237
미치는 영향
The Effect of Periurethral Prostatic Calculi on Lower Urinary Tract Symptoms in Benign Prostatic
Hyperplasia
Woo Heon Cha, Ki Ho Kim, Young Jin Seo
From the Department of Urology, College of Medicine, Dongguk University, Gyeongju, Korea
Purpose: The aim of this study was to evaluate the effect of periurethral prostatic calculi on lower urinary tract symptoms (LUTS) at the initial visit and after treatment with an alpha-blocker in benign prostatic hyperplasia (BPH).
Materials and Methods: A total of 223 male patients with LUTS were studied. Group 1 consisted of 81 patients with periurethral prostatic calculi within 5mm from the prostatic urethra of the transitional zone, as deter- mined by transrectal ultrasound. Group 2 consisted of 142 patients without periurethral prostatic calculi within 5mm from the prostatic urethra. The International Prostate Symptom Score (IPSS), maximal urinary flow rate (Qmax) and post voided residual urine (PVR) were measured in patients of both groups at the beginning of the study and at eight weeks after the treatment with 4mg doxazosin gastrointestinal therapeutic system (GITS).
Results: Voiding, storage and the total IPSS for Group 1 patients were higher than for Group 2 patients (p<0.05). Quality of life (QoL), Qmax, and PVR were not significantly different at the initial visit. After treatment with 4mg doxazosin GITS, an improvement of voiding, storage and the total IPSS for Group 2 patients was seen as compared to Group 1 patients (p<0.05). The mean improvement of QoL was 0.44±0.73 for group 1 pa- tients and 1.13±0.82 for group 2 patients (p<0.001). The mean change of Qmax was 1.02±1.40ml/sec for Group 1 patients and 1.52±1.84ml/sec for Group 2 patients (p=0.035). Changes of PVR were not significant between the two groups.
Conclusions: This study suggests that the periurethral prostatic calculi may aggravate lower urinary tract symptoms and decrease the effect of alpha- blockers. (Korean J Urol 2008;49:237-241)
Key Words: Calculi, Symptoms, Prostatic hyperplasia
대한비뇨기과학회지 제 49 권 제 3 호 2008
동국대학교 의과대학 비뇨기과학교실
차우헌ㆍ김기호ㆍ서영진
접수일자:2007년 11월 30일 채택일자:2008년 2월 12일
교신저자: 서영진
동국대학교 의과대학 경주병원 비뇨기과
경북 경주시 석장동 1090-1번지
780-350
TEL: 054-770-8265 FAX: 054-771-0769 E-mail: [email protected]
서 론
전립선비대증은 50세 이상 남성 환자들에서 흔한 질환이 며 하부요로증상으로 인해 고통을 야기하고 삶의 질에 악 영향을 끼친다. 사회의 고령화, 의료기술의 진보와 진단기 술의 향상으로 많은 환자들이 의료서비스를 이용하고 있으
며 언론매체의 홍보로 전립선비대증에 대한 관심이 증가하 고 있다.
우리나라의 정확한 통계는 밝혀져 있지 않으나 Chung 등1 은 전국 50대 이상의 남성 환자에서 전립선비대증의 유병 률을 44.7%로 추정하였고 임상적으로 의미 있는 전립선비 대증 환자들도 50세 이상 남성의 11.1%라고 하였다. 이런 높은 유병률을 보이는 전립선비대증에서 경직장전립선초
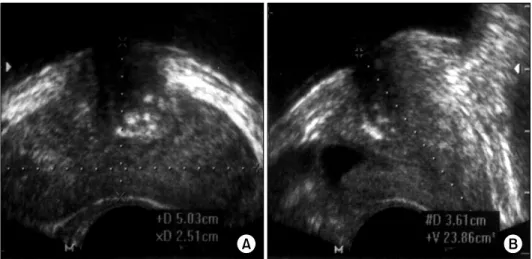
Fig. 1. Periurethral prostatic calculi within 5mm from the prostatic ure- thra of the transitional zone were detected on transrectal ultrasono- graphy (TRUS) findings, including more echogenic foci that caused acoustic shadowing as seen on a transverse view (A) and sagittal view (B) in Group 1 patients.
음파 검사는 직장수지검사에 비해 객관적인 방법으로 전립 선을 검사하여 정확한 진단과 치료에 도움을 주고 있다.
