184 통신저자:김 주 학
경기도 고양시 덕양구 화정동 697-24 관동대학교 의과대학 명지병원 정형외과 Tel:031-810-5409․Fax:031-810-6537 E-mail:[email protected]
*본 논문은 2005년 제49차 대한정형외과학회 추계학술대회에서 구연되었음.
Address reprint requests to:Joo-Hak Kim, M.D.
Department of Orthopaedic Surgery, Myongji Hospital, Kwandong University College of Medicine, 697-24, Hwajeong-dong, Deogyang-gu, Goyang 412-270, Korea
Tel:82-31-810-5409․Fax:82-31-810-6537 E-mail:[email protected]
골다공증을 동반한 상완골 근위부 분쇄골절의 변형된 Steinmann 핀과 긴장대 강선 요법을 이용한 치료
정수태․김주학․김형수․박상준
관동대학교 의과대학 명지병원 정형외과학교실
목 적: 골다공증을 동반한 상완골 근위부 분쇄골절에서 변형된 Steinmann 핀과 긴장대 강선 요법을 이용한 내고정의 유용성을 평가하
고, 골밀도, 연령, Neer 점수 및 골유합의 기간 간의 상관관계를 분석하고자 하였다.
대상 및 방법: 1998년 9월부터 2005년 2월 사이에 상완골 근위부 골절에 대해, 변형된 Steinmann 핀과 긴장대 강선 요법을 이용하여
내고정 치료를 시행한 25명의 환자 중 골다공증을 동반한 여자환자 12명을 대상으로 하였으며, 평균 연령은 73.6세 (범위, 59~85세),
평균 추시 기간은 20.8개월 (범위,6~39개월)이었다. 임상적 결과는 Neer의 평가 기준으로 측정한 점수를 이용하였다.
결 과: 임상적 결과는 우수가 8예, 만족이 4예였으며, 최종 추시 상에서 모든 골절의 골유합을 얻었다. 수술 후 합병증으로 Steinmann
핀의 근위부 자극으로 인한 충돌증후군으로 인한 증상이 2예에서 있었으나, 골 유합을 얻은 뒤 내고정물을 제거하였고, 1예에서 수술 부위의 감염으로 항생제 치료, 세척술 및 이차 봉합술로 증상은 모두 소실되었다.
결 론: 상완골 근위부 골절에서 변형된 Steinmann 핀과 긴장대 강선 요법을 이용한 내고정술은 골다공증이 있는 환자의 골절부의
완전한 골유합을 가능하게 하였고, 수술 후 합병증의 발생 빈도가 낮고, 충분한 내고정력으로 조기 재활치료를 가능하게 하였다.
색인 단어: 상완골 근위부 골절, 골다공증, 변형된 Steinmann 핀
Treatment with Modified Steinmann Pins and Tension Band Wiring Technique in Proximal Humeral Comminuted Fractures with Osteoporosis
Soo-Tai Chung, M.D., Joo-Hak Kim, M.D., Hyung-Soo Kim, M.D., Sang-Joon Park, M.D.
Department of Orthopaedic Surgery, Myongji Hospital, Kwandong University College of Medicine, Goyang, Korea
Purpose: To evaluate the usefulness of internal fixation with modified Steinmann pins and tension band wiring technique in comminuted proximal humeral fracture with osteoporosis and the correlations among bone mineral density, age, Neer’s score and period of union.
Materials and Methods: Twelve cases of comminuted proximal humeral fracture with osteoporosis were surgically treated with modified Steinmann pins and tension band technique, and followed up for an average 20.8 months (range, 6~39 months).
Average age was 73.6 years old (range, 59~85 years old). Results were assessed using Neer’s evaluation criteria.
Results: Excellent results were noted in eight cases and satisfactory results in four cases. Radiological union was obtained in all cases. Two cases showed impingement syndrome of the proximal portions of Steinmann pins, which were managed by early removal of the metal. One case developed operative wound infection, which were managed by antibiotics therapy, irrigation and secondary closure.
Conclusion: Internal fixation using modified Steinmann pins and tension band wiring technique for proximal humeral fracture, with osteoporosis, makes complete union of fracture, minimizes risk of complications, and enables early rehabilitation by rendering relatively rigid fixation.
