. We had chosen the PC7 acupoint as a nominee having inhibitory effect on analgesic action of ST36 acupoint throughout pre-experiment. We investigated the change of pain behavior using Weight bearing Test and the changes in the expression of a number of mediator in the spinal cord using COX-2 western blot analysis and immuno- reactive analysis.
The aim of this study was to investigate that the possibility of negative effect of combined acupoints are related with the analgesic effects of EA.
Materials and Methods
1. Experimental animals
The experiments were performed on 16 young adult male Sprague-Dawley rats(200∼250 g, Hyochang Science, Daegu, Korea). The animals were housed in pairs in plastic cages with soft bedding and were provided access to food and water ad libitum under a reversed 12/12 hour light-dark cycle(dark cycle: 8:00 A.M.∼8:00 P.M.). All animals were acclimated for 7 days before beginning the experiments. All experimental procedures were carried out in accordance with the Animals(Scientific Procedures) Act 2008(Korea) and all complied with the recommendations of the National Institute of Health’s Guide for the Care and Use of Laboratory Animals. The study was also approved by the Ethics Commi- ttee on Animal Research at Pusan National University (PNU-2012-0085). For peripheral inflammation induction, the animals were injected with 50 μl of 2% lambda CA(Sigma, St. Louis, USA) in 0.9% normal saline into the synovial cavity
of the right knee joint under isofluorane anesthesia(3% to induce and 1.5% to maintain in mixed N2O/O2 air).
2. Experimental procedures
All animals received the carrageenan(CA) treatment. The rats were divided randomly into four treatment groups: the control group(n=7, without EA treatment), the ST36 group (n=7, with EA treatment at ST36), the PC7 group(n=7, with EA treatment at PC7), and the ST36+PC7 group(n=7, with EA treatment at ST36 and PC7 simultaneously).
3. Electroacupuncture treatment
For EA stimulus, two stainless steel acupuncture needles, 0.25 mm in diameter and 40 mm in length, were inserted into specific acupuncture points[ST36, PC7] at a depth of 5 mm and electrical stimulation was applied by a Pulsemaster Multi-channel Stimulator SYS-A300(World Precision Instru- ments, Inc., Berlin, Germany). EA treatment was performed two times which were right after 2% CA injection and 2 hours after CA injection on the bilateral sides with a stimulus of 1 mA and 10 Hz for 30 min. The procedure was performed with the animals under gaseous anesthesia with iso-fluorane in mixed N2O/O2 air. ST36 acupoint is on the anterior aspect of the leg, lateral to the tibial tubercle on the midway of anterior tibialis muscle15). PC7 acupoint is on the anterior aspect of the forearm, between the tendons of the palmaris longus and the flexor carpiradialis tendon, on the palmar wrist crease.
4. Behavioral test: weight bearing measurements To confirm that CA-induced inflammatory pain occurred in the rat knee, we measured the weight-bearing force(WBF) ratio using a weight-bearing device(Acculab Pocket pro 250-B, PA, USA) 2 days before and 1, 4, 8 h after the injection of CA. The detailed procedure used to measure the WB ratio is explained elsewhere16).
5. Western blotting
Lumbar enlargement segments of the spinal cord were removed, The L4-5 spinal cord segment was first isolated.
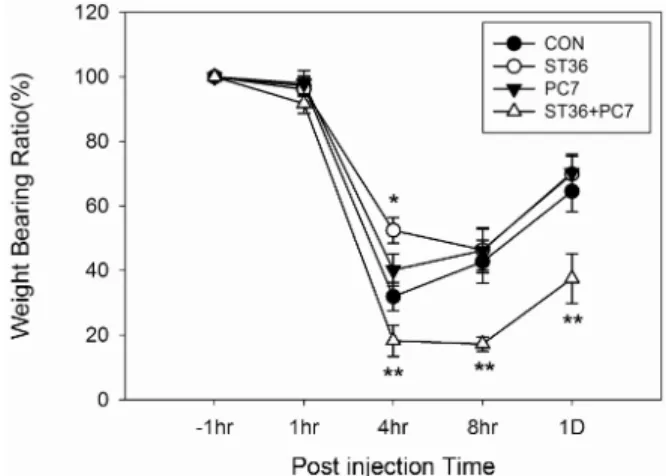
Fig. 1. Effect of electroacupuncture on weight bearing of rats with arthritis.
The ratio of weight bearing value to body weight were plotted.
Data are expressed as percent changes compared with responses before the induction of inflammatory pain. In control group, Weight Bearing Force(WBF) was reduced 4 h after CA injection.
