경추 후종인대 골화증의 전방경유 감압술 및 골 융합술후 예후인자에 대한 임상분석
인천기독병원 신경외과
심상준·조준호·유수일·권영대·이용성
= Abstract =
Clinical Analysis of Postoperative Prognostic Factors of Cervical Anterior Decompression and Interbody Fusion for Ossification of Posterior Longitudinal Ligament
Sang Joon Sim, M.D., Jun Ho Cho, M.D., Soo Il Yoo, M.D., Young Dae Kwon, M.D., Yong Sung Lee, M.D.
Department of Neurosurgery, Incheon Christian Hospital, Incheon, Korea
bjective:To investigate the prognostic factors associated with outcome in patients with ossification of posterior longitudinal ligament.
Method:During the past 4 years, we have operated on 35 patients with cervical OPLL. Anterior cervical decompression(total or subtotal corpectomy, discectomy, and removal of the OPLL) and interbody fusion with iliac bone were performed in all patients.
Results:Eight cases(22.9%) were continuous type, 11(31.4%) segmental, 13(37.1%) Mixed, and 3(8.6%) localized type. Thirty-two patients(91.4%) showed an excellent or good results.
Conclusion:These results indicate that surgical treatment should be considerated in case of clinical grading higher than Ⅱ and the surgical outcome is worse when duration of preoperative symptom is longer and when percentage of spinal narrowing is higher. Anterior cervical decompression and interbody fusion seems to be a better method in patients with lesions limited to one or two level. Age at surgery did not significantly affect the outcom.
KEY WORDS:Ossification of posterior longitudinal ligament・Cervical anterior decompression・Interbody fusion.
서 론
1838년 Key가 Guys Hospital Reports를 통하여 척추 인대가 골화될 수 있다고 보고한 뒤, 1964년 Terayama13) 는 이 질환을“Ossification of posterior longitudinal li- gament(OPLL)”이라고 명명하였으며 이후 이에 대한 연 구가 일본에서 활발히 진행되어 왔고 최근 한국 등 동남아 시아 지역국가에서 많이 발생한다고 보고되고 있다17).
후종인대 골화증의 형태학적 분류는 일본 후생성의 분류 법15)에 의하여 하나 이상의 추체에 걸쳐 골화가 분절없이 연속되어 있는 연속형(continuous), 연속되지 않으면서 여 러 추체에 분절되어 있는 분절형(segmental), 연속형과 분
절형이 섞여 있는 혼합형(mixed), 1개의 골화가 추간판을 사이에 두고 2개의 추체에 걸쳐 있는 국소형(localized)으 로 분류된다(Table 1, Fig. 1)10). 후종인대 골화증은 척수강 내로 돌출되어 척수나 신경근을 압박하여 다양한 신경학적 증상을 유발시킨다.
후종인대 골화증의 치료는 대부분 보존적 치료로는 호전 이 되지 않으며 수술적 치료가 필요하다. 수술적 방법으로 는 전방경유 감압술 및 골 융합술(cervical anterior dec- ompression with interbody fusion), 후방경유 감압술 및 척추 후궁 절제술(posterior decompressive laminectomy), 경추 후궁 성형술(expansive laminoplasty) 등이 있다.
본 신경외과에서는 최근 4년간 경추부 후종인대 골화증 으로 전방경유 감압술 및 추체간 골 융합술을 받은 환자 중
OOOO
6개월 이상 추적 가능한 35명에 대한 골 융합율(fusion rate) 과 기능적 경과(functional outcome)를 분석하여 전방 경 유 감압술 및 추체간 골 융합술의 장단점과 수술후 예후에 관여되는 요인들을 파악하여 향후 경추 후종인대 골화증 환 자의 치료 계획수립에 도움이 되고자 한다.
대상 및 방법
1995년부터 1998년까지 본 신경외과에서 경추 후종인 대 골화증으로 진단된 78예의 환자중 전방 경유 감압술 및 추체간 골 융합술을 받은 38예 중 6개월 이상 추적 가능한 환자 35명을 대상으로 하였다.
