258
서 론
유방암은 미국의 여성암 중 1위를 차지하고 있으며, 일본 과 우리 나라에서도 공히 1위를 차지하고 있다. 인구 비례 로 보면 우리 나라의 유방암은 미국의 4분의 1수준으로서, 일본보다 약간 낮은 발생률을 보이며, 세계적인 발생률보 다도 약간 낮은 상태이다. 그러나, 현재 급격히 증가하고 있 으며, 이러한 추세는 한동안 계속될 것으로 전망하고 있다.
처음 진단되는 유방암의 80%는 유방과 액와림프절에 국한 된 operable breast cancer이며, 이들의 약 반수는 결국 전이 에 의해서 사망하게 된다. 즉 처음 진단될 당시 대개 병기 1∼2이며, 국소 및 전신치료 후에도 재발률은 처음 병기에 비례해서 증가한다. 특히 병기 4의 경우 무병생존은 거의 드물지만, 약 10∼20%의 환자는 최소의 잔존질환(minimal disease)을 가지면서 5∼10년 정도의 장기 생존을 보인다.
이것이 바로 disease control의 개념이며, 전이성 유방암 환 자의 궁극적인 치료 목표이다. 전이성 유방암 환자에서 완 치는 현재로선 힘든 실정이며, disease control을 통한 생명 연장과 삶의 질(QOL) 향상에 그 치료의 목적이 있다. 일단
Taxane 저항성 전이성 유방암 환자에서 Capecitabine (Xeloda
Ⓡ) 단독 화학요법의 효과
충남대학교 의과대학 외과학교실 김 제 룡․장 일 성
책임저자:장일성, 대전광역시 중구 대사동 640번지 ꂕ 301-721, 충남대학병원 외과
Tel: 042-220-7179, Fax: 042-257-8024 E-mail: [email protected]
접수일:2005년 1월 31일, 게재승인일:2005년 4월 11일
Capecitabine Monotherapy in Taxane-Refrac- tory Metastatic Breast Cancer (MBC) Patients
Je-Ryong Kim, M.D. and Eil-Sung Chang, M.D.
Purpose: The therapeutic options for MBC patients who have been previously treated with taxane and anthracycline are limited. Capecitabine (XelodaⓇ) is a novel tumor- selective oral fluoropyrimidine, and it provides effective and well tolerated therapy for patients with MBC who are resistant to or are failing with anthracycline and taxane therapy. We present our experiences with oral capecitabine that was given as monotherapy for taxane and anthracycline pre-treated MBC patients from CNU hospital.
Methods: The study subjects were 32 female patients having MBC that progressed after anthracycline and taxane treatment, and they were then treated with oral capecitabine monotherapy from 1999 to 2002. The median disease free survival period was 26 months. All the patients had good ECOG perfomance status (>2) and normal renal function.
The primary end points were the response rate, time to progression (TTP) and overall survival. The response rate was assessed with standard UICC criteria, and toxicity was assessed with NCI toxicity criteria.
Results: The sites of first metastasis were bone in 17 cases (53.1%); cervical LN 5 (15.6%); liver 3 (9.4%); lung 3 (9.4%);
chest wall 2 (6.3%); brain 1 (3.1%); and contralateral axillary LN 1 (3.1%). The clinical response rates to therapy were 1 case of CR (3.1%); 13 cases of PR (40.6%); 11 cases of stable disease (34.4%); 6 cases of progressive disease (18.8%). The median TTP was 6.0 months (95% CI: 5.53∼
8.47). The median overall survival was 15.0 months (95%
CI: 11.90∼16.10). Toxicities related to therapy were 5 cases of hand-foot skin reaction (15.6%); 3 cases of diarrhea
(9.4%); and 1 case of stomatitis (3.1%). There was no bone marrow depression or alopecia. All treatment related toxi- cities were improved by a short period of drug interruption or dose reduction (2,500 mg/m2/day to 2,000 mg/m2/day).
Conclusion: Taxane resistant MBC has a poor prognosis.
