원 저
전자매체(스마트폰)를 이용한 치과임플란트환자의 구강위생 관리
양현우
1
, 김진2
, 최한마음1
, 방일흠1
, 김소영1
, 이천의1†
1연세대학교 원주세브란스기독병원 구강악안면외과, 2가톨릭대학교 대전성모병원 구강악안면외과
Oral hygiene management of patients with dental implants using electronic media (Smartphone)
Hyun Woo Yang 1 , Jin Kim 2 , Hanmaeum Choi 1 , Yiqin Fang 1 , So Young Kim 1 , Chunui Lee 1†
1
Department of Oral and Maxillofacial Surgery, Wonju Severance Christian Hospital, Yonsei University Wonju College of Medicine,
2Department of Oral and Maxillofacial Surgery, Daejeon St. Mary’s Hospital, The Catholic University of Korea
Abstract
Smartphone usage has become so common that it has reached 2 billion people in the last year. As a result of this, hospitals have started making use of smartphones at various medical sites and research services for patients. This study aimed to establish support for developing a long distance program for patients with implants who have difficulty visiting clinics or with busy modern lives, by using smartphones for oral hygiene management instruction. The data were collected for 12 weeks, from July 24 to October 21, 2015, for patients who agreed to participate in the study. Although the subjects found the process of transferring photos via smartphone to be cumbersome (75%), the satisfaction level of the oral hygiene management program was excellent for all participating patients, and they all wanted to continue with further management using this process. The results from the phone satisfaction survey showed that oral hygiene self-management after oral hygiene control training by smartphones was mostly equal to previous habits (87.5%) or had partially increased but had not decreased. The need for data on more varied age groups and the issues of protecting the security of personal information on smartphones require further study. However, our study confirmed the efficacy of using electronic media (smartphones) for oral hygiene management in patients with a dental implant due to their improvement of oral hygiene performance as evidenced by less bleeding from probing on post-program visit.
Key Words: Oral hygiene, Dental implant, Smartphone, Electronic media
ISSN 2288-2804, https://doi.org/10.22671/JKADA.2019.7.1.39Received: September 18, 2019 Revised: October 23, 2019 Accepted after revision: October 28, 2019
†
Correspondence to Chunui Lee
Department of Oral and Maxillofacial Surgery, Wonju Severance Christial Hospital, 162-33 Ilsan-ro, Wonju 26426, Korea
Tel: +82-33-741-1451, Fax: +82-33-741-1442, E-mail: [email protected]
I. Introduction
A dental implant is the most common treatment method for replacing missing teeth.
With the introduction of of osseointergration in 1983 by Brånemark et al(1983), replacing the missing teeth using implants has become an alternative, safe, and predictable treatment for the edentulous space.
One of the factors affecting the long-term success rate of implants is the sound peri- implant tissue(Figuero et al, 2014; Lee et al, 2017). For the long-term use of implants, the stability of peri-implant tissues should be protected from invading bacteria by a thorough management of dental plaque(Lindhe and Meyle, 2008; Brown et al, 2019; Cortellini et al, 2019).
To this end, systematic education is essential for proper management, and it is important to encourage patients through motivation to continuously recognize the importance of and practice self-management(Renvert and Quirynen, 2015). However, periodically following up on patients who live in remote areas or who have busy modern lives is difficult.
In recent years, due to the development of
smartphones and the explosive increase in the number of people who use them, their scope of use has become wider and more diverse in the medical field(Sharif and Alkadhimi, 2019).
With the hope that our research could provide fundamental evidence for the development of a digital oral hygiene program, our study was designed to investigate patient satisfaction and patient response to smartphone use as their oral hygiene management tool through plain statistical analyses.
II. Materials & Methods
Eight of the 45 people who qualified agreed to participate in our 12-week oral hygiene
Fig. 2. Image of videos with oral hygiene instructions.