Key Words: Proximal humeral fracture, Osteoporosis, Modified Steinmann pin
Table 1. Patient data
Periods of bone
Case Sex/Age Cause of injury Type of injury* Duration of F/U (Mon) Complication union (Wks)
1 F/74 T. A 2 part Fx. 39 16 Impingement syndrome
2 F/75 Slip down 3 part Fx. 6 21 -
3 F/60 Fall down 2 part Fx. 33 14 -
4 F/77 Slip down 2 part Fx. 28 12 -
5 F/59 Slip down 2 part Fx 33 15 -
6 F/81 Slipl down 3 part Fx 25 16 -
7 F/68 Slip down 3 part Fx 12 16 -
8 F/68 Slip down 3 part Fx. 8 16 -
9 F/70 Slip down 2 part Fx. 36 12 -
10 F/68 Slip down 3 part Fx 24 14 Wound infection
11 F/85 Slip down 2 part Fx. 6 20 -
12 F/59 Slip down 2 part Fx. 12 15 Impingement syndrome
*Neer's classification. T. A: Traffic accident, Fx: Fracture, F/U: Follow up, Mon: Months, Wks: Weeks.
서 론
골다공증은 골조직의 양의 감소와 구조적인 이상으로 골강 도의 감소와 함께 쉽게 골절을 일으킬 수 있는 질환이다5,6,8). 골절의 발생은 나이의 증가, 골밀도의 감소와 밀접한 관련이 있음이 보고된 바 있다17). 골다공증이 있는 중년 이후의 여 성에서 흔히 발생하는1) 상완골 근위부 골절은 전체 골절의 약 4~5%를 차지한다2,3). 이 중 80~85%를 차지하는 안정 골절은 보존적 치료로 만족스러운 결과를 얻은 것으로 알려 져 있다10,24). 그러나 약 20%에서는 골절부의 전위가 심하거 나 불안정성이 있어 보존적 치료보다는 수술적 치료를 고려 하게 되는데, 여러 수술적 방법에 대해서는 다양한 결과가 보고되고 있으나, 아직까지도 논란이 많다3,7,9,12-15,18-33). 특히 노령환자의 경우 장기간의 보존적 치료로 골다공증의 심화 와 전신적인 합병증 발생 가능성이 높으므로 가능하면 견고한 내고정을 통해 조기운동을 시킬 것이 권장되고 있다9,26). 골다 공증이 있는 노인의 경우 금속판과 나사못을 이용한 내고정 술은 내고정물의 해리와 금속판의 충돌에 의한 견관절 통증, 과도한 연부 조직 박리로 인한 무혈성 괴사를 일으킬 수 있 는 단점이 있다10,14,18). 골수강 내 고정물과 긴장대 강선을 이 용한 내고정술이 고령 환자에서 연부 조직의 박리를 최소화 하며 훌륭한 고정력으로 조기 재활 치료를 가능하게 하여 비 교적 합병증이 적어 널리 사용된다12,13,24,28,34)
. 우리나라의 경 우 노인 환자들의 체격과 상완골 길이가 서양인과 차이가 있 어 서양의 상품화된 유연성 골수강 내 고정물을 사용하는 데 어려움이 있어왔다4). 이에 저자들은 Steinmann 핀의 두부에 두 개의 구멍을 뚫은 변형된 Steinmann 핀을 제작하고 긴장 대 강선을 함께 이용하여 내고정술을 시행하였다. 본 연구의
목적은 이 술식의 결과를 분석하여 골다공증을 동반한 상완 골 근위부 분쇄골절의 내고정 방법으로서의 유용성을 평가 하고, 골밀도, 연령, Neer 점수 및 골유합의 기간 간의 상관 관계를 분석하고자 하였다.
대상 및 방법
1. 연구 대상
1998년 9월에서 2005년 2월 사이에 상완골 근위부 골절로 내원하여, 변형된 Steinmann핀을 이용한 골수강 내 고정과 긴 장대 강선으로 내고정술을 시행한 환자 25명 중, DEXA (Dual- Energy X-ray Absorptiometry, QDR4500, Hologic) 방법으로 요추 1~4번과 대퇴상부의 대퇴경부 Ward 삼각, 전자부의 골 밀도 검사를 시행하여 한 부위 이상에서 T-score<-2.5 SD 임이 확인된 12명의 여자 환자를 대상으로 하였다. 이 중 7예 가 Neer의 분류상27) 상완골 외과적 경부 이분 골절이었고, 5 예가 외과적 경부 골절 및 대결절 골절을 동반한 삼분 골절이 었다. 평균 연령은 73.6세 (범위, 59~85세)였으며, 수상 원인 은 자동차 사고 1예, 추락 1예, 실족 10예였으며, 평균 추시 기간은 20.8개월 (범위, 6~39개월)이었다 (Table 1).
