Received: 2013.8.16. Revised: 2014.1.1. Accepted: 2014.1.18.
Corresponding author: Ki Hyung Kim
Department of Obstetrics and Gynecology, Pusan National University School of Medicine, 179 Gudeok-ro, Seo-gu, Busan 602-739, Korea
Tel: +82-51-240-7287 Fax: +82-51-248-2384 E-mail: [email protected]
*These two authors contributed equally to this work.
Articles published in Obstet Gynecol Sci are open-access, distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.
org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Copyright © 2014 Korean Society of Obstetrics and Gynecology
Introduction
Endometrial adenocarcinoma is the most common gyneco- logic malignancy in the United States and Western Europe. In Korea, the incidence of endometrial cancer has been increas- ing in recent years: the age standardized incidence rate per 100,000 during 2010 was 5.0 [1]. The recent increasing prev- alence of risk factors is expected to result in a further increase in the incidence of this cancer.
Patients with endometrial cancer have a good progno- sis due to early detection resulting from postmenopausal
Tumor-infiltration of T-lymphocytes is inversely
correlated with clinicopathologic factors in endometrial adenocarcinoma
In Kook Jung 1* , Sun Sook Kim 2* , Dong Soo Suh 1 , Ki Hyung Kim 1 , Chang Hoon Lee 3 , Man Soo Yoon 1
1
Department of Obstetrics and Gynecology, Pusan National University Hospital, Pusan National University School of Medicine, and Biomedical Research Institute and Pusan Cancer Center,
2Department of Medicine, Pusan National University Graduate School of Medicine,
3Department of Pathology, Pusan National University School of Medicine, Busan, Korea
Objective
The aim of this study was to determine the distribution of T-lymphocytes and their relationship with clinicopathologic factors in endometrial carcinoma.
Methods
Samples were collected from 89 patients with endometrial endometrioid adenocarcinoma treated in Pusan National University Hospital from 2004 to 2011. Normal endometrial tissues were obtained from 30 hysterectomized women with benign adnexal masses and served as controls. Paraffin-embedded sections were immunohistochemically stained for CD8 (cytotoxic) and CD4 (helper) T-lymphocytes. The relationship of these cells with stage, histological grade, myometrial invasion, and lymph node metastasis was analyzed.
Results
The proportion of CD8+ and CD4+ lymphocytes in the endometrial endometrioid adenocarcinoma tissues was 67.4%
(60/89) and 44.9% (40/89), respectively, which was significantly higher (P<0.05) than in the control group. The extent of CD8+ lymphocyte expression was negatively correlated with histologic grade, myometrial invasion, and lymph node metastasis. The proportion of infiltration of the CD4+ lymphocytes was negatively correlated with histologic grade and myometrial invasion.
Conclusion
The high rate of infiltration of T-lymphocytes was negatively correlated with histologic grade, myometrial invasion, and lymph node metastasis. Our findings suggest that tumor-infiltrating T-lymphocytes may be used as pathologic prognostic factors in endometrial carcinoma.
Keywords: Clinicopathologic factors; Endometrial carcinoma; T-lymphocytes http://dx.doi.org/10.5468/ogs.2014.57.4.266
pISSN 2287-8572 · eISSN 2287-8580
bleeding. However, the prognosis for recurrent or metastatic endometrial cancer remains poor. An essential step for the im- provement of clinical outcomes is to understand the processes that inhibit and stimulate cancer progression [2].
Known prognostic factors in endometrial carcinoma include tumor stage, histologic grade, subtype, and vascular invasion [3]. In addition, changes in the immune system in the tumor microenvironment are considered one of the important fac- tors in the development and progression of cancer. Tumor- infiltrating lymphocytes are often found in human cancer.
Increasing evidence indicates that the high rate of infiltration of T-lymphocytes has been reported to be an indicator of good prognosis. A positive association between infiltrating CD8+ T cells and prognosis has been reported in various solid cancers such as colorectal and ovarian cancer [4,5]. However, the presence of tumor infiltrating lymphocytes (TILs) has not been fully assessed in endometrial cancer.
In the present study, we analyzed the tumor infiltration of CD8+ and CD4+ lymphocytes to determine whether the pres- ence of T-lymphocytes was associated with prognostic factors in endometrial carcinoma.
Materials and methods
1. Patients and tissue samples
A total of 89 patients diagnosed with endometrial endo- metrioid carcinoma who underwent surgery from 2004 to 2011 were selected from the archives of the Pusan National University Hospital for this study. All patients underwent a total abdominal hysterectomy and a bilateral salpingo- oophorectomy (BSO). Pelvic and/or para-aortic lymph node dissection was performed in the patients with more advanced disease or unfavorable histologic grade. Hematoxylin and eosin (H&E) stained sections were reviewed and reclassified by World Health Organization (WHO) guidelines. Histologic type, grade of differentiation, stage, and depth of myometrial invasion had previously been evaluated in the tissue materials.
This study was approved by the Ethical Review Committee of Pusan National University Hospital.
2. Immunohistochemistry
The tissue specimens were fixed in 10% formalin and embed- ded in paraffin. Sections, 4 μm in thickness, were deparaf- finized in xylene and rehydrated through a series of graded
ethanol. Endogenous peroxidase activity was blocked by incubation with 3% hydrogen peroxide in methanol for 10 minutes. Antigen retrieval was performed by microwaving the slides in citrate buffer (pH 6.0). The sections were then incubated at 4°C overnight with anti-Human CD4 antibody (rabbit monoclonal, SP35, 1:50; Spring Bioscience, Pleasan- ton, CA, USA), anti-Human CD8 antibody (mouse monoclonal, C8/144B, Dako, Glostrup, Denmark). Immunoreactivity was vi- sualized using 3,3’-diaminobenzidine (DAB, Dako-Cytomation, Glostrup). Slides were counterstained with Meyer’s hematoxy- lin. Human tonsil tissue for CD4 and skin for CD8 were used as positive controls.
