약물역학위해관리학회지 2013;6:33-36 □ REVIEW □
접수: 2013년 3월 5일, 승인: 2013년 4월 8일 연락처: 배종면, 690-756, 제주시 제주대학로 102
제주대학교 의학전문대학원 예방의학교실 Tel: (064) 764-3856, Fax: (064) 725-2593 E-mail: jmbae@jejunu.ac.kr
Correspondence to: Jong-Myon Bae, MD, PhD
Department of Preventive Medicine, Jeju National University School of Medicine, 102 Jejudaehakno, Jeju 690-756, Korea Tel: +82-64-764-3856, Fax: +82-64-725-2593
E-mail: jmbae@jejunu.ac.kr
환자군 코호트 연구의 개념과 특징
제주대학교 의학전문대학원 예방의학교실
배 종 면
The Concept and Characteristics of Patients Cohort Study Jong-Myon Bae, MD, PhD
Department of Preventive Medicine, Jeju National University School of Medicine, Jeju, Korea
According to activation of clinical epidemiologic studies using secondary data sources, the word of patients cohort study (PCS) is emerging. Because of sharing the concept of cohort, PCS may be confused with the traditional cohort study (TCS). In addition, PCS may be mixed up with disease registry (DS) in point of patients’
enrolment. To corroborate the concept and characteristics of patients cohort study, author tried to summarize the differences among PCS, TCS, and DS. The PCS obviously differentiates from TCS and DS in items of the con- structing aim, entry criteria, information of exposure, statistics of outcome, targeting factors, and confounding control. To derive a correct result from secondary data sources, the concept and characteristics of PCS should be understood exactly. (JPERM 2013;6:33-36)
Key Words: Cohort studies; Patient selection; Registries; Pharmacoepidemiology
서 론
제 3상 무작위배정 임상시험(randomized clinical trial, 이 후 RCT)을 통해 효능(efficacy)을 확인한 약물이라 할지라도, RCT의 연구 설계상 한계점들 때문에 시판 후에 실제 진료 상황에서 다양한 환자의 복용에 따른 효과(effectiveness)와 안전(safety)을 확인할 필요성이 부각되고 있다.1) 이런 목적 을 위해 의료보험 수진 청구자료 같은 이차 자료원(secon- dary data source)의 활용을 통한 연구가 활발해 지면서,2,3)
‘환자군 코호트 연구’(patients cohort study, 이후 PCS)라는 용어가 제시되고 있다.4,5)
PCS는 코호트란 뜻 때문에 건강인을 대상으로 하는 기존 의 전통 코호트 연구(traditional cohort study, 이후 TCS)와 혼 동될 뿐만 아니라,6) 환자를 대상으로 한다는 점에서 질병통
계산출을 목적으로 하는 질병등록(disease registry, 이후 DR) 와 혼동할 가능성이 높다.7) 이에 본 논문은 PCS가 TCS 및 DR과의 차이점을 각각 살펴보면서 PCS에 대한 고유한 특 성을 정리하고자 한다.