Oral capecitabine monotherapy provided activity in this subgroup of patients with an overall response rate of 43.7%
and a stable disease rate of 34.4%. Oral capecitabine is well tolerated with an acceptable toxicity profile in this population.
(J Korean Surg Soc 2005;68:258-263)
Key Words: Metastatic Breast cancer, Capecitabine, Taxane 중심 단어: 전이성 유방암, 카페시타빈, 탁산 ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ Department of Surgery, College of Medicine, Chungnam National University (CNU), Daejeon, Korea
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ 전이성 유방암으로 진단받은 경우 평균 생존기간은 18∼30
개월 정도이다.(1) 전이성 유방암 환자에서 항암화학요법은 20∼40% 정도의 반응률과, 6∼12개월 정도의 TTP (time to progression)를 보인다. 단일 약제로 30% 이상의 반응을 보 이는 약제로는 docetaxel, doxorubicin, epirubicin, paclitaxel, vinorelbine 등이 있다. 그리고 전이성 유방암 환자의 치료에 있어 전망을 밝게 하는 많은 신약들이 현재 연구 중에 있다.
여기에는 많은 면역학적인 치료전략과 전이에 관여하는 enzyme inhibitor 등이 있다. Anthracycline 저항성 전이성 유 방암 환자에서 taxane 및 vinorelbine의 사용이 증가하고 있 지만, 특이 taxane 저항성인 경우 새로운 항암제가 요구된 다. Capecitabine은 전이성 유방암 환자에서 taxane 저항성인 경우 20%의 반응을 보이고, anthracycline 저항성인 경우 36%의 좋은 반응을 보이며, 경구약으로서 투여 중 골수기 능저하 및 탈모가 거의 없다는 장점을 가지고 있다.(2,3) 이 러한 배경으로 경구 항암제 capecitabine의 도입은 말기 유 방암 환자에서 또 한 번의 새로운 선택의 계기를 마련하였 다. 저자들은 국내에 capecitabine이 도입된 지 불과 몇 년이 지난 시점에서, 전이성 유방암 환자에서의 효과와 독성 반 응 및 처치 등을 정리하여 고찰해보고자 한다.
방 법
대상 환자들은 1993년 2월부터 2001년 7월까지 유방암을 진단받고, 수술을 시행받았거나 수술받지 않고 지내던 중 전이가 발견된 32명의 전이성 유방암 환자로서, 전에 anthracycline 및 taxane을 투여받은 병력이 있다. 이들은 모 두 ECOG 2 이상이면서, 신기능의 장애가 없었다. 저자들은 1999년부터 2002년까지 capecitabine을 투여받은 전이성 유 방암 환자에서 이의 효과, 그리고 치료 중 발생한 합병증 및 처치에 대해 고찰하였다. Capecitabine의 효과는 객관적 반응률, TTP, 전체 생존율 등으로 평가하였다. 2주기의 capecitabine 투여를 마친 뒤 2주 후 전이부위의 전산화단층 촬영 혹은 초음파검사, 단순흉부사진 및 이학적 검사를 통 해 화학요법 전후 종양의 크기를 비교하여 종양의 최장축 과 그에 수직인 축을 곱한 값에 따라 standard UICC criteria 를 적용하여 반응도를 평가하였으며, 생존율은 Kaplan- Meier statistical method를 사용하여 구하였다.
결 과
1) 환자들의 임상병리학적 특성
전이가 발견되기 전 처음 수술받을 당시 환자들의 병기 는 T1 4예(13.3%); T2 16예(50.0%); T3 10예(31.3%); un- known 2예(6.3%)였으며, 림프절 전이는 없었던 경우 4예 (12.5%); 1∼3개 6예(18.8%); 4∼9개 11예(34.4%); 10개 이상 8예(25.0%); unknown 3예(9.4%)였다. 수술은 23예(71.9%)에
서 유방절제술, 8예(25.0%)에서 유방보존수술을 시행하였 으며, 1예(3.1%)는 본인의 거부로 수술을 시행받지 않았다.
