- 419 -
Address reprint requests to Heui-Jeon Park, M.D.
Department of Orthopaedic Surgery, Wonju College of Medicine, Yonsei University
#162 Ilsan-dong, Wonju, Kangwon-do 220-050, Korea
Tel : 82-33-741-1352, Fax : 82-33-741-1358, E-mail : Par73@wonju.yonsei.ac.kr
흉요추부 골절의 전방 도달법에 의한 치료
박 희 전・김 인 구
연세대학교 원주의과대학 정형외과학교실
Treatment of Thoracolumbar Fracture with Anterior Approach
Heui-Jeon Park, M.D. and In-Gu Kim, M.D.
Department of Orthopaedic Surgery, Wonju College of Medicine, Yonsei University, Wonju, Korea – Abstract –
The anterior approach to the spine offers several unique solution to problems posed by patients with thoracolumbar injuries. The major weight-bearing elements of the spine are anterior and this is the area where injured elements impinging on the spinal cord can cause significant but reversible damage. The two primary areas of concern for surgeons treating these patients are restoration of mechanical stability of the spinal column and restoration or preservation of neurologic function.
Indications for anterior decompression, 1)a large retropulsed fragment with significant(>50%) canal compromise, 2)anterior col- umn comminution and marked kyphosis, and a time lapse of greater than 10 days from the time of injury. Anterior approaches are also recommended for the late treatment of symptomatic post-traumatic kyphosis that causes pain or neurologic deficit.
The flexion-compression injuries addressed with anterior decompression and strut graft fusion require additional stability for satisfactory healing with maintenance of position assured during bone graft incorporation. Anterior instrumentation is most effective when balanced by an intact posterior ligamentous tension band.
The anterior approach is more superior in canal clearance and effective in restoring bladder and bowel function.
Key Words : Thoracolumbar spine, Fracture, Anterior approach
대한척추외과학회지 제 8 권 제 3 호 Journal of Korean Spine Surg.
Vol. 8, No. 3, pp 419~422, 2001
척추 골절의 치료 목적은 손상 받은 척주의 재 정열, 신경증상의 회복, 조기 운동 및 재활을 통한 사회복귀와 동통 없는 안정성 있는 척추를 갖게 하는 것이다. 많은 보고에서 침상 안정과 체위에 따른 정복에 의한 치료가 장기 추시에서 수술적 치료의 결과와 비슷하다고1,6)하나 신경증상이 동반된 경우나 불안정성 골절에서는 수술적 방법이 선호되고 있다2,9,10,14,15)
.
수술적 치료 방법에는 전방 도달법과 후방 도달법을 이용한 치료가 있으며, 일반적으로 후방 도달법에 의한 치료가 선호되고 있으나, 심한 척수강 침범과 불완전 신 경 손상이 있는 경우, 또는 후방 돌출된 골편에 의한 신
경 압박과 심한 척추 후만이 동반된 만성 척수강 협착이 있는 경우에는 후방에서 시행하는 간접 감압 만으로는 불충분한 경우가 많아 전방 감압을 시행하게 된다.
1. 전방 도달법의 적응증
전방 감압의 목적은 척수강의 감압과 골절 정복에 의 해 불완전 신경손상이 회복 될 수 있는 환경을 만들어 주 는데 있다. 동물 실험에 의하면 척수는 허혈, 급성 출혈, 부종에 의해 수상 후 4~8시간부터 손상이 시작되어 5~6 일 후에는 gray matter의 괴사가 시작된다. 따라서 이 시
간 안에 척수 감압을 해 주어야 신경의 회복을 기대 할 수 있다.
전방 감압은 1) 골편의 척수강 침범이 50%가 넘는 경 우 2) 전주의 복잡 골절과 심한 후만 변형이 동반 된 경 우 3) 수상 후 10일 이상 경과 된 방출성 골절로 간접 감 압으로는 골편의 정복을 기대하기 어려은 경우 4) 후방 도달법에 의한 수술을 시행하였으나 골편의 정복이 만 족스럽지 않고 신경회복이 불완전 할 경우에 적응증이 된다. 골편의 척수강 침범 정도와 신경 증상과의 관계에 서, 마미총 부위에서는 약 85%의 척수강 침범이 있어도 신경증상이 없을 수 있으나, 척수 부위에서는 20%정도 만 침범이 있어도 심한 하반신 부전마비를 초래 할 수 있어 척수강 협착 정도와 신경증상과는 항상 연관성이 있는 것은 아니다10)
.