환자군 코호트 개념 정리
현재까지 역학에서 ‘환자군 코호트(patients cohort)’란 용 어를 정의하는 발표 자료를 찾기는 아직 어렵다. 단지 코호 트(cohort)라는 용어는 ‘동일한 속성을 가진 집단’을 뜻한다 는 점에서, ‘환자군 코호트’란 ‘특정 질병으로 진단받은 환 자 집단’이란 의미를 갖기 위해 만든 복합어로 유추할 수 있다. 실제로 Glader 등4)이 수행한 연구의 대상을 살펴보면, 관상동맥질환을 의심받아 혈관조영술을 시행한 환자를 전
34 약물역학위해관리학회지 제6권 제1호, 2013
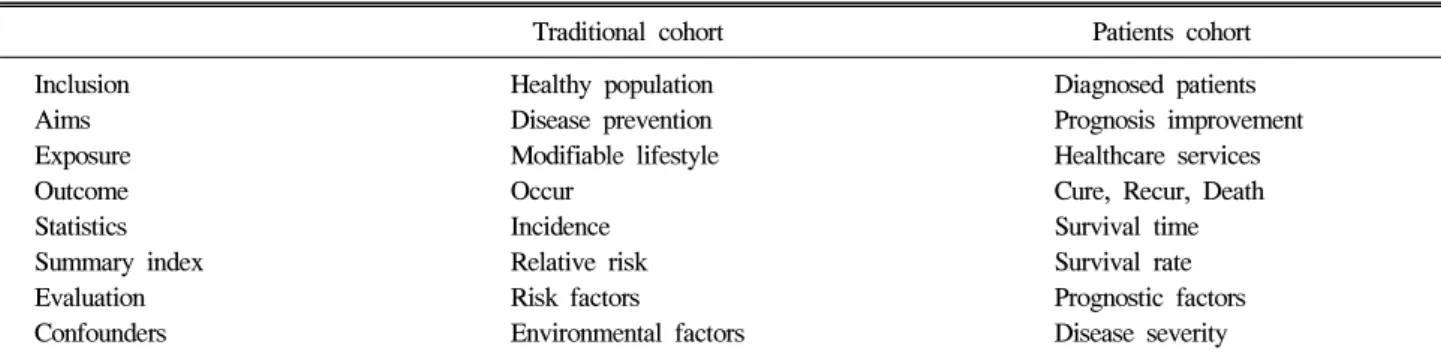
Table 1. Summary of differences between traditional cohort study and patients cohort study
Traditional cohort Patients cohort Inclusion Healthy population Diagnosed patients Aims Disease prevention Prognosis improvement Exposure Modifiable lifestyle Healthcare services
Outcome Occur Cure, Recur, Death
Statistics Incidence Survival time
Summary index Relative risk Survival rate
Evaluation Risk factors Prognostic factors
Confounders Environmental factors Disease severity 향적으로 모은 뒤, 예후 인자 규명을 위하여 추적 관찰을 한
것이었다.
따라서 PCS란 특정 질환에 관련하여 진단, 치료, 예방의 술 등을 받은 환자를 대상으로 코호트를 구성한 다음, 예후 인자 규명 등을 위해 추적 관찰을 하는 연구라고 정의할 수 있겠다. 연구 설계상 대상자 선정 시점에 따라 전향적(pro- spective) 및 후향적(retrospective) PCS로 대분할 수 있을 것 이다.8,9)
건강인 코호트 연구(TCS)와의 차이점
공통 속성을 갖는 대상자를 모아서 추적조사를 한다는 점에서 PCS와 TCS는 혼동될 수 있다. 그러나 두 연구 설계 간의 차이는 표 1와 같이 정리할 수 있다.
PCS가 TCS와 가장 두드러지게 차이나는 항목은 대상자 선정 기준이다. PCS는 특정 질병의 진단 기준(diagnostic criteria)에 맞는 환자를 연구대상자로 모집한다면, TCS는 특 정 질병의 발생 위험을 가진 건강인을 대상으로 구축한다는 점에서 가장 큰 차이점을 갖는다. TCS는 대상자 입적 시 특 정 질병이 없다는 점과 향후 질병이 일어날 수 있다는 점을 고려하여 대상자를 선정한다.2,10) 예를 들어 자궁경부암 발 생 위험요인을 규명하는 TCS에서는 대상자가 자궁경부암 유병환자가 아니어야 하고, 만약 자궁을 이미 절제했다면 이 또한 제외해야 하며, 추적관찰 도중 자궁절제술을 받았다면 그 시점까지 추적관찰을 완료하는 것이다. 그러나 PCS는 자 궁경부암의 진단기준에 맞는 환자로서 연구 관심을 가진 의 료서비스를 받는 경우에 연구대상자가 될 것이며, 재발이나 사망이 발생할 경우 추적관찰을 마감하게 된다.
두 번째 차이점은 폭로(exposure)에 대한 내용이다. TCS 는 질병예방(disease prvention)을 목적으로 조절 가능한 생활 습관(modifiable lifestyle) – 예를 들어 흡연, 음주, 운동, 식이 등-의 폭로여부를 코호트 구축 당시에 알아낸다. 반면 PCS 는 예후향상(prognosis improvement)을 목적으로 특정 질병 을 의심받아 행하게 될 의료서비스 – 예를 들어 진단, 약물,
수술, 기구 등 – 내용이 폭로 내용이 되는 것이다.