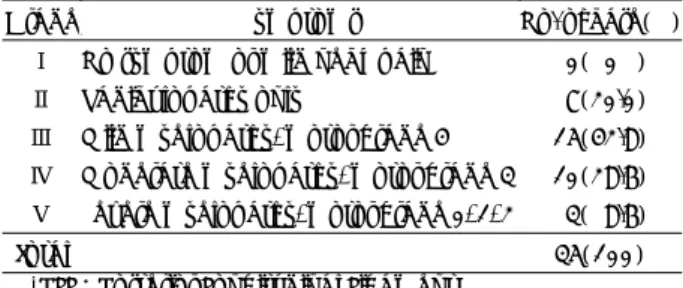
수술전 임상증상의 등급(clinical grading)은 척수 장애 등급에 따라 5등급으로 분류하여(Table 2) 증세가 없거나 경미한 경통을 호소하는 경우는 grade Ⅰ, 상지의 방사 통 증을 호소하는 경우는 grade Ⅱ, 경미한 척수 손상이나 운 동마비의 경우는 grade Ⅲ, 중등도의 척수 손상이나 운동마 비의 경우는 grade Ⅳ, 심한 척수 손상이나 운동마비의 경 우는 grade Ⅴ로 분류하였다.
경추 전방 경유 감압술 및 추체간 골 융합술의 적응증으 로는 임상 증상 등급 grade Ⅱ이상에서 골화의 범위가 2추 체 이하로 한하였으며 3추체 이상은 경추 후방 감압술 및
척추 후궁 절제술을 시행한 바 이번 조사에서 제외하였다.
수술 방법은 추체 전 적출술(total corpectomy) 또는 부분 적출술(subtotal corpectomy)를 시행한후 골화된 후종인대를 제거하거나 척수 경막과 유착이 심하여 박리시 척수 손상을
주거나1)3)17) 혈류의 장애를 일으킬 위험이 있는 경우 부분 절
제로 척수 압박을 감압하였으며 장골을 이용한 자가 골 이식 후 전 예에서 Orion locking plate system으로 고정하였다
수술후 환자들의 임상적, 형태학적 분류에 따른 수술결과 를 비교 분석하였으며 수술후 결과에 영향을 주는 요소를 비교하기 위해 수술당시의 연령, 수술전 증상의 기간, 골화 의 크기에 따른 척추강의 협착 정도를 비교 분석하였다.
결 과
성별 및 연령 분포는 남자 29례, 그리고 여자 6례로 남녀 성비는 4.8:1이며 남자에서 많이 발생하였으며 평균 연령 은 53.6세로 37세에서 64세까지 분포되었으며 50대가 전 체의 42.9%를 차지하였다(Table 3).
Table 1. Morphologic classification of operative patients Type Characteristics No. of case(%) Continuous Ossification over one vertebrae 8(22.9) Segmental Ossification within one
vertebral level 11(31.4)
Mixed Continuous type with
segmental type 13(37.1)
Localized Ossification of intervertebral
disc level 3( 8.6)
Total 35(100)
Table 2. Clinical grade of cervical ossification of PLL*
Grade Symptoms No. of case(%)
Ⅰ No symptom or mild neck pain 0( 0 )
Ⅱ Radiculopathy only 7(20.0)
Ⅲ Mild myelopathy, motor grade 4 15(42.8)
Ⅳ Moderate myelopathy, motor grade 3 10(28.6)
Ⅴ Severe myelopathy, motor grade 0, 1, 2 3( 8.6)
Total 35(100)
*PLL:Posterior Longitudinal Ligament Table 3. Age and sex of operative patients
Age Male Female Total(%)
30-39 1 1 2( 5.7)
40-49 8 1 9(25.7)
50-59 13 2 15(42.9)
60-69 7 2 9(25.7)
Total 29 6 35(100)
Table 4. Postoperative results according to preoperative symptom duration
Results Symptom
duration(month)
No. of
cases(%) Excellent Good Poor
- 3 10(28.6) 9 1 -
3- 6 8(22.9) 6 2 -
6-12 11(31.4) 7 3 1
12-24 4(11.4) 1 2 1
24- 2( 5.7) - 1 1
Total(%) 35(100) 23(65.7) 9(25.7) 3(8.6) Fig. 1. Morphological classification of ossification of posterior
longitudinal ligament.
수술전 증세의 기간을 보면 대부분 무증세로 지내다 작은 외상후 증상을 일으켰으며 2년이상 증상을 보인 경우도 2 례 있었다(Table 4).
수술받은 환자들의 형태학적 분류를 보면 혼합형, 분절형, 연속형 순으로 많았으며 국소형은 드믄 편이었다(Table 1).