In ST36 group, EA treatment to ST36 suppressed CA-induced pain at 4 h compared with control group(*ST36 vs. CON, p<0.05). In contrast, combined EA treatment to ST36 and PC7 did not suppressed CA-induced pain at 4h after CA injection(**ST36 vs.
ST36+ PC7, p<0.001), #CON : control group(n=7), PC7: EA to PC7(n=7), ST36 : EA to ST36(n=7), ST36+PC7: EA to both ST36 and PC7(n=7).
The dorsal horns were homogenized in 50 mM Tris/HCl, 1 mM EDTA, pH 7.4, PIC(protease inhibitor cocktail, Roche Inc.) 250 mM sucrose, 1 mM DTT and grided by using Pellet pestle(sigma-aldrich, USA). Following a 30 min inverting in cold(4oC), the mixture was centrifuged at 13,000 g for 20 min in a(4oC), then the supernatant was taken. Thus obtained supernatant was quantified by BCA protein assay and then was submitted to SDS-polyacrylamide gel electrophoresis(5%
stacking, 12% running gel) and transferred to nitrocellulose membranes(AmershamTM HybondTM-ECL, CE Healthcare, UK).
The membrane was shaken for 1 h at room temperature in Tris-buffered saline(TBST) pH 7.6 and 5% skim milk and incubated overnight at 4oC with Primary antibodies; the COX-2(mouse) polyclonal antibody(Cayman Chemical, Ann Arbor, MI, USA) diluted 1:1,000 in 3% BSA/TBST. This was followed by application of antimouse secondary antibody conjugated to horseradish peroxidase(Thermo scientific, Rock- ford, USA). COX-2 protein was detected by chemilumi- nescence using by ImageQuant LAS4000(GE Healthcare, Bu- ckinghamshire, England).
6. Immunohistochemistry
The L4-6 segments of the spinal cords were fixed in 4%
paraformaldehyde and immersed in 30% gradient sucrose for 48 h at 4oC for cryoprotection. Frozen tissue were sectioned at 30μm-thick on a freezing microtome(CM3050S, Leica biocyctems, Wetzlar, Germany). All the sections were blocked with CAS-block(Invitrogen-Molecular Probes, Inc., Camorillo, CA, USA) for 9 mins at room temperature(RT) after being pretreated with 2% H2O2 in PBS for 20 min and incubated with mouse anti-COX-2 at a dilution 1:500(Cayman Che- mical, Ann Arbor, MI, USA) following primary antibodies overnight in PBS at 4oC. After washed with PBS containing Tween-20(PBST), the sections were incubated with the secondary antibody, biotinylated goat anti-mouse IgG(Vector Laboratories Inc., Burlingame, CA, USA) or biotinylated goat anti-rabbit IgG(Vector Laboratories Inc., Burlingame, CA, USA) for 2 h at RT and then washed with PBST. Immu- noreactivity was visualized by incubating the sections in a solution consisting of 0.05% 3,3-diaminobenzidine(DAB) for
approximately 1 min 40 sec. The stained sections were exa- mined with Zeiss AxioScope A1 microscope, and images were captured with a Axiocam ICc3 camera.
7. Statistical analysis
The data is expressed as the mean±standard error of mean (SEM). Statistical analyses were conducted using a student’s t-test or by one way analysis of variance(ANOVA) followed by a Holm-Sidak post-hoc test. p values <0.05 were con- sidered significant.
Results
1. Weight bearing measurements
As known in the published paper, we showed that the analgesic effect of EA treatment appeared 4 h after CA injection at ST36 group compared with control group. The PC7 group did not show any effect on pain behavior, there was no great difference between the control group and PC7
Fig. 2. Quantitative analysis of COX-2 in spinal cord using Western blotting.
(A)Representitive immunoblots images for COX-2 protein from spinal cord. (B)Densitometric quantifications of band intensities of COX-2. In ST36 group, there was statistically significant reduction of COX-2 protein compared with control group(con vs.
st36 p<0.050). In ST36+PC7 group, COX-2 protein of was increased in contrast with ST36 group(st36+PC7 vs. st36 p< 0.050). *NOR: no injection, no EA treatment, CON: control group (n=4), PC7: EA to PC7(n=4), ST36: EA to ST36(n=4), ST36+PC7:
EA to both ST36 and PC7(n=4). Analysis was done using a one-way ANOVA followed by Holm-Sidak post-hoc multiple comparison test. A p value of less than 0.05 was considered to be statistically significant.
Fig. 3. COX-2 immunohistochemistry in the dorsal horn 4h after CA injection.