전립선비대증 환자에서 전립선결석은 경직장전립선초음 파 검사에서 많이 발견되지만 그 의미에 대해서는 논란이 있다. 전립선비대증의 하부요로증상이 전립선과 방광경부 의 평활근 긴장에 의한 전립선요도의 기능적 폐쇄에 의해 유발될 수 있음에도 전립선요도 주위의 전립선결석이 배뇨 시 전립선요도의 이완에 미치는 영향 및 이로 인한 전립선 비대증 환자의 하부요로증상에 미치는 영향에 대해서는 잘 알려져 있지 않다.2,3 또한 전립선 내의 결석은 전립선 선의 염증을 유발할 수 있고 전립선의 염증은 하부요로증상을 악화시키는 것으로 알려져 있다.4,5
따라서 저자들은 전립선비대증 환자에서 요도주위 전립 선이행대 결석이 하부요로증상에 미치는 영향과 약물치료 반응에 미치는 영향을 알아보고자 하였다.
대상 및 방법 1. 대상
2006년 1월부터 2007년 4월까지 하부요로증상을 주소로 내원한 50세 이상 환자 중 경직장전립선초음파 검사 후 doxazosin gastrointestinal therapeutic system (GITS) 4mg을 투 여한 223례를 대상으로 하였다. 5알파환원효소 억제제를 사용한 환자는 대상에서 제외하였다. 전립선비대증의 진단 은 전립선 크기가 25ml 이상이고 최대요속이 15ml/sec 이하 면서 국제전립선증상점수가 8 이상으로 하였다. 경직장전 립선초음파 검사에서 전립선 횡단면이미지에서 결석의 내 측면이 전립선요도로부터 5mm이내에 존재할 때 1군, 결석 이 관찰되지 않거나 결석의 내측면이 5mm 밖에 존재할 때 2군으로 분류하였다. 요도주위 전립선이행대 결석의 기준
을 요도주위 5mm 이내 결석의 내측면이 있는 것으로 정한 것은 대부분의 전립선이행대 결석이 요도주위에서 발견되 었고 요도주위 5mm를 벗어난 결석은 10%였으며 참고문헌 을 검색하였으나 이에 대한 적절한 기준이 없어 저자들이 임의로 정하였다.
1군은 81례, 평균연령은 63.30±7.72세였고 2군은 142례, 61.46±7.83세였다. 전립선특이항원이 4ng/ml 이상이었던 26 례는 경직장생검을 통해 전립선암이 없음을 확인한 후 각 군에 포함시켰다.
2. 방법
경직장전립선초음파 검사는 단일술자에 의해 초음파기 계 SA8000 (메디슨, 서울, 한국)을 사용하여 7.0MHz 탐침자 로 시행되었다.
술자는 환자를 좌측 측와위 자세에서 회색조 초음파검사 를 시행하였다. 전립선의 부피는 Terris와 Stamey 방식6으로 측정하였다.
전립선결석의 크기는 경직장전립선초음파의 횡단면 이 미지에서 전립선결석의 좌우의 길이가 제일 긴 이미지의 앞-뒤 (H)와 좌-우 길이 (W)를 측정하였고 정중선의 시상면 이미지에서 근위부와 원위부 사이의 길이 (L)를 측정하여 π/6xHxWxL (ml)로 계산하였다 (Fig. 1). 내원당시와 8주간 의 doxazosin GITS 4mg을 투여 후 국제전립선증상점수, 최 대요속, 잔뇨량을 비교분석하였다.