수술 후 보조요법으로서 23예(71.9%)에서는 anthracycline based chemotherapy (adriamycin, epirubicin)를 시행받았고, 5 예(15.6%)는 MMM (mitoxantrone, methotrexate, mitomycin), 2예(6.3%)는 CMF (cyclophosphamide, methotrexate, 5-Fu)를 시행받았으며, 1예 (3.1%)는 보조화학요법을 시행받지 않았 다. 환자들의 평균 나이는 50.4세(30∼70세)였으며 평균 활 력지수는 ECOG 1 (range 1∼2)이었고, 평균 무병기간은 33.0개월(6∼78)이었다(Table 1). 보조화학요법시행 후 처음 전이된 부위는 뼈 17예(53.1%); 경부림프절 5예(15.6%); 폐 3예(9.4%); 피부 2예(6.3%); 간 3예(9.4%); 뇌 1예(3.1%); 반 대측 액와림프절 1예(3.1%)순으로 많았으며, 대부분의 환자 들은 진행되면서 결국 여러 장기에 다발성 전이를 보였다 (Table 1).
Table 1. Clinical characteristics of the patients ꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚ Mean age±SD (range) 50.4±10.8 (34∼70) Menopausal status
Premenopausal 21 (65.6%)
Postmenopausal 11 (34.4%)
Disease free survival period (months)
<10 4 (12.5%)
11∼20 9 (28.1%)
21∼30 5 (15.6%)
31∼40 3 (9.4%)
41∼50 5 (15.6%)
51∼60 4 (12.5%)
61∼70 1 (3.1%)
71∼80 1 (3.1%)
First metastatic site
Bone 17 (53.1%)
Lung 3 (9.4%)
Liver 3 (9.4%)
Cervical LN 5 (15.6%)
Chest wall 2 (6.3%)
Brain 1 (3.1%)
Contralateral axillary LN 1 (3.1%) Radiotherpy after recurrence
Yes 20 (62.5%)
No 12 (37.5%)
ECOG perfomance status
0 5 (15.6%)
1 21 (65.6%)
2 6 (18.8%)
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ SD = standard deviation; LN = lymph node; ECOG = eastern coope- rative oncology group.
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
2) 치료
첫 전이가 발견된 후의 항암요법은 전에 술 후 1차 보조 화학요법으로서 anthracycline을 투여받은 25예(78.1%)의 환 자에게는 2차 화학요법으로서 taxane (TaxolⓇ 혹은 TaxotereⓇ) 과 non-anthracycline (cisplatin, gemcitabine, vinorelbine)의 병 합요법을 시행하였고, anthracycline을 투여받지 않은 7예 (21.9%)의 환자는 taxane과 adriamycin의 병합요법을 시행하 였다(Table 1). Taxane 치료 중 병변이 진행하거나, 새로운 병변이 나타날 경우 taxane 저항성으로 인정하고 3차 화학 요법으로서 capecitabine의 경구 투여를 시작하였다. Capeci- tabine의 투여는 2,500 mg/m2을 하루 두 번 나누어 2주간 투 약하고 1주 쉬는 것을 1주기로 하였다. 또한 ER (+)인 18예 (56.2%)의 폐경기 후 여성에서는 aromatase inhibitor인 ArimidexⓇ를 추가하였고, 골전이가 있었던 17예(53.1%)에 서는 bisphosphonate를 병용하였다. 특히 골전이에 의한 통 증을 호소한 11명(34.4%)의 환자와는 척추 및 골반에 대하 여 방사선 치료를 시행하였으며, 그 외 흉벽 및 경부림프절 전이에 대하여도 방사선 치료를 시행하였다. 또한 capeci- tabine의 투여는 전이부위의 병변이 진행할 때까지 계속하 였고, 투약한 평균기간은 10.2주기(1∼31주기)였다.