3. Evaluation of staining
Each slide was evaluated independently by two pathologists who were blinded to clinical and outcome data. Three inde- pendent areas with the most abundant lymphocyte infiltration were selected, and the stromal lymphocytes were indepen- dently counted in each microscopic field at ×200. The average count for three areas was accepted as the number of TILs in each case [6].
4. Statistical analysis
Statistical analyses were conducted using SPSS ver. 15.0 (SPSS Inc., Chicago, IL, USA). The χ
2test and Fisher exact test were used to evaluate the correlation between the expression of CD4 and CD8 and the clinicopathologic parameters. P-values of <0.05 were considered statistically significant.
Results
1. Patients’ characteristics
The clinicopathological characteristics of the 89 patients are
presented in Table 1. The mean age of the patients was 61
years (range, 40–78 years). Patients with endometrial cancer
included 12 with premenopausal status and 77 with post-
menopausal status. Clinical follow-up was available for all
cases. The median follow-up period was 64 months (range,
8–84 months). Overall, 86.5% of the patients had early-stage
disease (I, II) and 13.5% had advanced-stage disease. In addi-
tion, 40.4% had well-differentiated cancer (G1), 32.65% had
moderately differentiated cancer (G2), and 26.9% had poorly
differentiated cancer (G3). None of the patients had under-
gone radiation or chemotherapy before surgery. Treatment
consisted of total hysterectomy and a BSO alone (30.3%), or total hysterectomy and BSO and pelvic and/or para-aortic lymph node dissection (69.7%). No patients had remaining macroscopic tumors at the time of surgery.
2. CD8, CD4 infiltration into endometrial carcinoma tissues
CD8 and CD4 antigens were stained in endometrial carci- noma tissues. The distribution pattern of CD8+, CD4+ lym- phocytes was similar to that of lymphocytes as determined by conventional H&E staining. Lymphocytic infiltration of CD8+, CD4+ was observed more frequently in the stroma surrounding tumors than within the tumors. The patients were divided into 2 groups based on the median CD8+ or CD4+
cell counts. The positive/high cell count group consisted of patients with ≥40 stromal CD8+ or CD4+ T-lymphocytes in a microscopic field at ×200 [6,7]. The number of stromal CD8+
cells in positive group (range, 42–70; median, 50.3) was significantly higher (P<0.01) than in negative group (range, 14–32; median, 26.3) and the number of stromal CD4+
cells in positive group (range, 44–82; median, 53.0) was also significantly higher (P<0.01) than in negative group (range, 15–34; median, 24.7). The proportions of CD8+ and CD4+
lymphocytes in the endometrial adenocarcinoma were 67.4%
Table 1. Clinicopathological characteristics of the patients with endometrial carcinoma
Variable No. of patients (%)
Age (yr)
≤60 57 (64.0)
>60 32 (36.0)
Menopause
Pre- 12 (13.5)
Post- 77 (86.5)
Body mass index (kg/cm
2)
≤25 27 (30.3)
>25 62 (69.7)
FIGO grade
G1 36 (40.0)
G2 29 (32.6)
G3 24 (27.4)
FIGO stage
I 64 (71.9)
II 13 (14.6)
III 10 (11.2)
IV 2 (2.3)
FIGO, International Federation of Gynecology and Obstetrics.
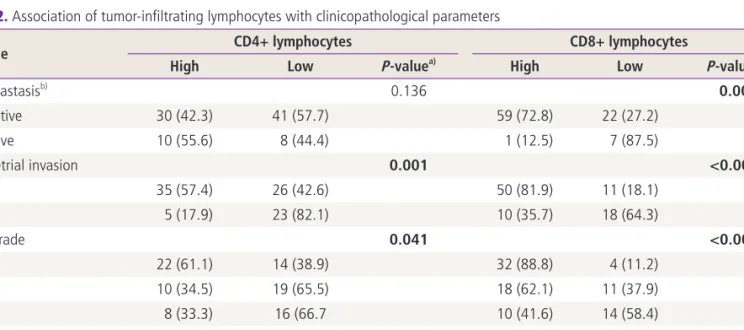
Table 2. Association of tumor-infiltrating lymphocytes with clinicopathological parameters
Variable CD4+ lymphocytes CD8+ lymphocytes
High Low P-value
a)High Low P-value
a)LN metastasis
b)0.136 0.002
c)Negative 30 (42.3) 41 (57.7) 59 (72.8) 22 (27.2)
Positive 10 (55.6) 8 (44.4) 1 (12.5) 7 (87.5)
Myometrial invasion 0.001 <0.001
<1/2 35 (57.4) 26 (42.6) 50 (81.9) 11 (18.1)
>1/2 5 (17.9) 23 (82.1) 10 (35.7) 18 (64.3)
FIGO grade 0.041 <0.001
G1 22 (61.1) 14 (38.9) 32 (88.8) 4 (11.2)
G2 10 (34.5) 19 (65.5) 18 (62.1) 11 (37.9)
G3 8 (33.3) 16 (66.7 10 (41.6) 14 (58.4)
FIGO stage 0.311 0.052
c)I–II 36 (46.8) 41 (53.2) 55 (71.4) 22 (28.6)
III–IV 4 (33.3) 8 (66.7) 5 (41.6) 7 (58.4)
Values are presented as number (%).
LN, lymph node; FIGO, International Federation of Gynecology and Obstetrics.
a)