3. 통계적 분석
각 군 간의 비교는 SPSS 13.0을 이용하였다. 연속변수의 비교에는 모수검정에 사용하는 Student's t-test를 사용하였 고 비연속변수에는 chi-square test를 사용하였으며, p값이 0.05 미만인 경우에 통계적으로 유의한 것으로 판정하였다
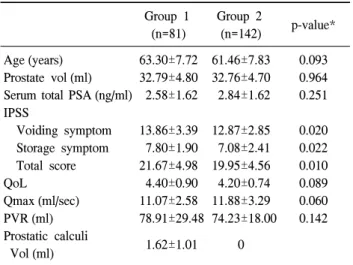
Table 1. Baseline patient characteristics Group 1
(n=81)
Group 2
(n=142) p-value*
Age (years) Prostate vol (ml) Serum total PSA (ng/ml) IPSS
Voiding symptom Storage symptom Total score QoL
Qmax (ml/sec) PVR (ml) Prostatic calculi Vol (ml)
63.30±7.72 32.79±4.80 2.58±1.62
13.86±3.39 7.80±1.90 21.67±4.98 4.40±0.90 11.07±2.58 78.91±29.48
1.62±1.01
61.46±7.83 32.76±4.70 2.84±1.62
12.87±2.85 7.08±2.41 19.95±4.56 4.20±0.74 11.88±3.29 74.23±18.00
0
0.093 0.964 0.251
0.020 0.022 0.010 0.089 0.060 0.142
PSA: prostate-specific antigen, IPSS: International Prostate Symp- tom Score, QoL: quality of life, Qmax: maximal urinary flow rate, PVR: post voided residual urine. *Statistical significance was done by student's t-test.
Table 2. Changes of IPSS, QoL, Qmax, PVR after 8 weeks of treatment with doxazosin GITS
Group 1 Group 2 p-value
IPSS
Voiding symptom Storage symptom Total score IPSS improvement ≥4
<4 QoL
Qmax (ml/sec) PVR (ml)
2.67±1.67
1.31±0.88
3.98±2.03
59.3%
40.7%
0.44±0.73 1.02±1.40 19.36±20.30
3.33±1.99
1.73±1.38
5.06±2.49
73.9%
22.1%
1.13±0.82 1.52±1.84 21.06±17.57
0.012*
0.015*
0.001*
0.023†
<0.001*
0.035*
0.511*
IPSS: International Prostate Symptom Score, QoL: quality of life, Qmax: maximal urinary flow rate, PVR: post voided residual urine, GITS: gastrointestinal therapeutic system. *Statistical significance was done by student's t-test, †Statistical significance was done by chi-square test.
(SPSS, Chicago, USA).
결 과 1. 치료 전 환자의 특성들
전립선 크기는 1군 32.79±4.80, 2군 32.76±4.70ml였고 (p>0.05) 혈중전립선특이항원은 1군 2.58±1.62, 2군 2.84±
1.62ng/ml였다 (p>0.05). 국제전립선증상점수 중 배뇨증상 점수는 1군 13.86±3.39, 2군 12.87±2.85였고 (p=0.020) 저장 증상점수는 1군 7.80±1.90, 2군 7.08±2.41이었으며 (p=0.022) 전체점수는 1군 21.67±4.98, 2군 19.95±4.56이었다 (p=0.010). 삶 의 질 점수는 1군 4.40±0.90으로 2군 4.20±0.74보다 높았으 나 통계적으로 유의하지 않았다 (p=0.089). 요류검사에서 최 대요속은 1군과 2군에서 각각 11.07±2.58과 11.88±3.29ml/
sec였고 (p=0.060) 잔뇨량은 1군과 2군에서 각각 78.91±29.48, 74.23±18.00ml였다 (p=0.142). 1군에서 요도주위 전립선이행 대 결석의 평균크기는 1.62±1.01ml였다 (Table 1).
2. Doxazosin GITS 투여 후 국제전립선증상점수, 최대 요속, 잔뇨량의 변화
8주간의 doxazosin GITS 4mg을 투여 후 1군과 2군에서 국제전립선증상점수, 최대요속, 잔뇨량을 측정하였다. 국제 전립선증상점수 중 배뇨증상점수는 1군 2.67±1.67, 2군 3.33±1.99가 감소하였고 (p=0.012) 저장증상점수는 1군 1.31±
0.88, 2군 1.73±1.38이 감소하였다 (p=0.015). 전체점수는 1 군과 2군에서 각각 3.98±2.03과 5.06±2.49가 감소되었고
(p=0.001) 4점 이상 전립선증상점수의 호전은 1군 59.3%
(48/81), 2군 73.9% (105/142)였다 (p=0.023). 삶의 질 점수는 1군 0.44±0.73, 2군 1.13±0.82가 호전되었다 (p<0.001). 최대 요속은 1군과 2군에서 각각 1.02±1.40, 1.52±1.84ml/sec가 증 가하였고 (p=0.035) 잔뇨량은 1군과 2군에서 19.36±20.30, 21.06±17.57ml가 감소하였으나 통계적으로 유의한 차이는 없었다 (p>0.05) (Table 2). 또한 단순히 요도주위 전립선결 석의 유무에 따라 비교하였을 때 국제전립선증상점수와 최 대요속은 1군과 2군의 차이와 비슷한 결과를 보였으나 통 계적인 유의성이 감소하였다.