(A)CON: control group(n=5), (B)PC7: EA to PC7(n=5), (C)ST36: EA to ST36(n=5), (D)ST36+PC7: EA to both ST36 and PC7(n=5).
(E)The difference of COX-2 immunoreactivity in the ipsilateral spinal cord(*ST36 vs. ST36+ PC7, p<0.05). Scale bar=100μm.
group in weight bearing force reduction. A significant weight bearing force reduction at 4 hr after injection was happened at the ST36+PC7 group in which the recovery(1 Day) was delayed as shown compared to other groups. There were statistically significant differences in response between the ST36 and ST36+PC7 group(Fig. 1). Analysis was done using a one-way ANOVA followed by Holm-Sidak post-hoc multiple comparison test. A p value of less than 0.05 was considered to be statistically significant.
2. Western blot analysis
We determined the induction of COX-2 protein in the spinal cord 4h after the CA injection using Western Blot analysis(Fig. 2). In the control group, COX-2 protein was
up-regulated as expected compared with normal group(NOR:
no injection, no EA treatment). The COX-2 protein of the ST 36 group was down-regulated compared with control group.
The PC7 group also was up-regulated as control group, but there were statistically no significant differences in response between the PC7 and CON group. In ST36+PC7 group, the expression of COX-2 protein increased compared with ST36.
There were statistically significant differences in response between the ST36 and ST36+PC7 group.
3. Immunohistochemistry
To identify COX-2 expression in ipsilateral dorsal horn at 4 hr after CA injection, we conducted immunohistochemistry.
Our data showed that COX-2 immunoreactivity of ST36+PC7 group was increased compared with ST 36 group(Fig. 3).
There were statistically significant differences in response between the ST36 and ST36+PC7 group.
Discussion
Physiological pain is initiated by specialized sensory nociceptor fibers innervating peripheral tissues and activated only by noxious stimuli. The sensory inflow generated by nociceptors activates neurons in the spinal cord which pro- ject to the cortex via a relay in the thalamus, eliciting pain.
Pain has multiple mechanisms but each of which is subject to or an expression of neural plasticity-the capacity of neu- rons to change their function, chemical profile, or structure.
Neural plasticity in primary sensory and dorsal horn neurons is related to the pathogenesis of pain. Pain hypersensitivity is an expression of neuronal plasticity, the duration of which is determined by the particular patterns of activation, mo- dulation, or modification occurring. These process is medi- ated by many different neurotransmitters and modulators which are the target of many clinical treatment17).
The nociceptor input also activates the inhibitory noci- ceptor transmission including neurotransmitters released from interneurons within spinal cord and supraspinal sources.
The transmission of nociceptive information is subject to modulation at all levels of the neuraxis, from the dorsal horn rostrally. Afferent impulses arriving in the dorsal horn initiate inhibitory mechanisms that limit the effect of subsequent impulses. Inhibition occurs through local inhibitory inter- neurons and descending pathways from the brain. A model of how this interaction occurs in relation to pain processing was proposed by Melzack and Wall in 1965, and has been termed the ‘gate theory’18). Although the gate theory does not completely resolve the specific mechanisms responsible for pain processing, it has clinical implications for modulation of spinal sensitization and it has been the possible explanation of acupuncture effects.
The effect of acupuncture reducing pain is a complicated neuronal process mediated by many different neurotran- smitters and mediators. There are many experimental evi- dences that many signaling molecules such as opioid pe- ptides, serotonin, noradrenalin, dopamine, glutamate, γ- amino-butyric acid, nerve growth factor(NGF), many infla- mmatory mediators and other bioactive substances may be
involved in acupuncture analgesia. The analgesic effect of acupuncture is decreased at the supraspinal level when opioid receptor antagonists are given4,16). The blocking of serotonin receptors by serotonin synthesis inhibitors induced inhibition of acupuncture analgesia5,19). The analgesic effects of electroacupuncture(EA) are blocked by administering the precursor of noradrenalin, whereas it is potentiated by admi- nistering intrathecally5). The activations of Dopamin D1 or D2 receptor is unfavourable to the expression of EA after ef- fect20). EA inhibits cycloxygenase-2 up-regulation in rat spinal cord after spinal nerve ligation21), and EA had a long lasting and better analgesic effect than COX-2 inhibitor in reducing neuropathic hypersensitivity22). EA modulates NGF in the pe- ripheral nervous system, being effective for the treatment of diabetic polyneuropathy(DPN) symptoms23). EA counteracted the NGF-driven variation of substance P and transient re- ceptor potential vanilloid type 1(TRPV1) response in both hind-paw skin as well as the corresponding dorsal root ganglia24). Render it down, EA-produced antihyperalgesia is mainly mediated by sensory nerve path-ways involving both spinal and supraspinal mechanisms10).