2. 전방 도달법의 장점
전방 도달법은 직접적인 감압이므로 간접적인 후방 도달법 보다 더욱 확실한 감압을 시행 할 수 있으며 더 많은 신경의 회복을 기대 할 수 있다. Scoliosis Research
S o c i e t y에서의 연구에서는 전방 감압과 후방 감압에서
신경의 회복(Frankel scores)에 있어 별 차이가 없다고 하 였으나7 ), Kostuik
1 0 )은 전방 감압 후 1.6 Frankel grades의 신경 회복이 있다고 하면서 전방 감압을 권장하였다. 다 른 연구에서도 전방 감압은 방광기능을 보존하는데 더 욱 효과적이고 , 1/3 이상에서 정상으로 회복되었으며5 0 %에서 보행이 가능하다고 하면서 전방 감압의 효용
성을 강조하였다3,5,13).
전방 도달법은 신경 증상과 통증이 동반된 외상성 후 만의 치료에 효과적이다. Bohlman 등2)은 외상 후 4.5년 이 지난 환자에서 전방 감압으로 외상성 후만으로 생긴 동통을 95%에서 치유 할 수 있었다고 보고하였다. 외상 성 만성 후만에서, 후방 도달법은 척수강 협착을 감압 할 수 없고 골 이식이 인장력이 작용하는 부위에 위치하 기 때문에 불유합이 잘 생기므로 외상성 후만의 치료에 효과적이지 못하다. 그러나 40도 이상의 척추 후만과 경 직된 후만 변형이 있는 경우에는 전방 감압과 후방 고정 기기술을 병행하여야 한다.
3. 전방 도달법의 단점
전방 도달법은 수술 수기가 어렵고 광범위 한 절개가 필요하고, 안정적인 고정을 할 수 있는 고정기기가 없는 단점이 있다. 흉곽의 외상이나 폐 좌상이 있는 다발성 외상 환자에서는 폐 기능의 악화를 초래하게 되고, 추체 절제술 시 상당히 많은 양의 혈액 소실이 있다9)
. 전위 된
추체의 정복을 전방 도달법으로 시도 할 때에는 매우 어 렵고 고정을 시행하여도 매우 불안정하며, 탈구나 전위 가 동반 된 경우에는 골절 된 골편이나 전위 된 후방 구 조물이 정복을 방해하기 때문에 후방 구조물을 절제하 여야 할 필요가 있다.
4. 수술 방법
좌, 우의 도달은 수술 하고자 하는 부위에 따라 달라 질 수 있는데, 우측 전방 도달법은 대동맥의 방해없이 상부 흉추체를 노출시킬 수 있다. 제12 흉추에서 제4 요 추까지는 좌측 도달법이 선호되고 있는데, 이 부위에서 는 대동맥이 추체의 중앙에 위치하고 벽이 얇은 정맥보 다는 두꺼운 벽의 대동맥이 견인에 용이하기 때문이다.
환자는 측와위로 하고 수술대를 jackknife position으로 하여 첨부가 골절 부위에 오도록 한다.
제 1 1흉추-제 1요추의 방출성 골절을 수술하는데 사용 되는 흉요추부 도달법은, 제 10 늑골을 따라 후 액와선
(posterior axillary line)에서 직근막(rectus sheath)까지 절개
한 후 늑간 근을 절단하고 늑골을 anterior rib과 관절을 이 루고 있는 곳에서 절단하는데 이 cartilagenous costal arch 는 횡경막 밑에 있는 후복막으로 들어가는데의 k e y s t o n e 이다. 후방으로는 늑 횡돌기 에 가능한 가까운 곳에서 절 단 한고 복막을 횡경막 하면에서 부터 완전히 분리한다.흉곽으로는 절제한 늑골 밑으로 들어가는데 횡경막은 늑골 끝에서 10~15 mm의 간격을 두고 전방에서부터 후 방으로 aortic hiatus 까지 절개한다. 분절 혈관은 추체 중 앙에서 분리하여 결찰하여야 한다.