세 번째 차이점은 결과(outcome)에 관한 내용이다. TCS는 관심 질병의 발생 여부가 주요 결과 변수인 반면, PCS는 완 치(cure), 재발(recur), 사망(death) 여부를 알아보는 것이다.
네 번째 차이점은 제시하는 지표에 관한 내용이다. TCS 는 질병발생여부를 비교하기 위하여 발생률(incidence)을 산 출하며, 폭로여부에 따른 발생률 차이를 상대위험도(relative risk)로 제시한다. 반면 PCS는 생존기간(survival time)을 산 출하며, 의료서비스 수진 여부에 따른 생존기간의 차이를 생존률(survival rate)로 제시하는 것이다.
다섯 번째 차이점은 폭로-결과의 관련성을 통해 규명하 는 내용이다. TCS는 조절 가능한 생활습관 중 관심 질병의 발생 위험을 높이는 위험 요인(risk factors)을 확인한다. 반 면, PCS는 특정 의료서비스에 따른 생존 여부의 차이를 비 교하여 예후 요인(prognostic factors)을 규명하는 것이다. 또 한 비교효과연구를 적용하여 생존율 비교를 통해 특정 의료 서비스의 효과(effectiveness), 안전성(safety), 비용(cost)을 평 가하기도 한다.11)
마지막 차이점은 결론 도출을 위해 연령, 성별을 포함하 여 통제하는 교란변수의 내용에 관한 것이다. TCS는 관심 을 갖는 폭로와 질병에 모두 영향을 미칠 수 있으면서 코호 트 구축 당시 폭로 수준을 측정한 다양한 환경 요인들 통제 한다.9) 그러나 PCS는 암의 병기(stage)나 APGAR 점수 같이 해당 질병의 심각도를 통제한다. 또한 2차 자료원을 활용한 경우 측정하지 않은 잠재 변수들을 고려하여 성향점수(pro- pensity score)를 부여하거나, 도구변수(instrument variable)를 활용하여 의료서비스의 효과나 안전성을 비교 제시하고 있 다.2,12-14)
질병등록(DR)과의 차이점
특정 질병의 통계를 산출할 목적으로 운영되는 질병등록 사업(DR)은 첫 진단받은 환자를 등록한다는 점에서 PCS와 혼동될 수 있다.15) DR과 PCS간의 차이점은 표 2와 같이 정 리할 수 있다.
배종면. Patients Cohort Study 35
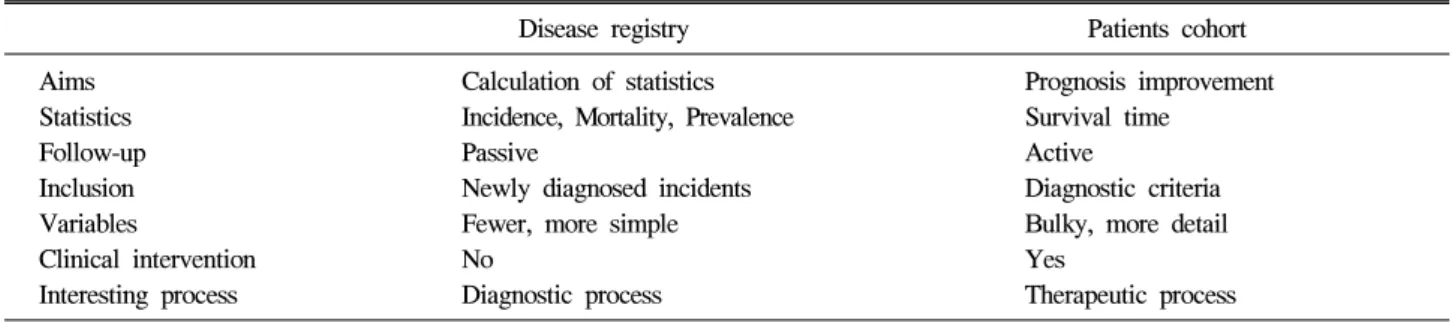
Table 2. Summary of differences between disease registry and patients cohort study
Disease registry Patients cohort Aims Calculation of statistics Prognosis improvement Statistics Incidence, Mortality, Prevalence Survival time
Follow-up Passive Active
Inclusion Newly diagnosed incidents Diagnostic criteria Variables Fewer, more simple Bulky, more detail
Clinical intervention No Yes
Interesting process Diagnostic process Therapeutic process