3) 약물치료에 대한 반응도 평가
Capecitabine에 대한 response는 2 cycle 후에 평가하였고, 측정 가능한 병변(measurable disease)이 있는 경우 주로 초 음파 검사, CT scan 소견 등을 참고하였고, 측정 가능한 병 변이 아닌 경우(unmeasurable disease), 즉 bone metastasis, lymphangitic lung metastasis가 있는 경우는 CEA, CA15-3 등 의 tumor marker와 chest PA, 골주사검사 등을 참고로 하였 다. 반응을 평가할 수 있었던 31예에서 임상적 반응도는 CR 1예(3.1%); PR 13예(40.6%); stable disease 11예(34.4%); pro- gressive disease 6예(18.8%)였다(Table 2).
4) 생존율 분석
Capecitabine 투여시점부터 종양이 진행할 때까지의 기간
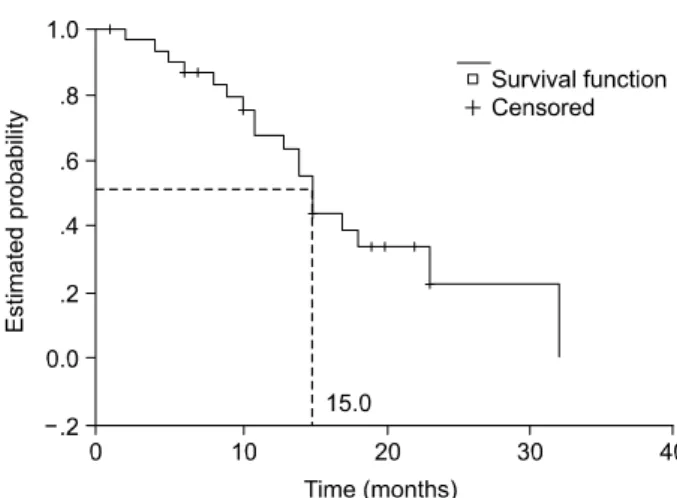
을 TTP라고 하였을 때, median TTP은 6.0개월(95% CI: 5.5 3∼8.47)이었다(Fig. 1). 역시 capecitabine 투여시점부터 환 자가 사망할 때까지의 기간을 전체생존율이라 보았을 때 median OS은 15.0개월(95% CI: 11.90∼16.10)이었다(Fig. 2).
5) 치료 중 독성 및 처치
부작용의 평가는 NCI toxicity criteria에 의거하여 분류하였 는데, capecitabine 투여기간 중 발생한 부작용으로는 grade 1∼2 정도의 구내염 1예(3.1%), 설사가 3예(9.4%), grade 1∼
2 정도의 hand-foot skin reaction이 5예(15.6%)에서 발생하였 고, 골수기능저하 및 탈모증은 없었다(Table 3). 특히 흔한 부작용인 hand-foot skin reaction에 대해서는 손 발바닥에 발 적, 각질박리 이외에 통증이 동반되는 경우 grade 2 이상으 로 보고, 약물을 일시 중단 후 증상 치료로 보습제와 Vit B6 200 mg/day을 처방하였으며, 이후 다시 시작하는 투여 용량을 2,500 mg/m2/day에서 2,000 mg/m2/day로 감량하였다.
즉 감량이 필요한 경우는 3예 있었고, 감량까지의 중앙 기
Table 2. Clinical response* to oral capecitabine monotherapy (n=32)
ꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚ
Clinical response No (%)
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
Complete response 1 (3.1)
Partial response 13 (40.6)
Stable disease 11 (34.4)
Progressive disease 6 (18.8)
No data 1 (3.1)
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
*according to standard UICC criteria. Fig. 2. Overall survival; median OS=15 months.
Fig. 1. Time to progression; median TTP=6 months.
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
간은 1.0개월이었다. 이러한 투약중의 부작용들은 약물투여 일시중단 및 감량으로 모두 호전되었다(Table 3).