제 1요추-제 5요추는 복부 측면 절개를 통하여, 필요 에 따라서는 제 11 또는 제 12 늑골을 절제하고, 제 3흉 추-제 11흉추는 감압하고자 하는 부위의 늑골을 절제하 면 된다. 골절된 추체는 골도, 큐렛, 연마기등을 이용하 여 반대편의 척추경이 보일 때가지 적절한 감압을 시행 하여야 한다. 유합 하고자 하는 추체 상연과 하연의 골 단판이 유지 될 수 있도록 하면서 피질을 제거하여 출혈 이 되도록 한 후 적절한 크기의 삼중 피질골 이식을 시 행하여야 이식 골의 추체내 함몰을 막을 수 있다(Fig. 1).
5. 전방 고정기기
굴곡-압박 골절의 전방 감압 후 이식골의 만족 할 만 한 유합을 얻기 위해서는 추가적인 고정이 필요하여 과 거에는 이식 후 후방고정을 시행하였다8,11)
. 그러나 최근
에는 전방 고정기기도 후방 고정기기와 같은 정도의 안 정성을 갖게 되었으며 전방 고정기기가 효과적이기 위 해서는 손상 받지 않은 후방 인대가 인장 대 역활을 하대한척추외과학회지 Vol. 8, No. 3, 2001
- 420 -
여야 한다12,16)
. 후방 구조물이 완전 절단 된 경우나 골 다
공증이 있을 때에는 전방 고정기기 만으로는 고정력이 충분치 않으므로 후방 고정기기의 보강이 필요하다.전방 고정기기는 초기에는 척추 측만증에 사용되었던
Z e i l k e기기를 이용하였으나 고정력이 약하여 교정소실,
기기 파손등의 합병증을 초래하였다 . 그 후 Dunn sys-t e m
4 )이 개발되었으나 대동맥 미란 등의 합병증으로 현 재는 사용되지 않고, Kostuik-Harrington device는 생역학 실험에서 축성 회전에 약한 단점이 있다1 8 ). 금속판형으
로는 Syracus I-plate 등1 7 )이 있으나 6.5 mm 해면 나사못 2 개만으로 고정하므로 고정력이 약하다. 1984년 K a n e d as y s t e m이 소개되었으며
9 ), 생역학 실험에서 손상 받지 않
은 척추와 같은 정도의 염전력에 대한 강성을 보여 비교 적 안정된 고정력을 갖고, 척추경 나사못을 이용한 상 하2분절씩 고정한 경우와 같은 안정성을 보인다
9 , 1 8 ). 그밖에 Z-plate, Ventrofix, Synex 등이 있다.
REFERENCES
01) Bedbrook GM : Spinal injuries with tetraplegia and para - plegia. J Bone Joint Surg, 61B:267-284, 1979.
02) Bohlman HH, Kirkpatrick JS, Delamarter RB and Lev- enthal ML : Anterior decompression for late pain and paralysis after fractures of the thoracolumbar spine. Clin Orthop, 300:24-29, 1994.
03) Bradford DS and McBride GG : Surgical management of thoracolumbar spine fractures with incomplete neurologic deficits. Clin Orthop, 218:201-216, 1987.
04) Dunn HK : Anterior stabilization of thoracolumbar injuries.
Clin Orthop, 189:116-124, 1984.
05) Esses SI, Botsford DJ and Kostuik JP : Evaluation of surgical treatment for burst fractures. Spine, 15:667-673, 1990.