첫 번째 차이는 추진하는 목적에 있다. 표 1에서 언급한 대로 PCS는 환자의 예후를 향상시킬 방안을 강구하는 반면, DR은 특정 질병에 대한 통계치를 산출하여 제시하는 것이 다. 암등록(cancer registry)이 DR의 대표적인 사업으로 암과 관련한 통계치를 산출하는 것을 일차 목표로 하고 있다.7) 두 번째 차이는 수행 목적에 따른 산출 항목이다. DR의 목 적에 맞추어 특정 질병의 발생률을 우선적으로 산출하며, 사망률, 유병률, 생존률 등을 추가로 제시한다. 반면 PCS는 생존기간의 차이 여부를 우선적으로 살핀다. 이 과정에서 생존률과 사망률을 추가로 제시한다.
세 번째 차이는 산출을 목적으로 한 추적 조사의 방법이 다. PCS는 외래 및 입원 진료 등을 통해 생존 기간을 능동 적으로 알아본다. 반면, DR은 수동적인 방법을 우선적으로 적용하여 신환자 발생을 확인하며, 등록 자료의 질 향상을 목적으로 누락 대상을 찾아내기 위하여 능동적 추적조사를 추가로 수행하는 것이다.
네 번째 차이는 입적 대상자의 등록 기준이다. PCS는 표 1에서 언급한대로 해당 질병의 진단 기준에 맞으면서 관심 대상이 되는 의료서비스를 받은 환자를 연구 대상자로 선정 한다. 반면 DR은 질병 발생률 산출을 우선하기 위하여 반드 시 새로이 진단받은 신환을 등록 대상으로 삼는다.7) 예를 들어 DR에서는 유방촬영술 및 조직검사를 거쳐 새로이 진 단된 암환자만을 등록하며, 만약 해당자가 2년 전에 다른 의료기관에서 유방암 진단을 이미 받았다는 사실을 등록 후 알게 되었다면 이를 제외하고 발생률을 산출하는 것이다.
다섯 번째 차이는 수집하는 변수의 정도와 내용이다. DR은 발생률 산출에 필요한 변수들을 중심으로 수집하므로 확보 하는 변수가 상대적으로 적으면서 단순하다. 이는 질병 발 생자를 간과하는 경우를 줄이고 수집 자료의 질을 확보하는 것을 우선시하기 위함이다.7) 반면 PCS는 의료서비스의 효 과 및 안전성을 평가하기 위하여 생존율 차이에 영향을 미 치는 변수들을 최대한 수집하고자 한다. 따라서 DR에 비하 여 상대적으로 수집하는 변수 종류도 많고 내용도 더 자세 하다.
마지막 차이는 치료 개입(intervention) 여부와 관심영역이
다. PCS는 효과 및 안전성을 평가할 의료서비스를 대상자에 게 제공하고 치료 과정(therapeutic process)에 집중하는 반면, DR은 전혀 치료과정에 전혀 개입하지 않고 오직 관찰한 내 용만을 수집하며 해당 환자의 진단 과정(diagnostic process) 에 주된 관심을 둔다.
요약 및 제언
이상과 같이 PCS는 TCS와 DR과 분명히 차별되는 새로 운 연구방법이다. 다시 말해서 PCS는 TCS와 동일한 연구방 법으로 수행해서는 안된다는 것이다. 특히 적응증 오류 (confounder by indication)16)나 불멸 시간 오류(immortal time bias)17) 같이 PCS에서 특히 중요하게 다루어야 할 개념들이 있음을 감안할 때,2) PCS는 연구 설계부터 분석, 해석까지 기존의 TCS와는 전혀 새로운 연구방법으로 이해하고 접근 해야 할 것이다. 그렇게 할 때, 향후 약물역학 나아가 임상 역학연구를 제대로 수행하여 올바른 결과를 도출할 수 있는 바탕이 되기 때문이다.