고 찰
전립선비대증 환자에서 하부요로증상은 전립선 선종의 비대로 인한 전립선요도의 기계적인 폐색과 알파수용체의 교감신경계 자극에 의한 평활근 긴장의 역동학적 요소들에 의해 나타난다.7-11
전립선결석은 경직장전립선초음파 검사에서 우연히 발 견되는 경우가 많다. 전립선비대증의 유병률과 비슷하게 전립선결석은 노령화가 될수록 유병률이 증가하고 특히 40 대 이후에 급격히 증가한다. 하지만 전립선비대증 환자에 서 전립선결석의 유병률은 정확히 알려져 있지 않다.12,13
정맥석 같이 임상적으로 중요하지 않게 생각되기도 하나 일부에서 전립선결석이 전립선의 염증, 감염, 관의 폐쇄 등 을 일으키는 원인으로 생각한다.14 본 연구에서는 요도주위 전립선결석이 있는 전립선비대증 환자에서 요도주위 전립
선결석이 없는 환자들보다 국제전립선증상점수 중 배뇨증 상, 저장증상, 전체점수가 모두 높은 것으로 나타났다 (p
<0.05). 삶의 질 점수와 최대요속은 통계적으로 유의하지 는 않지만 나쁜 것으로 나타나서 전립선비대증에서 요도주위 전립선결석이 하부요로증상을 악화시키는 것으로 보인다.
전립선결석의 발생기전도 정확하게 알려져 있지 않다.
Young15은 전립선비대증 환자에서 전립선결석이 전립선 피 막 내 폐쇄에 의해 형성된다고 하였고 Cristol과 Emmett7는 전립선암에서도 전립선비대증과 유사하게 기계적인 압박 에 의해 전립선결석이 발생한다고 하였다. Moore4와 Kirby 등8은 전립선 내의 요의 역류에 의해 만성전립선염이 발생 하며 전립선결석의 형성에 영향을 준다고 하였다.
전립선결석의 분류에 대해서 Fox16와 Vilches 등17은 전립 선의 포낭 속에 있는 핵산과 단백질의 구형체에서 만들어 지고 여러 가지 무기질이 풍부하게 함유되어 있으면서 크 기가 작은 것을 1형 전립선결석, 크기가 크고 다면체의 전 립선 선내에 존재하는 결석을 2형 전립선결석으로 분류하 였다. Peeling과 Griffiths18는 초음파에 의한 전립선결석의 반향성에 따라 크기가 작은 결석들이 산재되어 있으면서 주로 전립선 선과 전립선 포낭 속에 분포된 것을 A형, 크기 가 크고 전립선요도의 경계부위에 주로 위치하며 초음파검 사에서 A형보다 명확히 관찰되는 것을 B형 전립선결석으 로 분류하였다. Moore4는 전립선의 조직학적 변화를 기준 으로 전립선결석이 전립선 선포에 존재하면서 만성적인 염 증세포가 침윤되어 있는 것과 전립선결석이 전립선 관을 팽창시키면서 상피층이 파괴되고 전립선의 섬유화가 되는 것으로 분류하였다.
