INTRODUCTION
Nonalcolic fatty liver disease (NAFLD) is a disorder of a wide spectrum of symptoms including those of simple steatosis without any inflammation or fibrosis, steatosis with nonspecific inflammation, and steatosis accompanied by inflammation and fibrosis, namely nonalcoholic steatohepatitis (NASH)
1-3). NASH is a kind of hepatitis with pathologic findings similar to those of alcoholic hepatitis in nonalcoholics
1, 2). Since Ludwig and collea-
gues for the first time described this disease in 1980
4), the seriousness of this disorder has been being increasingly recogni- zed, because it may progress to cirrhosis, hepatic failure, and even hepatocellular carcinoma
5-8). Several conditions such as an advanced age, obesity, DM or insulin resistance, hyperlipidemia, and female gender have been reported as predisposing factors in this disorder
1, 4, 9-12). And in several articles
3, 6, 13-15), a few conditions, such as an advanced age, type II DM, obesity, and increased AST/ALT ratio have been reported to be the
Factors Associated or Related to with Pathological Severity of Nonalcoholic Fatty Liver Disease
Kyung Sik Park, M.D., Yeong Seok Lee, M.D., Heo Won Park, M.D., Sang Hyuck Seo, M.D., Byung Guk Jang, M.D., Jun Young Hwang, M.D.,
Kwang Bum Cho, M.D., Jae Seok Hwang, M.D., Sung Hoon Ahn, M.D., Yu Na Kang, M.D.* and Gap Chul Kim, M.D.
†Departments of Internal Medicine, Pathology* and Diagnostic Radiology
†, Keimyung University School of Medicine, Daegu, Korea
Background : Nonalcoholic fatty liver disease (NAFLD) has been more and more often regarded as a serious disorder, because nonalcoholic steatohepatitis (NASH), a part of NAFLD, may progress to the end stage of liver disease. Though an advanced age, obesity, diabetes mellitus (DM) etc. being not infrequent conditions in Korea, are known to exacerbate the severity of this disease, there are only a few Korean reports on this subject. The purpose of this study is to identify possible factors that might add up to the pathological severity of this disorder in Korean patients.
Methods : Of 60 patients with steatosis found at liver biopsy, 43 NAFLD patients were reviewed retrospectively after exclusion of other liver diseases.
Results : The cases of steatosis were mild, moderate, and severe in 9, 10, and 24 patients, respectively.
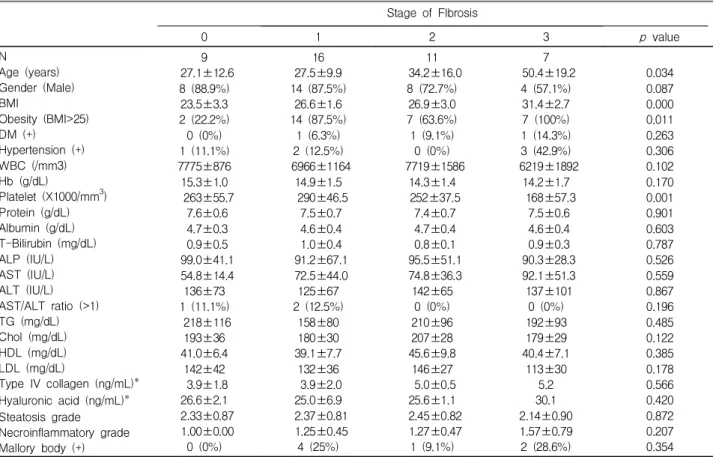
The degree of necroinflammatory activity was mild, moderate, and severe in 33, 9, and 1 patients, respectively. There were no established factors directly related to these classes. As to fibrosis, the cases were classified as none, mild, moderate, severe, and cirrhotic in 9, 11, 16, 7, and 0 patients, respectively.
The stage of fibrosis correlated with the age (p<0.001), BMI (body mass index) (p=0.032), and the platelet count (p=0.009), but the presence of NASH was associated only with BMI (p=0.002) and obesity (p=0.001).