2. 재료 및 수술 방법
사용된 Steinmann 핀은 직경 3.2 mm 또는 3.6 mm, 길이 175 mm, 200 mm 또는 225 mm로서 머리 부분에 2개의 구 멍을 뚫어 변형시킨 것을 수술 전 측정한 건측의 방사선계측 을 활용하여 적당한 크기를 선택한 뒤, 상완골 근위부 형태
Table 2. Results according to Neer's evaluation criteria
Case
Criteria (units)
1 2* 3 4 5 6* 7* 8* 9 10* 11 12
1. Pain (35) 30 30 35 30 30 30 30 35 30 30 30 30
2. Function (30) 26 26 30 30 26 30 26 26 28 28 28 30
3. Range of motion (25) 16 17 20 21 17 21 17 19 21 21 22 24
4. Anatomy (10) 10 10 10 10 8 10 10 10 10 10 10 10
Total (100) 82 83 95 91 81 91 83 90 89 89 90 94
Results S S E E S E S E E E E E
S: Satisfactory, E: Excellent. *3 part fracture.
Fig. 1. (A) Modified steinmann pins have different sizes.
(B) Modified steinmann pin has proximal two holes.
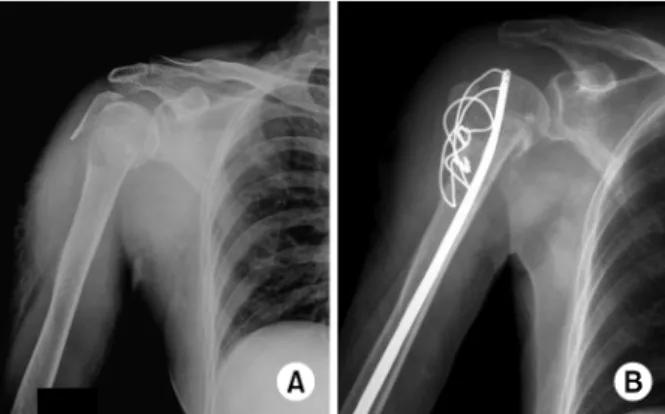
Fig. 2. (A) Initial radiograph shows a surgical neck fracture of the proximal humerus, eighty five-year-old woman.
(B) Postoperative radiograph shows intramedullary fixation with two modified Steinmann pins and one tension band wiring.
에 맞게 구부려서 이용하였다 (Fig. 1). 변형된 Steinmann 핀의 두부에 위치한 2개의 구멍 중, 위에는 1.2 mm 굵기의 강선을 통과시켜, 경부 골절부에서 약 4~5 cm 원위부에 횡 으로 뚫은 구멍을 이용하여 8자형 긴장대를 형성하여 내고정 을 시행했으며 (Fig. 2), 아래에는 필요에 따라서 5번 비흡수 성 봉합사를 이용하여 근위 골편간 봉합 고정을 시행하거나, K-강선을 걸어 Steinmann 핀의 방향을 바꿀 수 있게 하였고, 또 다른 8자형 긴장대를 추가할 수 있게 하였다 (Fig. 3). 수 술 후 재활치료는 가능한 한 빨리 시행하는 것을 원칙으로 하여, 1주일 후부터 추 운동 및 수동적 관절운동을 시행하였 고, 능동적 운동은 6주 후에 허용하였다.
3. 평가 방법
결과의 판정에는 Neer의 평가기준을 이용하였다26). 총 단
위 100을 기준으로 동통 35단위, 기능 30단위, 운동 범위 25 단위, 해부학적 위치 10단위로 할당하여 합산한 점수가 89 이상은 우수, 80 이상은 만족, 70 이상은 불만족, 70 이하는 실패로 판정하였다. 통계학적 평가는 비모수 검정 (nonpara- metric test)의 Ruskal-Wallis 방법과, Pearson 상관 분석법 (correlation analysis)을 이용하여 골밀도, 연령, Neer 점수 및 골유합의 기간과의 상관관계를 평가하였다.
결 과
우수가 8예, 만족이 4예였다. 이분 골절과 삼분 골절의 결 과는 특별한 차이를 보이지 않았다 (Table 2). 최종 추시상 모든 예에서 골유합을 얻었으며, 골유합의 판정은 단순 방사 선 촬영상 가골이 골절부위를 넘어서 견고하게 형성되어 있 고, 이학적 검사상 골절부위에 압통이 없는 경우로 하였다.