증세가 없거나 경미한 경통을 호소하는 grade Ⅰ은 수술 에서 제외되어 사례가 없었으며, 상지의 방사통증을 호소하 는 grade Ⅱ는 7례, 경미한 척수장애나 운동마비가 있는 grade Ⅲ는 15례, 중등도의 척수손상이나 운동마비가 있는 grade Ⅳ는 10례, 심한 척수장애나 운동마비가 있는 grade
Ⅴ는 3례였다(Table 2).
Table 5. Postoperative results accoring to narrowing rate of spinal canal
Result Maximal narrowing
rate(%)
No. of
cases(%) Excellent Good Poor
-20 - - - -
21-30 17(48.6) 13 4 -
31-40 12(34.3) 10 2 -
41-50 3( 8.6) - 2 1
51-60 1( 2.8) - 1
61-70 2( 5.7) 1 1
Total(%) 35(100) 23(65.7) 9(25.7) 3(8.6) Fig. 2. Narrowing ratio of spinal canal.
Fig. 3. Pre-operative cervical spine CT scan and MRI showing the compressed spinal cord. Post-operative cervical spine lateral X-ray showing total excision of the OPLL after corpectomy and interbody fusion with iliac bone and Orion plate system.
임상 증세는 대부분의 환자들이 경통 및 상지의 감각둔화 나 저린감을 호소하였으며 운동마비가 77.1%, 감각이상이 22.8%, 소변장애 5.7%였으며 상지 방사통증(radiculopa- thy)이 77.1%에서 있었다.
경추강내 협착율은 Fig. 2와 같이 OPLL이 가장 두꺼운 부 위에서 OPLL의 두께를 척추강내 직경(척추후연에서 lamina line까지의 거리)으로 나누어 percentage로 산출하였다1). 대부분이 20~40%였으며, 60~70%까지 협착을 보이는 경 우도 2례가 있었다(Table 5). 수술전 시행한 CT 또는 MRI 에서 경추간반 탈출증이 동반된 경우가 14례(40.0 %)에서 있었다.
수술결과는 수술후 증상이 현저히 회복된 경우에“Exce- llent”증상이 호전되었으나 경미한 상지 방사통 이나 운동 장애가 남은 경우“Good”증상의 호전이 없거나 더 악화된 경우에는“Poor”로 분류하였다. 수술당시의 연령과 수술후 예후는 크게 상관 관계가 없으나 수술전 증세가 나타나기 까지의 기간이 짧을수록 증세호전이 좋고 호전기간도 짧았 으나 증세를 나타낸 기간이 길수록 증세호전이 없거나 회복 이 느렸다(Table 4).
후궁인대 골화에 의한 척추강 협착의 정도에 따른 수술결 과는 협착 정도가 심할수록 회복기간이 길었다(Table 5).
이상의 수술결과를 종합해보면 증상 호전이 없었던 3예 (8.6%)를 제외한 32예(91.4%)에서 현저한 증상호전을 보 이거나 경미한 상지 방사통이나 운동장애만 남는 비교적 만 족스러운 결과를 가져왔으며 장골을 이용한 자가골 이식후 Orion plate를 사용함으로써 환자들의 조기 보행이 가능하 게하고 높은 골 융합율을 보였다(Fig. 3).
고 찰
척추인대는 척추의 전연, 후연, 상하후궁판, 극돌기간에 붙 어서 척추의 상하관절에 의한 굴전, 신전, 회전등의 운동을 지지하여 주며 무리한 운동을 제한하여 준다. 1838년 Key 가 처음으로 Guys Hospital Reports를 통하여 척추인대가 골화될 수 있다고 보고한 이후 간헐적으로 OPLL에 대한 보고 있었으나 진단명도 각각 달랐으며 병리학적 해석도 달 랐다. 1960년 Tsukimoto14)가 경추의 골성 종양으로 진단 되어 수술받은 환자의 부검에서 경추 후종인대 골화증에 의 한 척수장애를 처음으로 보고하였으며 1964년 Terayama 는 이 질환을“ossification of the posterior longitudinal ligament(OPLL)”이라고 명명한13) 이후 이 질환에 대한 관 심이 높아졌고, 특히 일본에서 활발한 연구가 진행되어 왔 다7)8)12)13).
