INTRODUCTION
Residual astigmatism is the component of total ocular astigmatism that is not attributed to the ante- rior corneal surface.1,2Dunne and Elawad3reported that phakic eye possesses approximately 0.5D of residual astigmatism and that it was predominantly against-the-rule (83% of right eyes and 66% of left eyes). Furthermore, residual astigmatism was not significantly affected by gender or race. They applied the principle of astigmatic decomposition. 4,5
In 1890, Emile Javal proposed the following rule for predicting the subjective correction for astigma- tism on the basis of keratometric astigmatism:
Refractive (total) astigmatism = 1.25 × corneal
astigmatism + (-0.50 × 90). The modification sug- gested by Grosvenor et al6 is: Refractive (total) astigmatism = 1.00 ×corneal astigmatism + (-0.50 × 90). 0.5D of against-the-rule was suggested to account for residual astigmatism. Other authors reported similar results.7-10 When performing cataract surgery as refractive surgery, pseudophakic residual astigmatism may be considered to minimize postoperative refractive astigmatism.
MATERIALS AND METHODS
We examined 110 eyes of 87 patients who had undergone phacoemulsification and posterior cham- ber intraocular lens (IOL) implantation between January 2000 and September 2003. Exclusion crite- ria was a history of ocular disease or intraocular surgery, glaucoma, or significant posterior segment pathology that could preclude the postoperative visual outcome and any surgical complication such as continuous curvilinear capsulorhexis (CCC) rim tear, zonular dehiscence, failure to place the IOL in Vol. 18:116-120, 2004
Pseudophakic Residual Astigmatism
Jung Gn Bae, MD, Sung Jin Kim, MD, Young In Choi, MD*
Department of Ophthalmology, Eulji University College of Medicine,
*Hana Eye Center, Seoul, Korea,
We investigated pseudophakic residual astigmatism in order to minimize postop- erative refractive astigmatism. We examined 110 eyes of 87 patients who had under- gone phacoemulsification with small incision and posterior chamber intraocular lens (IOL) implantation. Corneal astigmatism was measured using an autokeratometer (RK-5, canon), refractive astigmatism by manifest refraction, and residual astigma- tism by vector analysis. Mean pseudophakic residual astigmatism was +0.47 ×176°, predominantly against-the-rule. Variations of pseudophakic residual astigmatism according to sex, age and IOL type were not statistically significant. When perform- ing cataract surgery as refractive surgery, we may consider that pseudophakic resid- ual astigmatism is approximately 0.50D against-the-rule.
Key words: refractive cataract surgery, pseudophakic residual astigmatism, corneal astig- matism, refractive astigmatism, against-the-rule
Reprint requests to Sung Jin Kim, MD, Department of Ophthalmology, Eulji General Hospital, #280-1 Hagye-1- dong, Nowon-gu, Seoul 139-711, Korea.
This paper was presented in part at the 90th annual meeting of the Korean Ophthalmological Society, October 2003.
the capsular bag, posterior capsular rupture, or vitre- ous loss.
All operations were performed by one surgeon (YI Choi) using a standard phacoemulsification technique. Topical anesthesia was used in all cases.
Before surgery, the pupils were dilated by topical instillation of phenylephrine hydrochloride 2.5%
and tropicamide 1.0%. A 3.0 mm limbal incision or clear cornea incision was made on the steep corneal meridian and the anterior chamber was reformed with viscoelastic material. CCC was performed with an approximately 5.0-mm diameter incision made using a bent 26-gage needle and CCC forceps.
Following hydrodissection and hydrodelineation, phacoemulsification of the nucleus and cortical aspiration were performed. After the lens capsule was inflated with viscoelastic material, the main incision was extended a littile, but not more than 3.2 mm. IOL was inserted in the capsular bag with injector mode. Foldable silicone IOL (SILENS 6, Bausch & Lomb) was injected for 61 eyes and fold- able acrylic IOL (SENSAR AR40e, AMO) for 41 eyes.
Corneal astigmatism was measured using an autokeratometer (RK-5, canon), with the mean value from three repeat values being selected.