고 찰
Capecitabine은 thymidine phosphorylase (TP) pathway를 통 한 종양 선택성과 경구복용이라는 커다란 장점이 있다. 경 구복용이면서도 5-FU의 지속적인 정주와 흡사한 작용기전 을 보이는 점이 또 하나의 장점이다. Capecitabine은 변화되 지 않은 상태로 장점막을 신속하게 통과하여, 간에서 5-FU 전구체로 변환되고, 이것은 종양조직에서 가장 중요한 효 소인 TP에 의해 5-FU로 대사된다. Capecitabine의 중간대사 물질은 세포독성을 나타내지 않으며, 오로지 종양조직에서 5-FU로 대사되어야만 세포독성을 가진다. 이것이 바로 capecitabine이 종양 선택성을 가지는 중요한 이유이다.
Shiller 등은 capecitabine의 종양 선택성을 증명하기 위해, capecitabine 투여군과 5-FU 정주한 두 군 간에 혈장, 정상조 직 및 종양조직에서의 5-FU 농도를 비교하였다. Capeci- tabine 투여군에서는 종양조직에서 5-FU 농도가 혈장에 비 해 21배가 높았으며, 정상조직과 비교하면 3배 이상의 차이 를 보였다. 그러나 5-FU 정주한 군에서는 전혀 종양 선택성 을 보이지 않았다. 이러한 종양 선택성은 바로 TP가 종양조 직에서 높은 활성을 보이기 때문이다. Miwa 등은 유방암, 직장대장암, 위함, 자궁암, 자궁경부암, 난소암, 그리고 방 광암에서도 주변의 정상조직에 비해 TP 활성이 의미 있게 높았음을 증명하였다.(4-6) TP 활성을 증가시키는 여러 인 자들이 보고되고 있다. Hypoxia, cytokine, radiation, 그리고 몇가지의 cytotoxic agent들이 있다. 이러한 cytotoxic agent들 에는 유방암에 많이 쓰이는 paclitaxel, docetaxel, mitomycin C, cyclophosphamide 등이 있다. 이들을 capecitabine과 병합 했을 때 상승효과가 예상되고, 실제로 많은 임상시험들에 서 이들 항암제와 capecitabine의 병합화학요법이 진행 중에 있다. 현재 유방암에서 capecitabine의 위치는 단독 경구요 법이 전에 taxane을 치료받았던 전이성 유방암 환자들에서 표준요법으로 자리를 잡았고, 더 나아가서는 현재 진행되 고 있는 여러 임상시험을 통해 보조요법 혹은 전이성 유방
암에서, 또 일차요법 혹은 그 이후의 구제요법에서, 또 병합 혹은 순차적 요법에서의 capecitabine의 역할이 규명되어야 하겠다.
전이성 유방암 환자의 치료에서 anthracycline 제재를 포 함하는 병용요법을 사용한 후 진행되는 경우에는 taxane을 추가 투여하는 것이 근래의 경향이지만, 최근에는 이들 약 제를 술 후 보조요법에 사용하는 시도가 이루어지고 있다.