전립선비대증 환자에서 알파차단제는 기능적인 폐쇄에 의한 전립선 평활근의 긴장도를 낮춰 전립선요도에서의 요 류의 흐름을 원활하게 한다. 알파수용체 중 A1 수용체에서 선택적으로 작용하는 doxazosin은 전립선과 방광경부 및 요 도에 분포하는 A1 수용체에 장기간 영향을 준다.19,20 Lepor 등21은 8주간 doxazosin 8mg을 사용하였을 때 전체 전립선 증상점수는 평균 5가 감소하고 최대요속은 3ml/sec가 증가 한다고 하였고 (p<0.05) Rahardjo 등22은 6주간 doxazosin 2mg을 사용하였을 때 전체 전립선증상점수는 7.2 감소 (p=0.036), 최대요속은 0.7ml/sec 증가 (p=0.004), 잔뇨량은 21ml가 감소하였다고 하였다 (p>0.05). 저자들의 경우에도 8주간 GITS 4mg을 사용하였을 때 요도 주위 전립선결석이 없는 군에서 전체 전립선증상점수는 5.06 감소, 최대요속은 1.52ml/sec 증가, 잔뇨량은 21ml가 감소하였다. 그러나 요도 주위 전립선결석이 있는 군은 알파차단제의 사용 후 국제 전립선증상점수 중 배뇨증상점수, 저장증상점수, 전체증상 점수의 호전정도가 결석이 없는 군보다 모두 통계적으로
유의하게 감소하였다. 삶의 질 향상과 최대 요속 또한 통계 적으로 유의하게 호전 정도가 감소하였다. 잔뇨량은 통계 적으로 의미는 없으나 결석이 있는 군에서 좀 더 낮게 나타 났다. 이는 요도주위의 전립선결석이 전립선비대증 환자의 약물투여 후의 증상개선에 부정적인 영향을 준다는 것을 추론해 볼 수 있다.
Bedir 등23은 여러 가지의 커다란 전립선결석들이 전립선 요도로 돌출되어 요폐를 일으킬 수 있다고 보고하였으나 Fox16와 Vilches 등17이 분류한 1형 전립선결석을 말하는 것 이다. 저자들이 대상에 포함시킨 전립선요도 주위의 전립 선결석은 Fox16와 Vilches 등17의 2형 전립선결석에 해당한 다.
Moore4는 전립선결석이 있는 전립선비대증 조직에서 만 성염증 또는 섬유화가 존재한다고 하였다. Minnery와 Getzenberg24는 하부요로증상을 심하게 호소하는 전립선비 대증 환자의 전립선조직에서 만성염증이 많이 나타나고 알 파차단제의 효과에 악영향을 줄 수 있다고 하였다. Konig 등5은 전립선비대증에서 interleukin 4, 5, 7, 9 수용체가 염증 반응에 의한 하부요로증상을 악화시킨다고 하였으며 Steiner 등25은 interleukin 17이 interleukin 6과 8의 표현을 증 가시켜 전립선비대증 조직의 성장을 촉진한다고 하였다.
본 연구에서도 전립선요도주위 전립선결석이 있는 전립선 비대증 환자가 결석이 없었던 환자보다 하부요로증상이 심 하고 알파차단제의 치료효과도 낮은 것을 알 수 있었다. 이 는 전립선결석에 의한 전립선비대증에서의 만성염증이 여 러 가지 cytokine에 의해 전립선증상을 악화시킨다고 추론 해 볼 수 있고 추후 요도주위 전립선결석이 배뇨 시 전립선 요도의 이완에 미치는 영향과 전립선조직의 염증반응에 대 한 연구가 필요할 것으로 생각한다.
Minnery와 Getzenberg24는 ibuprofen과 같은 non-steroidal anti-inflammatory drugs (NSAIDs) 등이 알파차단제의 효과와 독립적으로 항염증작용과 세포고사작용을 가지고 있기 때 문에 전립선비대증 환자에서 알파차단제의 기대했던 효과 가 경감되었을 때 투여해 볼 수 있다고 하였다. 그러므로 심한 하부요로증상을 호소하는 전립선비대증 환자에서 전 립선요도 주위에 전립선결석이 존재할 때 알파차단제의 치 료효과가 기대치보다 낮은 경우 NSAIDs의 사용을 고려할 수 있을 것이다.
결 론
전립선비대증 환자의 요도주위 전립선이행대의 결석은 경직장전립선초음파 검사에서 흔하게 관찰되며 전립선비 대증의 하부요로증상을 악화시키는 원인이 될 수 있고 전
립선비대증의 알파차단제의 치료효과도 감소시키는 것으 로 생각한다.