Refractive astigmatism was measured by manifest refraction using retinoscopy and Jackson cross- cylinder ± 0.25D after at least 2 weeks postopera- tively.11,12 Residual astigmatism was calculated by vector analysis and then analyzed.13-15
With-the-rule corneal astigmatism included flat- test corneal meridian (minus cylinder) along 180° ± 30°, while against-the-rule astigmatism included flattest corneal meridian (minus cylinder) along 90°
± 30°.
For statistical analysis, independent T-test, ANOVA and multivariate analysis were done using SPSS program.16 P-value < 0.05 was considered significant.
RESULTS
Forty patients were male and 49 eyes were the right eye. The mean age at the time of the surgery was 65.6 ± 12.8 (range, 34-85) years. Power of pre- operative corneal astigmatism was predominantly less than 1.0D (Fig. 1), and 46 eyes were against-
the-rule (Fig. 2). Mean postoperative corneal astig- matism was +0.29 D × 96°, mean postoperative refractive astigmatism was +0.20 D × 165°, and mean pseudophakic residual astigmatism was +0.47
×176°. Axis distribution of pseudophakic residual astigmatism was predominantly against-the-rule (Fig. 2). Power of pseudophakic residual astigma- tism was predominantly less than 1.0D (Fig. 1).
Variations of pseudophakic residual astigmatism according to sex, age and IOL type were not statisti- Fig. 1. Power distribution of preoperative corneal astigmatism and pseudophakic residual astigmatism.
Fig. 2. Axis distribution of preoperative corneal astig- matism and pseudophakic residual astigmatism.
ATR: against-the-rule astigmatism.
WTR: with-the-rule astigmatism.
OBL: oblique astigmatism.
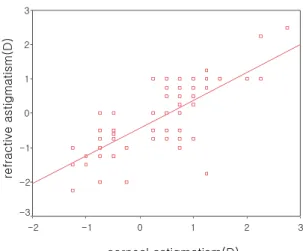
cally significant (Tables 1-3). To determine the rela- tion between refractive and corneal astigmatism of pseudophakia, we performed linear regression analysis for 81 eyes, after excluding 29 eyes of oblique astigmatism.
The linear regression equation had the form:
Refractive (total) astigmatism = 0.81 × corneal astigmatism + (-0.43 × 90), R = 0.75, P < 0.001 (Fig. 3).
DISCUSSION
Recently, refractive cataract surgery has become widely used in ophthalmology. The term implies a coordinated and encompassing attention to both
spherical and astigmatic components of refraction.17 The refractive cataract surgeon knows the astigmat- ic effects of various approaches and selects a surgi- cal plan that optimizes the refractive outcome for an individual patient.17In addition to the cataract inci- sion, whose size, location and configuration help determine the astigmatic effects of surgery, the cataract surgeon now has two additional options for correcting astigmatism: corneal relaxing incisions (CRIs) and toric IOLs. CRIs can be characterized as those made in the corneal midperiphery, co-called astigmatic keratotomy (AK), and those made peripherally, so-called peripheral or limbal corneal relaxing incisions (PCRIs).17 However, cataract Table 1. Pseudophakic residual astigmatism according to sex
Sex Eyes Mean Cylinder
C0* C45** Mean Cylinder Axis
Absolute value(D) Vector(D) (°)
Male 40 0.68 0.550 0.040 0.551 177.9
Female 70 0.65 0.391 0.045 0.394 176.7
P value P = 0.77*** P = 0.37***
*: Cylinder ×cos2Axis(°), **: Cylinder ×sin2Axis(°), ***: Independent T-test, ****: Multivariate analysis
Table 2. Pseudophakic residual astigmatism according to age
Age Eyes Mean Cylinder absolute value(D) C0 C45
≤50 16 0.52 0.39 0.10
51-60 15 0.66 0.59 -0.01
61-70 37 0.72 0.54 -0.04
71-80 23 0.68 0.36 -0.18
≥81 17 0.63 0.29 -0.31
Total 110 0.66 0.49 -0.04
P value P = 0.71* P = 0.30**
*: ANOVA, **: Multivariate analysis
Table 3. Pseudophakic residual astigmatism according to IOL type
IOL Eyes Mean Cylinder C0 C45 Mean Cylinder Axis
absolute value(D) Vector(D) (°)
SILENS 6 61 0.68 0.416 -0.072 0.422 175.0
SENSAR AR 40 49 0.64 0.490 -0.007 0.490 179.6
P value P = 0.66* P = 0.52**
*: Independent T-test, **: Multivariate analysis
surgery may be performed based on preoperative corneal astigmatism because the preoperative refrac- tive astigmatism is usually not known.