Fig. 1. (A) Previous oral hygiene kit. (B) Improved oral hygiene kit.
program (July 24 to October 21, 2015). The kit of oral hygiene care materials was improved and distributed to patients who had implant surgeries (Fig. 1). The patients were educated with videos which included oral hygiene instructions (Fig.
2). Most importantly, dental hygienists from our clinic instructed the patient on how to use the smartphones. The patients were able to access oral hygiene instructions through their smartphones when they could not visit the clinic.
We subsequently analyzed the gender and age composition of all patients and participants of our program separately. We also conducted a simple demographic of patients and analyzed their general characteristics. At the end of our program, patients filled out questionnaires which were composed of two categories: 1) the reason for not participating in the program and
2) the degree of satisfaction after oral hygiene instructions via smartphone. One implant was selected from each patient, and patients’
oral hygiene was comparatively evaluated by checking for bleeding on probing (defined as 3 points on the buccal surface) during the first visit and the visit after the end of the program. The Wilcoxon signed rank test was also performed to compare the variables between these two visits.
III. Results
Patients who visited Wonju Severance Christian Hospital dental clinic for implant surgery were middle-aged, (Table 1) the majority of participants were female (75%), and 50%
lived in remote areas (Table 2). The participants responded that the smartphone oral hygiene
Table 1. General characteristics of overall patients Characteristics Categories n (%)
Gender Male 29 (64.4)
Female 16 (35.6)
Age (years) 20~30 6 (13.3)
40~50 25 (55.6)
Over 60 15 (33.3)
Sum 45 (100)
Table 2. General characteristics of participants Characteristics Categories n (%)
Gender Male 2 (25)
Female 6 (75)
Age (years) 20~30 4 (50)
40~50 3 (37.5)
Over 60 1 (12.5)
Habitation Local 2 (25)
Less than 1 hour 2 (25) More than 1 hour 4 (50)
Sum 8 (100)
Table 3. Degree of satisfaction
Characteristics Categories n (%)
Procedure Cumbersome 75
Tolerable 25
Degree of satisfaction
Satisfactory 100
Unsatisfactory 0
Desire for further management
Wanted 100
Unwanted 0
Improved sense of oral hygiene control
Unimproved 87.5
Improved 13.5
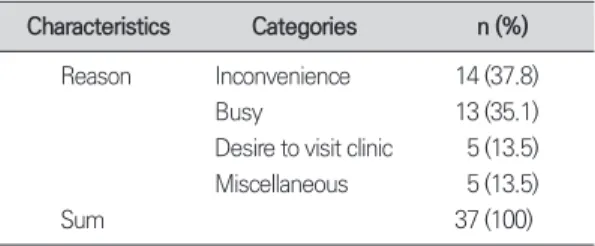
Table 4. Reasons for refusing to participate in the pro- gram
Characteristics Categories n (%)
Reason Inconvenience 14 (37.8)Busy 13 (35.1)
Desire to visit clinic 5 (13.5) Miscellaneous 5 (13.5)
Sum 37 (100)
tool use was rather cumbersome compared to oral instructions. However, all participants were completely satisfied after using their smartphones for the oral hygiene program and desired to continue this program afterwards. A post-research telephone survey revealed that some participants developed a better sense of and attention to oral hygiene care (13.5%) but most of the patients continued their previous degree of oral hygiene management (Table 3). The major reason that patients did not consent to participate in the program was the inconvenience of using the smartphone. Aside from this, some of them simply wanted to visit the clinic and some of them did not own smartphones (Table 4). Patients’ comparative analysis of bleeding on probing (BOP) on a selected implant revealed improved patient oral hygiene. The Wilcoxon signed rank test was performed between two subgroups: the first visit and the visit after the program at a significance level of 0.05. However, negative statistical significance was found between the two groups (Table 5).
IV. Discussion
There has been significant growth in the field of dental implants in the past few decades.