Besides, the effect of simultaneous acupuncture to two or more acupoints has been reported constantly. Han JS repor- ted that a greater increase in pain threshold was produced when both LI4 and ST36 acupoints were stimulated simu- ltaneously with acupuncture as compared with the results when either one of these two points was stimulated alone10). In addition, there is a report with no synergic effect that simultaneous EA applied to the SI6 and ST36 acupoints produced no synergic interaction, therefore has no beneficial effect for ankle-sprained pain compared to individual EA14).
Our results also showed EA on rat ST36 acupoint relieved pain and down-regulated COX-2 enzyme level in rat spinal cord in comparison with control group. But simultaneous EA of ST36 and PC7 points worsened hyperalgesia, induced COX-2 enzyme in spinal dorsal horn 4 hr after CA injection and hindered the recovery of inflammatory pain 1 day after injection. This results suggested simultaneous EA applied to the several acupoints could produce no synergic interaction, therefore had no beneficial effect and some acupoints com-
bination could have harmful effects to treat specific site’s pain. This might be the clue that according to combined acu- points EA treatment have various effects of inducing neuro- transmitters, modulators on injury sites. In this study, the potential of unexpected effects derived from combination of acupoints suggests the requirement of more specific and delicate acupunctural treatment. Additionally, we propose well designed further studies are necessary to identify the related substances and mechanisms.
Acknowledgements
This research was supported by Basic Science Research Program through the National Research Foundation of Korea(NRF) funded by the Ministry of Education, Science and Technology(2010-0003928).
References
1. Baek YH, Choi DY, Yang HI, Park DS. Analgesic effect of elec- troacupuncture on inflammatory pain in the rat model of colla- gen-induced arthritis: mediation by cholinergic and serotoner- gic receptors. Brain Res. 2005 ; 1057 : 181-5.
2. Choi BT, Kang J, Jo UB. Effects of electroacupuncture with dif- ferent frequencies on spinal ionotropic glutamate receptor ex- pression in complete Freund's adjuvant-injected rat. Acta Histochem. 2005 ; 107 : 67-76.
3. Fu X, Wang YQ, Wu GC. Involvement of nociceptin/orphanin FQ and its receptor in electroacupuncture-produced anti-hy- peralgesia in rats with peripheral inflammation. Brain Res. 2006 ; 1078 : 212-8.
4. Zhang RX, Lao L, Wang L, Liu B, Wang X, Ren K, et al.
Involvement of opioid receptors in electroacupuncture-pro- duced anti-hyperalgesia in rats with peripheral inflammation.
Brain Res. 2004 ; 1020 : 12-7.
5. Han JS, Terenius L. Neurochemical basis of acupuncture analgesia. Annu Rev Pharmacol Toxicol. 1982 ; 22 : 193-220.
6. Taguchi R, Taguchi T, Kitakoji H. Involvement of peripheral
opioid receptors in electroacupuncture analgesia for carra- geenan-induced hyperalgesia. Brain Res. 2010 ; 1355 : 97-103.
7. Goldman N, Chen M, Fujita T, Xu Q, Peng W, Liu W, et al.
Adenosine A1 receptors mediate local anti-nociceptive effects of acupuncture. Nat Neurosci. 2010 ; 13 : 883-8.
8. Chen WH, Hsieh CL, Huang CP, Lin TJ, Tzen JT, Ho TY, et al.
Acid-sensing ion channel 3 mediates peripheral anti-hyper- algesia effects of acupuncture in mice inflammatory pain.
Journal of Biomedical Science. 2011 ; 18 : 82.
9. Koo ST, Park YI, Lim KS, Chung K, Chung JM. Acupuncture an- algesia in a new rat model of ankle sprain pain. Pain. 2002 ; 99 : 423-31.
10. Ulett GA, Han S, Han JS. Electroacupuncture: mechanisms and clinical application. Biol Psychiatry. 1998 ; 44 : 129-38.
11. Baek K-W, Ko E-S, Min K-I, Park D-s. The analgesic effect of combined electroacupuncture at Hoku(LI4) and Zusanli(ST36) using TFL. The Journal of Korean Acupuncture & Moxibustion Society. 2001 ; 18 : 76-87.
12. Gao YH, Chen SP, Wang JY, Qiao LN, Meng FY, Xu QL, et al.
Differential proteomics analysis of the analgesic effect of elec- troacupuncture intervention in the hippocampus following neuropathic pain in rats. BMC Complementary and Alternative Medicine. 2012 ; 12 : 241.