Pseudophakic residual astigmatism in which the lens is eliminated as one of the many reasons of residual astigmatism was not considered.
Mean pseudophakic residual astigmatism was +0.47 × 176°, predominantly against-the-rule (72%), and was similar to known phakic residual astigmatism. In addition, the simplified Javal’s rule by Grosvenor et al6 was similar to the relation between corneal astigmatism and refractive astigma- tism of pseudophakia.
These results indicated that residual astigmatism was not changed, even if the lens which was known as one of several causes of residual astigmatism was removed. Therefore, we conclude reason that crys- talline lens does not contribute greatly to residual astigmatism, or that left posterior capsule or inserted IOL may take the place of the lens part of residual astigmatism.
When performing cataract surgery as refractive cataract surgery, we may consider that pseudopha- kic residual astigmatism is approximately 0.50D against-the-rule in order to minimize postoperative refractive astigmatism.
REFERENCES
1. Lyle WA. Changes in corneal astigmatism with age.
Am J Optom Arch Am Acad Optom. 1971;48:467- 468.
2. Kim SJ, Choi O. A clinical study on residual astig- matism. J Korean Ophthalmol Soc. 1984;25:463-455.
3. Dunne MCM, Elawad MEA. A study of the axis of orientation of residual astigmatism. Acta Ophthalmol (Copenh). 1994;72:483-489.
4. Bennett AG. A new approach to the statistical analy- sis of ocular astigmatism and astigmatic prescrip- tions. The Frontiers of Optometry: First Internation- al Congress 2. 1984:35-42.
5. Bennett AG, Rabbetts RB. Clinical Visual Optics.
London: Butterworth; 1989:105-106.
6. Grosvenor T, Quintero S, Perrigin DM. Predicting refractive astigmatism: a suggested simplification of Javal’s rule. Am J Optom Physiol Opt. 1988;65:292- 297.
7. Grosvenor T, Ratnakaram R. Is the relation between keratometric astigmatism and refractive astigmatism linear? Optom Vis Sci. 1990;67:606-609.
8. Elliott M, Callender MG, Elliott DB. Accuracy of Javal’s rule in the determination of spectacle astigma- tism. Optom Vis Sci. 1994;71:23-26.
9. Keller PR, Collins MJ, Carney LG, Davis BA, Saarloos PPV. The relation between corneal and total astigmatism. Optom Vis Sci. 1996;73:86-91.
10. Lam AKC, Chan CCY, Lee MH, Wong KM. The aging effect on corneal curvature and the validity of Javal’s rule in Hong Kong Chinese. Curr Eye Res.
1999;18:83-90.
11. Oshika T, Tsuboi S. Astigmatic and refractive stabi- lization after cataract surgery. Ophthalmic Surg.
1995;26:309-315.
12. Masket S, Tennen DG. Astigmatic stabilization of 3.0mm temporal clear cataract incisions. J Cataract Refract Surg. 1996;22:1451-1455.
13. Hollady JT, Cravy TV, Koch DD. Calculating the surgically induced refractive change following ocular surgery. J Cataract Refract Surg. 1992;18:429-443.
14. Hollady JT, Dudeja DR, Koch DD. Evaluating and reporting astigmatism for individual and aggregating data. J Cataract Refract Surg. 1998;24:57-65.
15. Hollady JT, Moran JR, Kezirian GM. Analysis of aggregate surgically induced refractive change, pre- diction error, and intraocular astigmatism. J Cataract Refract Surg. 2001;27:61-79.
16. Naser K, Hjortdal JØ. Bivariate analysis of surgically induced regular astigmatism. Mathematical analysis and graphical display. Ophthal Physiol Opt.
1999;19:50-61.
17. Lindstrom RL, Koch DD, Osher RH, Wang L.
Control of astigmatism in the cataract patient. In:
Fig. 3. Linear regression: Pseudophakic refractive astigmatism and corneal astigmatism.
Steinert RF, ed. Cataract Surgery: Technique, Com- plication, and Management, 2nd ed. Philadelphia:
Saunders; 2003:253-266.