Conclusion : It seems that there are no factors that are directly related to the degree of steatosis or necroinflammatory activity. BMI seems to be a unique factor directly related to both the severity of fibrosis and the presence of NASH. The age and the platelet count are factors that are directly related to the degree of fibrosis but not to the presence of NASH.
Key Words : Fatty liver, Hepatitis, Fibrosis
∙Received : August 25, 2003
∙Accepted : November 13, 2003
∙Correspondence to : Kyung Sik Park, M.D., Department of Internal Medicine, Dongsan Medical Center, 194, Dongsan-dong, Jung-gu, Daegu, 700-712, Korea Tel : 82-53-250-7088, FAX : 82-53-250-7434, E-mail : [email protected]
conditions that can lead to the development of severe fibrosis.
There have been only few Korean reports
16, 17)on this subject, and the results are not fully consistent with those of other reports. The aim of this study was to identify possible factors that may influence the pathological severity, such as steatosis, inflammation, and fibrosis in Korean NAFLD patients.
MATERIALS AND METHODS
1. Patient Population
Reports of 933 liver biopsies which were done between year 1998 and 2002 were analysed retrospectively. Different degrees of steatosis were found in 60 patients at microscopic examination, and, finally, 43 patients with NAFLD were reviewed after clinical exclusion of liver diseases, such as alcoholic liver disease, viral hepatitis, autoimmune hepatitis, drug-induced hepatitis, primary biliary cirrhosis, Wilson's disease, hemochromatosis, biliary obstruction, secondary nonalcoholic steatohepatitis, etc. The alcohol intake below 40 g/week was applied as a criterion for exclusion of alcoholic liver disease. Patients who had experien- ced gastrointestinal surgery or taken drugs
1, 3)which may in- duce hepatic steatosis, such as corticosteroids, estrogens, metho- trexate, tetracycline, calcium channel blockers, or amiodarone were excluded.
2. Methods
Liver biopsy was done with employment of ultrasonography in all patients, stained with hematoxylin-eosin and Masson's trichrome. All biopsy specimens were reviewed again by one pathologist. The grading and staging system proposed by Brunt and et al.
18)was used to classify the severity of the disease;
i.e., the degree of steatosis was graded as 1 (mild), 2 (moderate), and 3 (severe), based on the percent of hepatocytes in the given biopsy specimen. The necroinflammatory activity was also graded as 1 (mild), 2 (moderate), and 3 (severe).
Because there was only one patient whose necroinflammatory activity was graded 3 in this study, the comparison was done between two groups, "grade 1" and "grade 2 or more," for the purpose of the statistical processing. Fibrosis was classified into stages 0 (none), 1 (pericellular or perisinusoidal), 2 (periportal), 3 (bridging), and 4 (cirrhosis). The disease entity "NASH" was considered only when, at least, minimal fibrosis was present, and other cases were considered as "simple steatosis"
regardless of the necroinflammatory activity. Presence of Mallory's hyaline was reported in all specimen. Age, gender, body mass index (BMI), presence of DM or hypertension, serum or blood tests, such as the white blood cell count (WBC), hemoglobin (Hb), platelets, total protein, albumin, total and direct bilirubin, alkaline phosphatase (ALP), aspartate
transaminase (AST), alanine transaminase (ALT), AST/ALT ratio, triglyceride (TG), cholesterol, high density lipoprotein (HDL), low density lipoprotein (LDL), prothrombin time (PT) prolongation, partial thromboplastin time (PTT), type IV collagen, and hyaluronic acid level were reviewed. The patient was considered obese when BMI exceeded 25 and DM case, if there was a documented administration of oral hypoglycemic agents or insulin, with the fasting glucose level exceeding 125 mg/dL on 2 occasions, or random glucose level exceeding 200 mg/dL. Hypertension was considered when the patient had been taking antihypertensive medicine or when diastolic blood pressure exceeding 90 mmHg or systolic blood pressure excee- ding 140 mmHg was noted more than on 2 separate days.