특히 이들 두 약제를 사용한 후 재발한 전이성 유방암의 경우, 다음 약제의 선택에 상당한 어려움을 겪게 된다. 또한 이러한 경우 치유의 목적보다는 종양과 연관된 증상의 경 감, 삶의 질 차원에서 접근해야 하므로 항암제의 선택은 중 요하다.(7-9) 최근 개발된 capecitabine (XelodaⓇ)은 이러한 경우에 좋은 기회를 제공한다. Anthracycline 및 taxane을 이 미 투여받은 전이성 유방암에 대한 capecitabine 단독요법은 126명의 환자를 대상으로 시행한 제 2상 임상연구에서 유 용성이 입증되었다.(10) 이 연구에서 capecitabine 2,500 mg/m2 을 하루 두 번 나누어 14일간 투여하고 7일간 쉬는 것을 1주 기로 하였을 때, 28%의 객관적 종양 반응률, 4.9개월의 TTP, 중앙 생존기간 15.2개월을 보고하였다.(10-14) 특히 capeci- tabine과 taxane을 병합투여했던 phase II 임상시험에서는 관 해율을 40∼50%까지 보고하고 있다. 전 세계적으로 75개의 센터에서 anthracycline 치료에 실패한 511명의 전이성 유방 암 환자를 대상으로 한 임상시험이 시행되었다.(15) 환자들 은 두 군으로 나뉘었는데 225명은 capecitabine (1,250 mg/m2 twice daily for 14 days, followed by 1 week without treatment) 과 docetaxel (75 mg/m2 as 1 hour IV infusion, 3 week cycles) 을 병합 투여하였고, 256명은 docetaxel (100 mg/m2 IV infusion, 3 week cycles)을 단독 투여하였다. 결과는 병합투 여군에서 더 높은 관해율(32% vs 22%)을 보였으며, median time to progression (6.1 vs 4.2 months), 전체 중앙생존율(14.5 vs 11.5 months)에서도 더 좋은 결과를 보였다. 부작용은 설 사(67% vs 48%), 구내염(67% vs 43%), hand-foot skin reaction (63% vs 8%) 등으로 병합투여군에서 더 많이 나타 났다. 부작용으로 용량조절이 필요했던 경우는 병합투여군 에서 65%, 단독투여군에서 36%였다. Anthracycline 저항성 인 전이성 유방암 환자에서 capecitabine (X)과 docetaxel (T) Table 3. Toxicities (according to NCI toxicity criteria)
ꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚ
Adverse affect Grade No (%) Action outcome
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
Hand-foot skin reaction 1 3 (9.4) - improved
2 2 (6.3) interrupt & DR* improved
Diarrhea 1 1 (3.1) - improved
2 1 (3.1) interrupt & DR* improved
Stomatitis 1 1 (3.1) - improved
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
*DR = dose reduction (2,500 → 2,000 mg/m2/day); NCI = national cancer institute.
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ 의 병합요법(XT)은 현재 FDA의 공인을 받은 상태이다. 이
외 여러 보고에서 capecitabine과 taxane의 병합요법으로 좋 은 성적을 발표하였다.(16,17) 그러나 최근까지는 병합요법 을 시행한 환자가 드물기 때문에, taxane 투여 후 진행하는 경우에 capecitabine 단독요법을 처방하는 것이 일반적인 경 향이다. 본 연구의 결과와 비교하면, 일단 관해율에서 큰 차 이를 보인다. 본 연구의 결과에서 객관적 관해율은 43.7%로 서 capecitabine과 docetaxel의 병합투여군의 32%보다도 높 게 나타났다. 또한 저자들의 결과와 capecitabine 및 doce- taxel의 병합투여군과 비교할 때 median time to progression (6.0 vs 6.1개월), 전체 중앙생존율(15.0 vs 14.5개월)에서 대 등한 결과를 보이고 있다. 이것은 아마도 저자들의 경우 호 르몬 수용체 양성인 18예(56.2%)의 폐경기 후 여성의 경우 aromatase inhibitor인 Arimidex를 병용처방한 결과로 보여진 다. 단 본 연구 대상 환자가 적기 때문에 향후 대상 환자를 확대하여 재규명이 필요할 것으로 생각된다. Capecitabine 단독 경구요법의 또 하나의 큰 장점은 부작용이 적다는 것 이다. 