참고문헌
1. The Korean Society of Preventive Medicine. Evidence-based clinical preventive service. Seoul: Kaechuk Publisher; 2011.
p. 25-35.
2. Korea Society for Pharmacoepidemiology and Risk Manage- ment. Pharmacoepidemiology. Seoul: Seoul National Universi- ty Press; 2011. p. 234-391.
3. Schneeweiss S, Avorn J. A review of uses of health care uti- lization databases for epidemiologic research on therapeutics.
J Clin Epidemiol 2005;58:323-37.
4. Glader CA, Birgander LS, Stenlund H, Dahlén GH. Is lip- oprotein(a) a predictor for survival in patients with establish- ed coronary artery disease? Results from a prospective patient cohort study in northern Sweden. J Intern Med 2002;252:
27-35.
5. Carabellese F, Candelli C, Martinelli D, La Tegola D,
36 약물역학위해관리학회지 제6권 제1호, 2013
Catanesi R. Cannabis use and violent behaviour: a psychiatric patients cohort study in Southern Italy. Riv Psichiatr 2013;48:
43-50.
6. Szklo M, Nieto FJ. Epidemiology. Beyond the basics, 2nd ed. Sudbury: Jones & Bartlette Publishers; 2007. p. 19-23.
7. Jensen OM, Parkin DM, MacLennan R, Muir CS, Skeet RG.
Cancer registration: principles and methods. Lyon: Internatio- nal Agency for Research on Cancer; 1991. p. 7-63.
8. Euser AM, Zoccali C, Jager KJ, Dekker FW. Cohort studies:
prospective versus retrospective. Nephron Clin Pract 2009;
113:c214-7.
9. Yu IT, Tse SL. Workshop 5. Sources of bias in cohort studies. Hong Kong Med J 2012;18:137-8.
10. Grimes DA, Schulz KF. Clinical research in obstetrics and gynecology: a Baedeker for busy clinicians. Obstet Gynecol Surv 2002;57(9 Suppl 3):S35-53.
11. Park BJ. Evidence-based healthcare. Seoul: Korea Publisher;
2009. p. 20-34.
12. Glynn RJ, Schneeweiss S, Stürmer T. Indications for propen- sity scores and review of their use in pharmacoepidemiology.
Basic Clin Pharmacol Toxicol 2006;98:253-9.
13. Greenland S. An introduction to instrumental variables for ep-
idemiologists. Int J Epidemiol 2000;29:722-9.
14. Schneeweiss S. Sensitivity analysis and external adjustment for unmeasured confounders in epidemiologic database studies of therapeutics. Pharmacoepidemiol Drug Saf 2006;15:291- 303.
15. Furuichi K, Shimizu M, Toyama T, Koya D, Koshino Y, Abe H, Mori K, Satoh H, Imanishi M, Iwano M, Yamauchi H, Kusano E, Fujimoto S, Suzuki Y, Okuda S, Kitagawa K, Iwata Y, Kaneko S, Nishi S, Yokoyama H, Ueda Y, Haneda M, Makino H, Wada T; Research Group of Diabetic Nep- hropathy, Ministry of Health, Labour, and Welfare of Japan.
Japan Diabetic Nephropathy Cohort Study: study design, methods, and implementation. Clin Exp Nephrol 2013 Feb 28. [PMID 23446518].
16. Farrington CP, Firth MJ, Moulton LH, Ravn H, Andersen PK, Evans S; Working Group on Non-specific Effects of Vaccines. Epidemiological studies of the non-specific effects of vaccines: II--methodological issues in the design and anal- ysis of cohort studies. Trop Med Int Health 2009;14:977-85.
17. Suissa S. Inhaled steroids and mortality in COPD: bias from unaccounted immortal time. Eur Respir J 2004;23:391-5.