3. Statistical analysis
The SPSS statistical package 11.0 (SPSS Inc., Chicago, IL., U.S.A.) was used for the statistical analysis. All the data were summarized by mean±SD (standard deviation) for continuous variables and by frequency or percentage for categorical variables. The values of the variables were compared among each grades of steatosis and the necroinflammatory activity.
The comparison was also done in respect of each stage of fibrosis and between the groups of simple steatosis and NASH.
The univariate analysis was performed using Mann-Whitney test for comparison of two groups and Kruscal-Wallis test for more than two groups. Chi-square test was used for comparison of the frequency data. Values of p less than 0.05 were considered as "significant" and values of p between 0.05 to 0.1 were considered as "tending to significant" statistically.
The multiple regression analysis was used to identify the independent effects of significant variables on steatosis, the necroinflammatory activity, and fibrosis.
RESULTS
1. Patients' demographic and basic laboratory data The main clinical and laboratory data of the patients of the study are summarized in Table 1. Thirty four (79.1%) patients were male. The mean age was 32.9 years. Mean BMI was 26.8, and the obese patients, whose BMI exceed 25.0, were thirty (69.8%). Three (7.0%) patients had DM and six (14.0%) patients had hypertension. Only three (7.0%) patients had AST/ALT ratio above 1.
2. Histologic findings
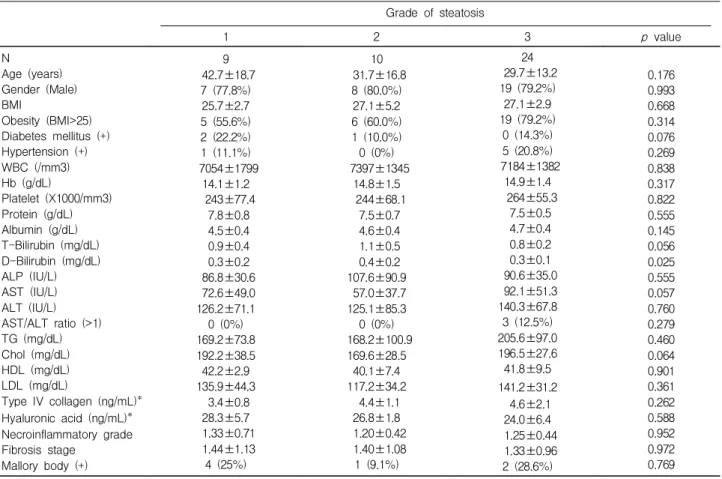
The biopsy findings are summarized in Table 2. The grades
of steatosis were 1 in 9 (20.9%), 2 in 10 (23.3%), and 3 in 24
(55.8%) patients, respectively. The grades of the necroin-
flammatory activity were 1, 2, and 3 in 33 (76.8%), 9 (20.9%),
and 1 (2.3%) patients, respectively. There were 9 (20.9%) sim- ple steatosis and 34 (79.1%) NASH patients. The ostages of fibrosis were 0 in 9 (20.9%), 1 in 11 (25.6%), 2 in 16 (37.2%), and 3 in 7 (16.3%) patients, respectively. There were no patients with fibrosis stage 4. Mallory bodies were found in 7 (16.3%) patients.
3. Factors associated with the degree of steatosis, necroinflammatory activity, and fibrosis
In the univariate analysis (Table 3), there was a significant difference in the direct bilirubin concentration among the 3 grades groups of steatosis (p=0.025), but the mean levels were within the normal range. The degree of steatosis by DM (p=0.076), total bilirubin concentration (p=0.055), AST (p=0.057), and serum cholesterol level (p=0.064). None of these variables were significant independently in the multivariate analysis.