본 연구 대상 환자의 경우 설사(6.2%), 구내염(3.1%), hand-foot skin reaction (15.7%) 모두 capecitabine 및 docetaxel 병합투여군에 비해 현저히 적었다. 즉 capecitabine 단독 경 구요법은 관해율과 생존율 측면에서 capecitabine 및 doce- taxel의 병합치료군에 필적하는 좋은 결과를 보이는 반면, 부작용이 현저히 적다는 장점을 가져, 말기 유방암 환자에 게 매우 좋은 치료방법으로 생각된다. Capecitabine은 부작 용이 적은 약물이기도 하지만, 만일 부작용이 나타났다고 하더라도 신속하게 대처할 수 있다는 점이 더욱 안전성에 기여하고 있다. 복용 방법상 하루 2번, 14일간 투여하는 capecitabine의 한 주기동안 용량을 줄일 수 있는 기회가 이 론적으로는 27번이나 있다. 즉 약물 복용 전에 grade 2 이상 의 부작용이 나타날 경우, 복용을 일시 중단할 수 있다. 현 재 진행되고 있는 capecitabine의 모든 임상시험에서 부작용 에 대한 처치로 용량조절계획(dose modification schedule)을 가지고 있다. 용량조절의 목적은 같은 부작용이 다시 나타 나는 것을 피하고, 더 심한 부작용의 발생을 예방하며, 각자 에 맞게 조절된 용량으로 약물의 효과를 그대로 유지하는 것이다. Capecitabine의 용량조절의 예를 하나 들면, grade 2 이상의 부작용이 처음 나타났을 경우 약물을 일시 중단 후 시초용량을 그대로 사용한다. 두 번째에는 일시 중단 후 시 초용량의 75%로 감량 투여한다. grade 3의 경우는 처음부터 일시중단 후 시초용량의 75%로 감량 투여한다. 또 grade 2 라도 4번 이상 반복되거나, grade 3가 3번 이상 반복되면, capecitabine을 완전히 중단할 것을 권하고 있다. capecitabine 의 부작용은 본 대상환자들에서처럼 용량조절 후 대부분은 호전을 보인다. 하지만 극히 일부에서는 진행되거나 호전 되지 않는 경우도 있다. 특히 renal function은 부작용과 밀접 한 상관관계를 가지는데, grade 3 hand-foot skin reaction은 creatinine clearance (Ccr)가 낮을수록 빈발하는 경향이 있다.
그래서 Ccr의 계산치에 맞추어 시초용량을 조절해야 한다.
Ccr이 50 ml/min 이상이면 그대로 2,500 mg/m2/day을 사용 하고, 50 ml/min 이하면 1,900 mg/m2/day으로 줄이고, Ccr이 30 ml/min 이하면 capecitabine은 금기가 된다. 그러나 부작 용으로 인한 capecibabine의 용량감소는 종양의 진행에는 영 향이 없는 것으로 보고되고 있다.(18) 드물지만 capecibabine 은 coumadin과 약물 상호작용이 있으며, 5-FU 자체의 심장 독성이 일부에서 나타날 수 있기 때문에 주의를 요한다. 따 라서 환자의 교육이 중요한데, 이를 통해 환자 스스로가 부 작용을 감지할 수 있도록 하고 중등도 이상이라 생각되면 약물을 중단하고 의사와 상담하도록 교육받아야 한다.
결 론
본 연구에서 경구 capecitabine 단독요법은 anthracycline 및 taxane에 저항성인 전이성 유방암환자들에서 43.7%의 객 관적 반응율과 34.4%의 종양 안정화를 보였으며, 6.0개월의 median TTP 및 15.0개월의 생존율을 보였다. 또한 capeci- tabine은 경구 복용하므로 투여가 간편하고, 심한 부작용이 없어 활동지수가 떨어지는 말기 유방암 환자에서 유용한 치료가 될 수 있을 것으로 생각된다.
REFERENCES
1. Perez EA. Current management of metastatic breast cancer.
Semin Oncol 1999;26(suppl.12):110.
2. Liu G, Franssen E, Fitch M, Warner E. Patient preferences for oral versus intravenous palliative chemotherapy. J Clin Oncol 1997;15:110-5.
3. Payne SA. A study of quality of life in cancer patients re- ceiving palliative chemotherapy. Soc Sci Med 1992;35:1505-9.
4. Ishitsuka H, Miwa M, Takemoto K, Fukuoka K, Itoga A, Maruyama HB. Role of uridine phosphorylase for antitumor activity of 5'-deoxy-5-Fluorouridine. Gann 1980;71;112-3.
5. Suzuki S, Hongu Y, Fukazawa H, Ichihara S, Shimizu H.
Tissue distribution of 5'-deoxy-5-Fluorouridine and derived 5-Fluorouracil in tumor-bearing mice and rats. Gann 1980;71:
238-45.