척추 후종인대는 해부학적으로 사대(clivus)로부터 천추(sa- crum)까지 척추체의 후면을 따라 위치하며 위쪽으로는 덮 개막(membrana tectoria)으로 이행된다. 이는 평활 아교섬 유(smooth collagen fiber)로 구성되어 있으며 경추부위에 서는 denticulate shape을 보이며 척추체 부위에서는 좁아 지며 추간판 부위에서는 넓어지는 형태를 보인다.
후종인대 골화의 원인에 대해서는 확실히 밝혀지지 않았
으나8)15)18) 원인요소로서 상기도 감염증(disseminated ph-
aryngeal infection), 성장 호르몬의 불균형(GH imbalance), 불소중독(fluoride intoxication), 당뇨병, 추간판 노화증(lo- calized disc degeneration), 반복적 외상(recurrent minor truma), 면역질환(immunologic disorders:HLA-Ag) 등 이 연구되고 있다8).
본 연구에서 경추부에 형성된 후종인대 골화증은 C5와 C6부위에 호발하는 것으로 나타났으며 이는 Kim 등이 35 예를 분석한 결과4)와 1987년 Tadao Nose 등이 74예를 분석한 결과11)와 일치하였다. 형태학적으로는 분절형과 혼 합형이 많은 것으로 나타났으며 여러 보고16)를 분석하여보 면 연속형은 상부 경추부에, 분절형은 하부 경추부에 많은 것으로 보고되고 있다. 환자들의 일반적인 특성은 타 문헌 의 통계와 비슷하였다2)6)7)9). 남녀의 성비는 4.8:1로 남자 에게 많았다.
연령별 분포를 보면 일반적으로 50대에서 호발(42.9%) 하고 있으며5) 증세가 나타날 때까지의 기간을 보면 1년 이 내에 나타나는 경우가 82.9%를 차지하고 있으며 대부분이 증세없이 지내다 가벼운 외상으로 증세가 나타난 것으로 보 아 경추 후종인대 골화증이 있는 환자에서 경미한 손상에도 쉽게 척수장애를 일으키는 것을 알수 있다. 경추 후종인대 골화증의 임상증상 등급에 따른 분류를 보면 grade Ⅱ 7례 (20.0%), grade Ⅲ 15례(42.8%), grade Ⅳ 10례(28.6%), grade Ⅴ 3례(8.6%)로 대부분의 환자들이 서서히 진행하 는 척수장애를 보였다(80.0%)(Table 1). 그리고 경부통증 과 상지의 감각둔화나 저린감은 거의 모든 환자에서 나타나 고 있으며 경추간반 탈출이 같이 동반된 경우(40.0%) 방사 통증이 더 심하게 나타났다.
수술적 치료는 임상증상 등급 grade Ⅱ이상에서 이루어 졌으며 전방경유 감압술 및 추체간 골융합술로 경추 추체를 제거한 뒤 척수장애의 직접원인인 골화된 후종인대를 직접 적으로 제거할 수 있으며 장골을 이용한 자가골 이식으로 추체간 융합을 한 뒤 환자의 조기보행 및 골융합율을 높이 기 위해 Orion plate system으로 고정하였다. 이 방법으로 치료받은 경추부 후종인대 골화증 환자 35예에서 증상 호 전이 없었던 3예(8.6%)를 제외한 32예(91.4%)에서 현저
한 증상호전을 보이거나 경미한 상지 방사통이나 운동장애 만 남는 비교적 만족스러운 결과를 가져왔으며 이번 조사에 서 환자의 예후에 관여하는 요소는 연령보다는 수술전 증상 의 기간과 골화에 의한 척추강 협착 정도였으며 수술전 증 상의 기간이 길수록, 골화에 의한 척추강 협착정도가 심할 수록 예후가 좋지 않은 것으로 나타났다.
결 론
1) 경추부 후종인대 골화증의 진단에는 골화의 정확한 부 위, 유형, 그리고 협착정도를 알수 있는 컴퓨터 단층 촬영이 매우 중요하다. 특히 골화에 의한 척추강 협착율에 따라 수 술후 예후를 예측할 수 있는 만큼 반드시 확인하는 것이 좋 겠다.
2) 본 연구에서 경추 후종인대 골화증으로 수술받은 35 명의 환자중 32명(91.4%)에서 만족할 만한 결과를 보이고 있으므로 임상등급 grade Ⅱ이상인 환자에서는 보존적 치 료보다는 적극적인 수술이 환자의 증상을 빨리 호전시킬 수 있다.