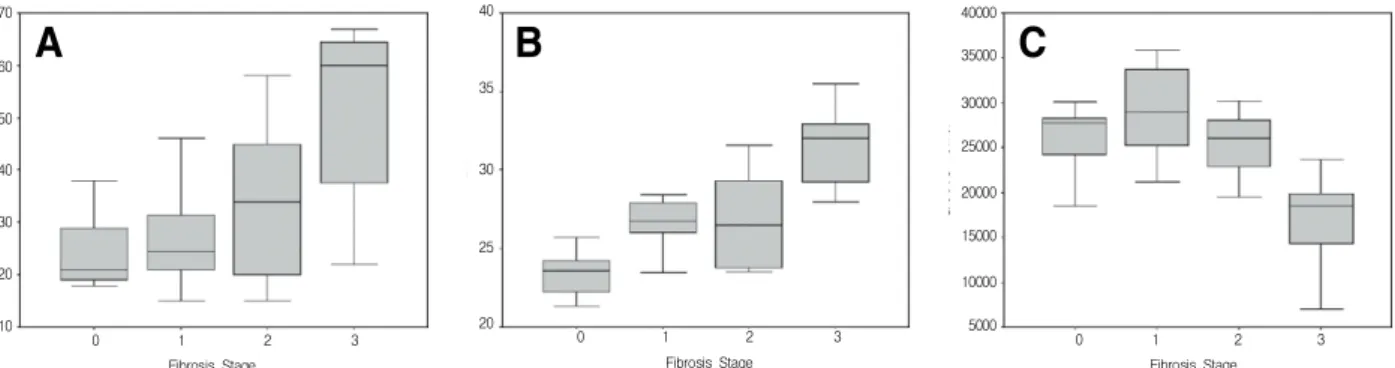
Though the patients of the advanced age (p=0.082) and low hemoglobin concentration (p=0.056) showed a tendency to have Figure 1. The distribution of age (A), BMI (B), and platelet count (C) according to the stage of fibrosis. In all three above variables, the statistically significant differences were taken from radically different values of the stage 3 group.
0 1 2 3
Fibrosis Stage 10
20 30 40 50 60 70
0 1 2 3
Fibrosis Stage 20
25 30 35 40
0 1 2 3
Fibrosis Stage 5000
10000 15000 20000 25000 30000 35000 40000
A B C
Table 1. Patient demographics and basic laboratory data (n=43)
Variables Value/Number
Age (years) Gender (Male) BMI
Obesity (BMI>25) Diabetes mellitus (+) Hypertension (+) WBC (/mm3) Hb (g/dL)
Platelet (X1000/mm
3) Protein (g/dL) Albumin (g/dL) T-Bilirubin (mg/dL) D-Bilirubin (mg/dL) ALP (IU/L) AST (IU/L) ALT (IU/L) AST/ALT ratio (>1) TG (mg/dL) Chol (mg/dL) HDL (mg/dL) LDL (mg/dL)
Type IV collagen (ng/mL)*
Hyaluronic acid (ng/mL)*
32.9±15.8 34 (79.1%) 26.8±3.5 30 (69.8%)
3 (7.0%) 6 (14.0%) 7206±1437
14.7±1.4 255±63
7.5±0.6 4.7±0.4 0.9±0.4 0.3±0.2 93.8±51.8 72.6±39.4 133.8±71.4 3 (7.0%) 190.8±93.7 189.3±31.6 41.4±8.1 134.6±34.7
4.3±1.6 25.6±5.2
All values are described as mean±SD. BMI, body mass index;
WBC, white blood cell; Hb, hemoglobin; ALP, alkaline phospha- tase; AST, aspartate aminotransferase; ALT, alanine aminotrans- ferase; TG, triglyceride; Chol, cholesterol; HDL, high density li- poprotein; LDL, low density lipoprotein
*Total number of subject is 18.
Figure 2. ROC curve for diagnosis of NASH with BMI. Cut-off BMI value of 26.0 was relevant for theto diagnosis of NASH, with sensitivity and specificity of 76% and 89%, respectively (BMI : body mass index).
1-Specificity BMI score of 28.0 is cut-off value
0.00 .25 .50 .75 1.00
0.00 .25 .50 .75 1.00