Various implants have surfaced which are designed for efficient osseointegration, and rapidly-developing prosthetic techniques have led patients to report dental implant therapy as irreplaceable(Smeets et al, 2016). Along with such support and an increasing number of patients, many studies have now identified that peri- implant diseases are inevitable without proper management(Tawse-Smith et al, 2002; Derks and Tomasi, 2015). Moreover, researchers have come to the consensus that a systematic and long-term oral-hygiene management protocol is obligatory for every patient who has an implant surgery and prosthesis. Through systematic programs, dental clinic staff must help patients to understand the importance of peri-implant self-maintenance.
However, those who live in remote areas or have busy lives have missed conventional oral hygiene maintenance programs due to their limited visits to the dental clinic. This study
Table 5. Comparative analysis of oral hygiene improvement via bleeding on probing (BOP)
First visit (n=24) Visit after the program (n=24)
1 + + + + - +
2 - - - - - -
3 - - + - - -
4 - - - - - -
5 + - - - - -
6 - + + + - -
7 - - - - - -
8 - - + - - +
Sum 8 sites of bleeding on probing 4 sites bleeding on probing
p-value 0.102
*p-value by Wilcoxon signed rank test.
provides optimistic evidence for a digital oral hygiene maintenance program with full patient satisfaction. Although the oral hygiene improvement outcome was not statistically verified due to factors such as low sample size, researchers could strongly confirm patients’
oral hygiene improvement from a clinical perspective. Additionally, authors recognized that patient satisfaction not only came from the context of the mobile management program, but also the periodic collection of patient responses via telephone. Furthermore, concern for elderly patients who are not familiar with smartphones is required. Visually simplified manuals and tools which can be more easily used by elderly patients must be designed in order to increase the positive outcome of a program like this one.
The risks associated with personal data being sent via smartphones must also be taken into consideration.
V. Conclusion
The oral hygiene management of dental implant patients in our study using electronic media (smartphones) resulted in patients’
satisfaction and an improvement of oral hygiene performance.
VI. References
Brånemark PI. Osseointegration and its experimental background. J Prosthet Dent 1983;50(3):399-410.
Brown JL, Johnston W, Delaney C, Short B, Butcher MC,
Young T, et al. Polymicrobial oral biofilm models:
simplifying the complex. J Med Microbiol 2019. doi:
10.1099/jmm.0.001063. [Epub ahead of print]
Cortellini S, Favril C, De Nutte M, Teughels W, Quirynen M.
Patient compliance as a risk factor for the outcome of implant treatment. Periodontol 2000 2019;81:209-25.
Derks J, Tomasi C. Peri-implant health and disease. A systematic review of current epidemiology. J Clin Peri- odontol 2015;42 Suppl 16:S158-71.
Figuero E, Graziani F, Sanz I, Herrera D, Sanz M. Man- agement of peri-implant mucositis and peri-implanti- tis. Periodontol 2000 2014;66(1):255-73.
Lee CT, Huang YW, Zhu L, Weltman R. Prevalences of peri-implantitis and peri-implant mucositis: systematic review and meta-analysis. J Dent 2017;62:1-12.
Lindhe J, Meyle J; Group D of European Workshop on Periodontology. Peri-implant diseases: consensus re- port of the Sixth European Workshop on Periodontol- ogy. J Clin Periodontol 2008;35(8 Suppl):282-5.
Renvert S, Quirynen M. Risk indicators for peri-implanti- tis. A narrative review. Clin Oral Implants Res 2015;26 Suppl 11:15-44.
Sharif MO, Alkadhimi A. Patient focused oral hygiene apps: an assessment of quality (using MARS) and knowledge content. Br Dent J 2019;227(5):383-6.
Smeets R, Stadlinger B, Schwarz F, Beck-Broichsitter B, Jung O, Precht C, et al. Impact of dental implant sur- face modifications on osseointegration. Biomed Res Int 2016;2016:6285620.
Tawse-Smith A, Duncan WJ, Payne AG, Thomson WM, Wennström JL. Relative effectiveness of powered and manual toothbrushes in elderly patients with implant- supported mandibular overdentures. J Clin Periodontol 2002;29(4):275-80.