3) 예후와 환자의 연령, 증상 발현기간, 골화에 의한 척추 강 협착율 등의 관계를 보면 증상 발현기간이 1년 이하였던 29명의 환자중 28명(96.6%)이 수술후 만족할 만한 결과 를 보여주었고(Table 4), 척추강 협착율이 50% 이하였던 32명의 환자중 31명(96.9%)이 수술후 만족할 만한 결과 를 보여주었으며(Table 5) 증상 발현기간과 골화에 의한 척 추강 협착율과 결과의 연관성을 알아보기 위해 CMH(Co- chran-Mantal-Haenszel) χ2-test를 실시한 결과 p=0.001 (Non-zero correlation)로 통계적으로 유의한 결과를 보 여, 증상 발현기간이 짧을수록, 척추강 협착율이 낮을수록 예후가 좋으며 환자의 연령은 예후와 크게 관계가 없어 고 령이라도 수술 적응증이 되면 수술을 하는 것이 좋을 것으 로 사료된다.
•논문접수일:1999년 7월 6일
•심사완료일:1999년 9월 10일
•책임저자:심 상 준
400-130 인천광역시 중구 율목동 237번지 인천기독병원 신경외과
전화:032) 762-7831, 전송:032) 773-4877 E-mail:[email protected]
References
1) Abe H, Tsuru M, Ito T, et al:Anterior decompression for
ossification of posterior longitudinal ligament of the cervical spine. J Neurosurg 55:108-116, 1981
2) Chin WS, Oon DI:Ossification of the posterior longitudinal ligament of the spine. Brit J Radiol 52:865-869, 1984 3) Griffith R, Horsh Ⅳ, George W, et al:Cervical spine steno-
sis secondary to ossification of posterior longitudinal ligament.
J Neurosurg 67:349-357, 1987
4) Kim YS, Kim SH, Lee JK:Cervical Myelopathy caused by Ossification of the Posterior Longitudinal Ligament. J Kor Neurosurg Soc 12:751-758, 1983
5) Malcolm D, Jones M, Joyce Pais, et al:Bony overgrowth and abnormal calcification about the spine. Radiologic Clinics of North America 26:1213-1234, 1988
6) Nagashima C:Cervical myelopathy due to ossification of the posterior longitudinal ligament. J Neurosurg 37:653-660, 1972 7) Okamata Y, Yasuma Y:Ossification of posterior longitudi- nal ligament of the cervical spine with or without myelopathy.
J Jap Orthop Asso 40:1349-1360, 1967
8) Ono K, Ota H, Tada K, et al:Ossifed Posterior longitudinal ligament:A Clinicopathologic study. Spine 2:126-138, 1977 9) Scoville WB:Cervical spondylosis treated by bilateral face- tectomy and laminectomy. J Neurosurg 18:423-428, 1961 10) Shunji M, Takashi S, Eiji T, et al:The natural course of
myelopathy caused by ossification of posterior longitudinal ligament in the cervical spine. Clinical Orthopaedics and re- lated research 305:168-177, 1994
11) Tadao Nose, Taihei Egashira, Takac Enomoto, et al:Ossi- fication of the posterior longitudinal ligament. A clinical-ra- diological study of 74 cases. J Neurol Neurosurgery and Psy- chiatry 50:321-326, 1987
12) Terayama K:The ossification of the cervical ligament. J Jap Orthop Ass 50:415-442, 1976
13) Terayama K, Maruyama S, Miyashita R, et al:Ossification of the posterior longitudinal ligament in the cervical spine.
Orthop Surg 15:1083-1095, 1964(Jap)
14) Tsukimoto H:A case report:Autopsy of syndrome of com- pression of spinal cord of cervical spine. Arch Jap Chir 29: 1003-1007, 1960
15) Tsuyama N:Disease designations by Ministry of Health and Welfare. Report of the proceedings of studies of the Research Commitee on Posterior Longitudinal Ligament Ossification.
Tokyo, Ministry of Health and Welfare, 1975(Jap)
16) Tsuyama N:Ossification of the posterior longitudinal liga- ment of the spine. Clin Orthop 184:71-83, 1984
17) Wan CC, Chen NC, Tai NL, et al:Surgical treatment for ossification of posterior longitudinal ligament of the cervical spine. Surg Neurol 41:90-97, 1994
18) Yamaura I, Takayama M:Pathological study of cervical postrior longitudinal ligament. J Jap Orthop Ass 42:688- 689, 1966