평균 골유합 기간은 15.6주 (범위, 12~21주)였다 (Table 1).
Fig. 3. (A) Initial radiograph shows a 3 part fracture of the proximal humerus sixty eight-year-old woman.
(B) Postoperative radiograph shows intramedullary fixation with two modified Steinmann pins and two tension band wirings.
0 5 10 15 20 25
50 60 70 80 90
Age
Period of union
r=0.414 p=0.181
Fig. 4. This graph shows a correlation between age and aver- age of Neer's score.
70 75 80 85 90 95 100
50 60 70 80 90
Age
Neer`s score r=-0.047
p=0.885
Fig. 5. This graph shows a correlation between age and aver- age of union period.
0 4 8 12 16 20 24
-6 -5 -4 -3 -2
BMD
period of union
r=0.256 p=0.423
Fig. 6. This graph shows a correlation between BMD and average of union period.
수술 후 합병증으로, Steinmann 핀 근위부의 자극으로 인한 충돌 증후군이 2예 있었으나, 골유합 후 내고정물을 제거하 여 문제를 해결하였으며, 1예에서 유발된 수술부위의 감염으 로 항생제 치료 및 세척술, 이차 봉합술로 문제를 해결하였 다. 집단의 수가 적어 통계적인 평가를 내리기에 무리가 있 다고 생각되었지만, 환자의 연령과 골유합에 필요한 기간과 의 관계는 서로 통계학적 유의성이 없었으며 (r=0.414, p> 0.05) (Fig. 4), 연령과 Neer의 평가 기준에 따른 점수와의 관계는 서로 통계학적 유의성이 없었다 (r=-0.047, p> 0.05) (Fig. 5). 그리고 골밀도 검사상 가장 낮은 수치와 골 유합에 필요한 기간과의 관계는 서로 통계학적 유의성이 없 었다 (r=0.256, p>0.05) (Fig. 6).
고 찰
상완골 근위부의 골절은 골다공증이 있는 노인층, 특히 여 성에서 발생빈도가 높다. Horak과 Nilsson은 연령이 증가함 에 따라 남자보다 여자에서 발생빈도가 두 배 이상으로 증가 된다고 보고하였다16).
골다공증이 있는 노인 환자의 상완골 근위부 골절의 치료 에서는 장기간 고정으로 전신적 합병증, 유착성 관절낭염 등 으로 인한 견관절의 구축 및 골다공증 심화의 가능성이 높 다. 따라서 여러 수술적 방법에 대해 저자에 따라 다양한 결 과가 보고되고 있으나 아직까지도 논란이 많다3,7,9,12-15,18-33). Kristiansen 등은 조기에 통증 없이 관절운동을 할 수 있는 경피적 정복 후 외고정술을 권장하였으나, 경피적 정복을 통 한 외고정술은 정확한 정복이 어려울 뿐만 아니라, 외고정 장치에 의해 조기 재활이 방해되는 단점이 있다20,22,23,28). 내 고정 방법에는 금속판 및 나사못을 이용한 내고정이 있으나 골다공증이 있는 환자에서는 고정이 안정적이지 못하고, 금
속판의 충돌에 의한 견관절 통증, 금속판과 나사의 고정을 위해 연부 조직의 많은 손상으로 상완골두 무혈성 괴사가 초 래될 수 있다10,14,18).