흉요추부 골절의 전방 도달법에 의한 치료・박희전 외
- 421 -
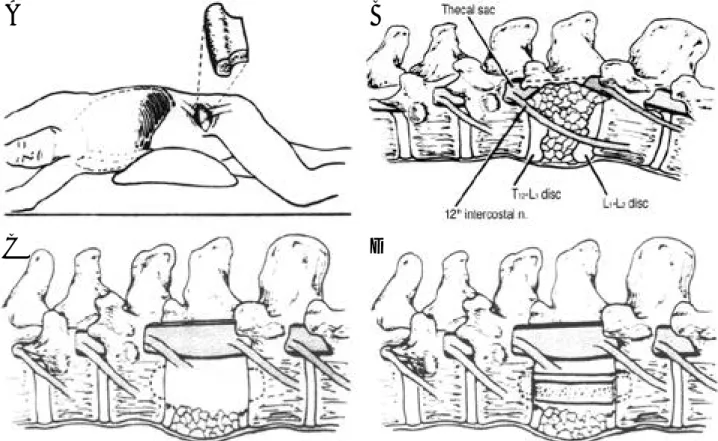
Fig. 1-A. The retroperitoneal approach to the first lumbar vertebra from the left through an incision overlying the twelfth rib.
Fig. 1-B. Orientation to the spinal canal is facilitated by tracing the course of the twelfth intercostal nerve. After removal of the left pedicle of the first lumbar vertebra, the retropulsed vertebral-body fragments of a burst fracture of the first lumbar vertebra are seen compressing the thecal sac.
Fig. 1-C. The vertebral body fragments are removed with a high-speed burr until the base of the opposite pedicle is visualized.
Fig. 1-D. An iliac-crest tricortical strut graft is locked in place using bone tamps. Each end is countersunk into the vertebral body above and below.
A B
C D
06) Freebody D, Bendall R and Taylor RD : Anterior trans- peritoneal lumbar fusion. J Bone Joint Surg, 53B:617-627, 1971.
07) Gertzbein SD : Neurologic deterioration in patients with thoracic and lumbar fractures after admission to the hospi - tal. Spine, 19:1723-1725, 1994.
08) Gertzbein SD, Court-Brown CM, Jacobs RR, Marks P, Martin C, Stoll J, Fazl M, Schwartz M and Rowed D : Decompression and circumferential stabilization of unsta - ble spinal fractures. Spine, 13:892-895, 1988.
09) Kaneda K, Abumi K and Fujiya M : Burst fractures with neurologic deficits of the thoracolumbar-lumbar spine.
S p i n e , 9:788-795, 1984.
10) Kostuik JP : Anterior fixation for burst fractures of the thoracic and lumbar spine with or without neurological involvement. Spine, 13:286-293, 1988.
11) Malcolm BW, Bradford DS and Winter RB and Chou SN : Post-traumatic kyphosis. J Bone Joint Surg, 63:891- 899, 1981.
12) Mann KA, McGowan DP, Fredrickson BE, Falahee M and Yuha HA : A biomechanical investigation of short seg -
ment spinal fixation for burst fractures with varying degree of posterior disruption. Spine, 15:470-478, 1990.
13) McAfee PC, Bohlman HH and Yuan HA : A n t e r i o r decompression of traumatic thoracolumbar fractures with incomplete neurological deficit using a retroperitoneal approach. J Bone Joint Surg, 67:89-104, 1985.
14) Park HJ, Rah JH and Lee HK : Surgical treatment for the burst fracture of the thoracolumbar spine. J Korea Orthop Assoc, 29: 457-486, 1994.
15) Park HJ, Rah JH and Yoo KJ : Operative treatment of thoracolumbar spine fractures with AO internal fixator. J Korean Orthop Assoc, 31:1116-1123, 1996.
16) Roberson JR and Whitesides TE : Surgical reconstruc - tion of late post-traumatic thoracolumbar kyphosis. Spine, 10:307-312, 1985.
17) Yuan HA, Mann KA, Found EM, et al. : Early clinical experience with the Syracuse I-plate, an anterior spinal fixation device. Spine, 13:278-285, 1988.
18) Zdeblick TA, Warden KE, Zou D McAfee PC and Abitol M D : Anterior spinal fixatiors. Spine, 18:513-517, 1993.
대한척추외과학회지 Vol. 8, No. 3, 2001
- 422 -