6. Miwa M, Eda H, Fukuda H, Fujimoto K, Ishitsuka H. Com- parative studies on the antitumor activity of Fluorinated pyrimidines, 5'-DFUR, Tegafur, UFT and 5-FU, with various murine tumors. Jpn J Cancer Chemother 1988;15:1755-63.
7. Gianni L, Capri G. Experience at the Istituto Nazionale Tumori with paclitaxel in combination with doxorubicin in women with untreated breast cancer. Semin Oncol 1997;24(Suppl. 1):
S1-S3.
8. Luck HJ, Thomssen C, du Bois A, Untch M, Lisboa B, Kohler G, et al. Phase II study of paclitaxel and epirubicin as first-line therapy in patients with metastatic breast cancer. Semin Oncol
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ 1997;24:35-9.
9. Nabholtz JM, Senn HJ, Bezwoda WR, Melnychuk D, Des- chenes L, Douma J, et al. Prospective randomized trial of docetaxel versus mitomycin plus vinblastine in patients with metastatic breast cancer progressing despite previous anthra- cycline-containing chemotherapy. 304 Study Group. J Clin Oncol 1999;17:1413-24.
10. Fumoleau P, Largillier R, Clippe C, Dièras V, Orfeuvre H, Lesimple T, et al. Multicenter, phase II study evaluating capecitabine monotherapy in patients with anthracycline- and taxane-pretreated metastatic breast cancer. Eur J Cancer 2004;
40:536-42.
11. Blum JL, Smith SE, Buzbar AU, Lo Russo PM, Kuter I, Vogel C, et al. Multicenter phase II study of capecitabine in pacli- taxel-refractory metastatic breast cancer. J Clinl Oncol 1999;
17:485-93.
12. Blum JL, Dieras V, Lo Russo PM, Horton J, Rutman O, Buzdar A, et al. Multicenter, phase II study of oral capeci- tabine in taxane-pretreated metastatic breast carcinoma pa- tients. Cancer 2001;92:1759-68.
13. Cassidy J, Dirix L, Bissett D, Reigner B, Griffin T, Allman D, et al. A phase I study of capecitabine in combination with oral leucovorin in patients with intractable solid tumors. Clin Cancer Res 1998;4:2755-61.
14. Fumoleau P, Largillier R, Clippe C, Dieras V, Orfeuvre H,
Lesimple T, et al. Multicentre, phase II study evaluating capecitabine monotherapy in patients with anthracycline- and taxane-pretreated metastatic breast cancer. Eur J Cancer 2004;
40:536-42.
15. O'Shaughnessy J, Miles D, Vukelja S, Moiseyenko V, Ayoub JP, Cervantes G, et al. Superior survival with capecitabine plus docetaxel combination therapy in anthracycline-pretreated pa- tients with advanced breast cancer: phase III trial results. J Clin Oncol 2002;20:2812-23.
16. Talbot D, Moiseyenko V, van Belle S, O'Reilly SM, Alba Conejo E, Ackland S, et al. Randomised, phase II trial com- paring oral capecitabine (XelodaⓇ) with paclitaxel in patients with metastatic/advanced breast cancer pretreated with anthra- cyclines. British J Cancer 2002;86:1367-72.
17. O'Shaughnessy JA, Blum J, Moiseyenko V, Jones SE, Miles D, Bell D. et al. Randomized, open-label, phase II trial of oral capecitabine (XelodaⓇ) vs. a reference arm of intravenous CMF (cyclophosphamide, methotrexate and 5-fluorouracil) as first-line therapy for advanced/metastatic breast cancer. Annals of Oncology 2001;12:1247-54.
18. Procopio G, Bajetta E, Catena L, Alù M, Longarini R, Zilembo N, et al. Safety and activity of Capecitabine in elderly patients with advanced breast cancer. Eur J Cancer 2001;37(Suppl 6):
S197.