Hawkins 등은 노인의 3분 골절에서 소결절과 대결절에 횡으로 통과시킨 강선을 8자 모양으로 교차시킨 후 근위 간 부의 구멍에 통과시켜 매듭을 조이는 방법으로, 골절부위의 광범위한 노출을 요하지 않으며 비교적 쉬운 술기인 긴장대 요법을 주장하였고14), Cuomo 등은 골다공증이 있는 상완골 근위부 골절에서 회전근개를 봉합사나 강선을 이용하여 고 정하는 방법으로 불필요한 연부 조직의 박리를 피하여 골두 의 무혈성 괴사를 막아줄 수 있다고 소개하였으나7), 골다공 증이 동반된 경우 고정력이 약하여 조기 관절 운동을 하기에 어려움이 있고, 약한 고정력으로 인한 불안정한 정복은 오히 려 불유합을 초래한다9). 이러한 문제점들을 보완한 방법으로 Koval 등은 Ender정과 긴장대를 이용한 내고정이 강한 고정 력을 갖는다고 하였고19), Flatow 등은 이 술식의 장점으로서 Ender정이 골수강 내에 있기 때문에 골두의 골밀도에 영향 을 비교적 적게 받으며, 강선 고리의 근위부가 약한 뼈가 아 니라 Ender정의 두부에 뚫린 구멍에 고정된다는 점을 지적하 였다10). 또한 이 방법은 불안정한 골절편의 충분한 고정으로 수술 후 조기 견관절 운동의 시행을 가능하게 한다12,13,24,28,34). 이러한 장점에도 불구하고 우리나라 노인들의 체격뿐만 아 니라 상완골 길이가 서양인과 비교하여 왜소하여, 서양의 상 품화된 유연성 골수강 내 고정물을 사용하는데 어려움이 있 어 왔다4). 이에 저자들은 머리 부분에 2개의 구멍을 뚫어 변 형시킨 Steinmann 핀과 긴장대 강선 고정을 사용하여 골다 공증을 갖는 상완골 근위부 분쇄 골절의 모든 치료 예에서 고정의 실패나 불유합 없이 기능적인 면에서도 좋은 결과를 얻을 수 있었다 (Fig. 2, 3).
전위형 상완골 근위부 골절 후의 기능회복은 여러 인자에 의하여 좌우되나11), 본 연구에서는 기능회복과 골유합의 기 간은 골다공증의 정도, 환자의 연령과 상관관계는 없었다 (Fig. 4~6). 기능 회복과 골유합의 기간은 분쇄성이나 골결 손과 같은 손상의 정도, 수술에 의한 고정력의 정도에 영향 이 있을 것으로 사료되며, 무엇보다도 수술 후 기능의 향상 을 위해 조기 재활치료의 중요성이 다시 인식되어야 할 것으 로 사료된다.
결 론
골다공증 및 골절부의 분쇄성이 있어 일반적인 수술법으 로 충분한 고정력을 얻기가 어려운 상완골 근위부 골절에서 변형된 Steinmann 핀과 긴장대 강선을 이용한 술기는 골절 부위에 수직으로 작용하는 굴곡력과 회전력에 대해 안정성 을 얻을 수 있으며 골절부위의 연부 조직의 박리를 최소화하
여 무혈성 괴사와 수술 후 동통을 줄이고, 충분한 고정력으 로 조기재활을 가능하게 하는 유용한 치료법으로 사료된다.
참 고 문 헌
1) Bengner U, Johnell O, Redlund-Johnell I: Changes in the incidence of fracture of the upper end of the humerus during a 30-year period. A study of 2,125 fractures. Clin Orthop Relat Res, 231: 179-182, 1988.
2) Bigliani LU: Fractures of the proximal humerus. In:
Rockwood CA Jr, Masten FA III eds. The shoulder. 1st ed.
Philadelphia, WB Saunders Co: 287-334, 1990.
3) Bigliani LU, Fratow EL, Pollck RG: Fractures of the pro- ximal humerus. In: Rockwood CA, Masten FA eds. The shoulder. 2nd ed. Philadelphia, WB Saunders Co: 337-280, 1998.
4) Chun JM, Chung ER, Kim KY: Measurement of proximal humerus in Korean adult skeleton. J Korean Orthop Assoc, 34:
219-226, 1999.
5) Cummings SR, Cauley LA, Palermo L, et al: Racial dif- ference in hip axis lengths might explain recial difference in rates of hip fracture. Study of Osteoporotic Fractures Research Group. Osteopporosis Int, 4: 226-229, 1994.
6) Cundy T, Cornish J, Evans MC, Gamble G, Stapleton J, Reid IR: Sources of interracial variation in bone mineral density. J Bone Miner Res, 10: 368-373, 1995.
7) Cuomo F, Flatow EL, Maday MG: Open reduction and internal fixation of two and three-part dispalaced surgical neck fractures of the proximal humerus. J Shoulder Elbow Surg, 1:
287-295, 1992.
8) Dennison E, Mohamed MA, Cooper C: Epidemiology of osteoporosis. Rheum Dis Clin North Am, 32: 617-629, 2006.
9) DePalma AF, Cautilli RA: Fractures of the upper end of the humerus. Clin Orthop Relat Res, 20: 73-93, 1961.
10) Flatow EL, Cuomo F, Maday MG, Miller SR, McIlveen SJ, Bigliani LU: Open reduction and internal fixation of two-part displaced fractures of the greater tuberosity of the proximal part of the humerus. J Bone Joint Surg Am, 73: 1213-1218, 1991.