REFERENCES
1. Chung TG, Chung JS, Lee MS, Ahn HJ. Prevalence of benign prostatic hyperplasia in Jeong-eup area: community-based study. Korean J Urol 1999;40:51-8
2. Lepor H. Role of alpha-adrenergic blockers in the treatment of benign prostatic hyperplasia. Prostate Suppl 1990;3:75-84 3. Caine M. Alpha-adrenergic blockers for the treatment of benign
prostatic hyperplasia. Urol Clin North Am 1990;17:641-9 4. Moore RA. Morphology of prostatic corpora amylacea and
calculi. Arch Pathol 1936;22:22-40
5. Konig JE, Senge T, Allhoff EP, Konig W. Analysis of the inflammatory network in benign prostate hyperplasia and prostate cancer. Prostate 2004;58:121-9
6. Terris MK, Stamey TA. Determination of prostate volume by transrectal ultrasound. J Urol 1991;145:984-7
7. Cristol DS, Emmett JL. Incident of coincidence prostatic calculi, prostatic hyperplasia and carcinoma of prostate gland.
JAMA 1944;124:646-7
8. Kirby RS, Lowe D, Bultitude MI, Shuttleworth KE. Intra- prostatic urinary reflux: an aetiological factor in abacterial prostatitis. Br J Urol 1982;54:729-31
9. Abrams P, Donovan JL, de la Rosette JJ, Schäfer W. Inter- national Continence Society “Benign Prostatic Hyperplasia”
Study: background, aims, and methodology. Neurourol Urodyn 1997;16:79-91
10. Shapiro E, Hartanto V, Lepor H. The response to alpha blockade in benign prostatic hyperplasia is related to the percent area density of prostate smooth muscle. Prostate 1992;21:297-307
11. Shapiro A, Mazouz B, Caine M. The alpha-adrenergic blocking effect of prazosin on the human prostate. Urol Res 1981;
9:17-20
12. Klimas R, Bennett B, Gardner WA Jr. Prostatic calculi: a review. Prostate 1985;7:91-6
13. Sondergaard G, Vetner M, Christensen PO. Prostatic calculi.
Acta Pathol Microbiol Immunol Scand 1987;95:141-5 14. Shoskes DA, Lee CT, Murphy D, Kefer J, Wood HM.
Incidence and significance of prostatic stones in men with chronic prostatitis/chronic pelvic pain syndrome. Urology 2007;70:235-8
15. Young HD. Prostatic calculi. J Urol 1934;32:660-709 16. Fox M. The natural history and significance of stone formation
in the prostate gland. J Urol 1963;89:716-27
17. Vilches J, Lopez A, De Palacio L, Muñoz C, Gomez J. SEM and X-ray microanalysis of human prostatic calculi. J Urol 1982;127:371-3
18. Peeling WB, Griffiths GJ. Imaging of the prostate by ultrasound. J Urol 1984;132:217-24
19. Schwinn DA, Michelotti GA. Alpha 1-adrenergic receptors in the lower urinary tract and vascular bed: potential role for the alpha1d subtype in filling symptoms and effects of ageing on vascular expression. BJU Int 2000;85(Suppl 2):6-11 20. Elliott HL, Meredith PA, Reid JL. Pharmacokinetic overview
of doxazosin. Am J Cardiol 1987;59:78G-81
21. Lepor H, Kaplan SA, Klimberg I, Mobley DF, Fawzy A, Gaffney M, et al. Doxazosin for benign prostatic hyperplasia:
long-term efficacy and safety in hypertensive and normoten- sive patients. The Multicenter Study Group. J Urol 1997;
157:525-30
22. Rahardjo D, Soebadi DM, Sugandi S, Birowo P, Djati W, Wahyudi I. Efficacy and safety of tamsulosin hydrochloride compared to doxazosin in the treatment of Indonesian patients with lower urinary tract symptoms due to benign prostatic hyperplasia. Int J Urol 2006;13:1405-9
23. Bedir S, Kilciler M, Akay O, Erdemir F, Avci A, Ozgök Y.
Endoscopic treatment of multiple prostatic calculi causing urinary retention. Int J Urol 2005;12:693-5
24. Minnery CH, Getzenberg RH. Benign prostatic hyperplasia cell line viability and modulation of jm-27 by doxazosin and ibuprofen. J Urol 2005;174:375-9
25. Steiner GE, Newman ME, Paikl D, Stix U, Memaran-Dagda N, Lee C, et al. Expression and function of pro-inflammatory interleukin IL-17 and IL-17 receptor in normal, benign hyperplastic, and malignant prostate. Prostate 2003;56:171-82