13. Taechaarpornkul W, Suvapan D, Theppanom C, Chanthip- waree C, Chirawatkul A. Comparison of the effectiveness of six and two acupuncture point regimens in osteoarthritis of the knee: a randomised trial. Acupunct Med. 2009 ; 27 : 3-8.
14. Cho Hs, Gwak Ms, Lee SY, Hahm TS. The effect of simultaneous electroacupuncture on ankle sprain pain in rats. Korean J Anesthesiol. 2007 ; 52 : 566-70.
15. Koo ST, Kim SK, Kim EH, Kim JH, Youn DH, Lee BH, et al.
Acupuncture point locations for experimental animal studies in rats and mice. Korean Journal of Acupuncture. 2010 ; 27 : 75-86.
16. Yang EJ, Koo ST, Kim YS, Lee JE, Hwang HS, Lee MS, et al.
Contralateral electroacupuncture pretreatment suppresses carrageenan-induced inflammatory pain via the opioid-mu receptor. Rheumatology International. 2011 ; 31 : 725-30.
17. Woolf CJ, Salter MW. Neuronal plasticity: increasing the gain in pain. Science. 2000 ; 288 : 1765-9.
18. Dickenson AK. Gate control theory of pain stands the test of time. British Journal of Anaesthesia. 2002 ; 88 : 755-7.
19. Li A, Wang Y, Xin J, Lao L, Ren K, Berman BM, et al. Electroacu- puncture suppresses hyperalgesia and spinal Fos expression by activating the descending inhibitory system. Brain Res. 2007 ; 1186 : 171-9.
20. Cai B, Huang X, Wang G, Mo W. [Potentiation of electro- acupuncture analgesia on visceral pain by metoclopramide and its mechanism]. Zhen Ci Yan Jiu. 1994 ; 19 : 66-70, 4.
21. Lau WK, Chan WK, Zhang JL, Yung KK, Zhang HQ. Electroacu- puncture inhibits cyclooxygenase-2 up-regulation in rat spinal cord after spinal nerve ligation. Neuroscience. 2008 ; 155 :
463-8.
22. Lau WK, Lau YM, Zhang HQ, Wong SC, Bian ZX. Electroacu- puncture versus celecoxib for neuropathic pain in rat SNL model. Neuroscience. 2010 ; 170 : 655-61.
23. Nori SL, Rocco ML, Florenzano F, Ciotti MT, Aloe L, Manni L.
Increased nerve growth factor signaling in sensory neurons of early diabetic rats is corrected by electroacupuncture. Evid Based Complement Alternat Med. 2013 ; 2013 : 652735.
24. Aloe L, Manni L. Low-frequency electro-acupuncture reduces the nociceptive response and the pain mediator enhancement induced by nerve growth factor. Neurosci Lett. 2009 ; 449 : 173-7.
국문초록
목적 : Carrageenan(CA)으로 유발시킨 슬관절염 동물 모델에서 족삼리와 대릉을 배오한 전침의 효과를 알아보기 위해 실험을 수행하였다.
두 개 이상의 경혈에 동시에 자침함으로써 상승작용을 일으키는 연구는 많이 보고되었으나, 본 연구에서는 배합한 경혈(족삼리와 대릉)에 의
한 전침 진통 작용의 감쇄 효과가 발생할 수 있는지에 대해 알아보고자 하였다. 방법 : CA을 흰쥐의 슬관절강 내에 주입하여 염증성 통증을
유발시켰다. 실험동물을 임의로 4군으로 배정하였다; PC7 군: 양쪽 상지 대릉 전침 군, ST36 군: 양쪽 하지 족삼리 전침 군, ST36+PC7 군:
양쪽 상지 대릉과 양쪽 하지 족삼리 전침 군, CON: 무처치군. 통증 정도를 측정하기 위해서 weight bearing force의 변화를 측정하였고, 척수 의 후각에 유도된 COX-2 발현을 측정하기 위해 면역조직화학법과 western blot 분석을 실시하였다. 결과 : ST36+PC7군은 ST36군과 비교 하여, 행동실험에서는 weight bearing force가 유의하게 감소하였고, 면역조직화학법과 western blot 분석에서는 COX-2 발현이 상대적으
로 유의하게 증가하였다. 결론 : 이상의 실험결과를 통하여 족삼리와 대릉을 배오한 전침 자극은 슬관절염 모델에서 족삼리 전침의 진통 효과
를 감소시킴을 알 수 있었다.