11) Hagg O, Lundberg BJ: Aspects of prognostic factors in com- minuted and dislocated proximal humerus fractures. In: Bate- man JE, Welsh RP eds. Surgery of the shouder. Philadelphia, BC Decker: 1984.
12) Hall RF Jr, Pankovich AM: Ender nailing of acute fracture of the humerus. J Bone Joint Surg Am, 69: 558-567, 1987.
13) Hawkins RJ, Angelo RL: Displaced proximal humeral frac- tures. Selecting treatment, avoiding pitfalls. Orthop Clin North Am, 18: 421-431, 1987.
14) Hawkins RJ, Bell RH, Gurr K: The three-part fracture of the proximal part of the humerus. J Bone Joint Surg Am, 68:
1410-1414, 1986.
15) Hawkins RJ, Kiefer GN: Internal fixation techniques for proximal humeral fractures. Clin Orthop Relat Res, 223: 77-85, 1987.
16) Horak J, Nilsson BE: Epidemiology of fracture of the upper end of the humerus. Clin Orthop Relat Res, 12: 250-253, 1975.
17) Kang JD, Kim HC, Kyoung CW, Seo HC: Case-control study of risk factors of fracture due to osteoporosis. J Korean Fractures Soc, 15: 7-14, 2002.
18) Ko JY, Yamamoto R: Surgical treatment of complex fracture of the proximal humerus. Clin Orthop Relat Res, 327: 225- 237, 1996.
19) Koval KJ, Blair B, Takei R, Kummer FJ, Zuckerman JD:
Surgical neck fractures of the proximal humerus: a laboratory evaluation of ten fixation techniques. J Trauma, 40: 778-783, 1996.
20) Kristiansen B: External fixation of proximal humeral fracture.
Clinical and cadaver study of pinning technique. Acta Orthop Scand, 58: 645-648, 1987.
21) Kristiansen B, Christensen SW: Plate fixation of proximal humeral fractures. Acta Orthop Scand, 57: 320-323, 1986.
22) Kristiansen B, Kofoed H: External fixation of displaced frac- ture of the proximal humerus. Technique and preliminary re- -sults. J Bone Joint Surg Br, 69: 643-646, 1987.
23) Kristiansen B, Kofoed H: Transcutaneous reduction and exter- nal fixation of displaced fractures of the proximal humerus. A controlled clinical trial. J Bone Joint Surg Br, 70: 821-824,
1988.
24) Lee KW, Hwang IS, Lee SH, et al: Treatment of two-part, displaced surgical neck fracture of the proximal humerus with modified Ender nail and tension band technique. J Korean Fractures Soc, 12: 395-401, 1999.
25) Leyshon RL: Closed treatment of fractures of the proximal humerus. Acta Orthop Scand, 55: 48-51, 1984.
26) Neer CS 2nd: Displaced proximal humeral fractures. II. Treat- ment of three-part and four-part displacement. J Bone Joint Surg Am, 52: 1090-1103, 1970.
27) Neer CS 2nd: Displaced proximal humeral fractures. I. Classi- fication and evaluation. J Bone Joint Surg Am, 52: 1077-1189, 1970.
28) Ogiwara N, Aoki M, Okamura K, Fukushima S: Ender nailing for unstable surgical neck fractures of the humerus in elderly patients. Clin Orthop Relat Res, 330: 173-180, 1996.
29) Paavolainen P, Bjorkenheim JM, Slatis P, Paukku P: O- perative treatment of severe proximal humeral fractures. Acta Orthop Scand, 54: 374-379, 1983.
30) Savoie FH, Geissler WB, Vander Griend RA: Open reduc- tion and internal fixation of three-part fractures of the proximal humerus. Orthopedics, 12: 65-70, 1989.
31) Sehr JR, Szabo RM: Semitubular blade plate for fixation of the proximal humerus. J Orthop Trauma, 2: 327-332, 1988.
32) Stableforth PG: Four-part fractures of the neck of the hu- merus. J Bone Joint Surg Br, 66: 104-108, 1984.
33) Sturzenegger M, Fornaro E, Jakob RP: Results of surgical treatment of multifragmented freactures of the humeral head.
Arch Orthop Trauma Surg, 100: 249-259, 1982.
34) Sung JH, Kim WY, Han CW, Ryu JD, Son HS, Kim JY:
Operative treatment using minimized internal fixation and tension band technique on proximal humeral fracture. J Korean Orthop Assoc, 33: 1852-1858, 1998.