서 론
유방암 환자에서 액와부 림프절 전이는 생존율에 영향을 주는 가장 중요한 예후인자로 알려져 있다.(1) 2003년도 American
Joint Committee on Cancer (AJCC) 6판 분류법에 의하면 액 와부 림프절 전이가 없는 경우, 1개에서 3개, 4개에서 9개, 10개 이상 전이된 경우를 각각 N0, N1, N2, N3로 분류하였다.(2) 전 이된 액와부 림프절의 절대적 개수는 유방암의 중요한 예후 인자 로서, 수술 후 어떠한 보조적 치료를 선택하느냐에 영향을 미친 다.(3-5)
수술 후 보조적 방사선 치료는 일반적으로 종양의 크기가 5 cm 를 초과하거나 전이된 액와부 림프절이 4개 이상일 경우에 권장 되고 있지만, 전이된 액와부 림프절이 1개에서 3개일 경우 수술
Purpose: The status of axillary lymph node (LN) metastasis
is the most important prognostic factor in breast cancer.
Postoperative regional nodal radiotherapy is recommended usually based on the number of metastatic LNs, which is associated with the total number of removed LNs during the axillary dissection. We evaluated the prognostic impact of the ratio of metastatic LNs to removed LNs on disease free survival and overall survival in breast cancer patients.
Methods: The medical records of 743 breast cancer patients
with metastatic axillary LNs and treated at Samsung Medical Center between 1994 and 2003 were retrospectively ana- lyzed. The ratio of metastatic/removed LNs as well as the other prognostic factors were analyzed.Results: Both disease-free survival and overall survival rates
were significantly worse in patients with a ratio of metastatic/
removed LNs greater than 20% compared to those patients with a ratio of less than 20% (p=0.028, p<0.001, respectively).
In patients with T1-2 and N1 breast cancer, the ratio of meta- static/removed LNs greater than 20% was significantly asso- ciated with poorer disease-free survival (p=0.027).
Conclusion: A ratio of metastatic/removed LNs greater than
20% in the axilla can be an adverse prognostic factor in breast cancer patients with axillary node metastasis. In T1-2 N1 breast cancer patients, adjuvant radiotherapy as well as more aggressive chemotherapy therapy may be indicated.Key Words : Breast cancer, Lymph node, Ratio, Survival 중심단어 : 유방암, 림프절, 비율, 생존율
The Impact of the Ratio of Positive Nodes to Removed Nodes on Recurrence and Overall Survival in Node Positive Breast Cancer Patients
Je-Yeon Kim, Hye-In Lim, Se-Kyung Lee, Jae-Hyuck Choi, Wan-Wook Kim, Jun-Ho Choe, Jung-Han Kim, Ji-Su Kim, Jeong-Eon Lee, Seok-Jin Nam, Jung-Hyun Yang
Department of Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea
Breast Cancer
O R I G I N A L A R T I C L E
김제연ㆍ임혜인ㆍ이세경ㆍ최재혁ㆍ김완욱ㆍ최준호ㆍ김정한ㆍ김지수ㆍ이정언ㆍ남석진ㆍ양정현 성균관대학교 의과대학 삼성서울병원 외과학교실
절제한 액와 림프절과 전이된 림프절의 비율이 액와부 전이 유방암 환자의 재발과 전체생존율에 미치는 영향
책임저자 : 양정현
135-710 서울시 강남구 일원동 50, 성균관대학교 의과대학 삼성서울병원 외과
Tel: 02-3410-3463, Fax: 02-3410-0929 E-mail : [email protected]
접수일 : 2008년 9월 5일 게재승인일 : 2008년 12월 2일
194
후 보조적 방사선 치료의 효과와 필요성에 대해서는 논란의 여지 가 있어 왔다.(6-9) 전이된 액와부 림프절이 1개에서 3개인 환자 (N1군)를 대상으로 한 여러 연구들에서, 전신적 항암치료는 하였 으나 수술 후 보조적 방사선 치료를 하지 않은 경우, 10년 국소 재 발률은 16%에서 30%까지로 다양하게 보고되었다.(10-14) 한편, 절제한 액와부 림프절의 개수에 따른 국소 재발률의 차이가 연구 되었는데, Katz 등(13)은 절제한 액와부 림프절 개수 10개 이상 을 기준으로 재발률이 의미 있게 차이가 난다고 보고하였고, van der Wal 등(15)은 14개 이상을 기준으로 사망률이 의미 있는 차 이를 보인다고 보고하였다. 이런 연구 결과들은 액와부 림프절의 전이가 있는 유방암 환자의 재발률과 사망률이 전이된 림프절의 개수뿐만 아니라 절제한 림프절의 개수까지 고려할 필요가 있다 는 것을 시사하고 있다. 이러한 배경을 통하여 절제된 액와부 림 프절의 절대적 개수만이 아닌 절제된 전체 림프절 중 전이된 액와 부 림프절의 비율이 중요하다는 주장이 나오게 되었다.
최근 몇 년 동안 절제된 전체 림프절 중 전이된 액와부 림프절 의 비율이 유방암 환자의 재발과 전체 생존과 관계된 의미 있는 예후 인자라는 보고들이 있었으므로,(15-19) 저자들은 절제된 액 와부 림프절 중 전이된 림프절의 비율이 유방암 환자의 무병생존 율과 전체생존율에 어떤 관계를 가지고 있는지 알아보았다. 그리 고, 방사선 치료 시행 여부에 대한 논란이 있는 종양의 크기가 5 cm 이하인 N1군에 대하여 수술 후 보조적 방사선 치료 결정에 영향을 미치는지에 대해 알아보고자 하였다.
방 법
1994년 10월부터 2003년 5월까지 성균관대학교 의과대학 삼 성서울병원에서 유방암으로 수술받은 2,400명 중 유방 부분절제 술과 액와부 림프절 곽청술을 시행 받은 환자 혹은 변형근치적 유 방절제술을 시행 받은 환자들 중에서 액와부 림프절 전이가 확인 된 743명의 환자를 대상으로 하였다. 평균 추적관찰 기간은 58 개월(2-129개월)이었고 환자들의 나이, 림프-혈관 침윤 유무, 조 직학적 등급, 에스트로겐 수용체 유무, 종양의 크기, 전이된 액와 부 림프절 개수, 절제된 액와부 림프절 개수, 절제된 액와부 림프 절에 대한 전이된 림프절의 비율을 후향적으로 조사하였다. 환자 들의 상기 인자들을 전체생존율과 무병생존율에 대해서 단변량 분석을 시행하였다. 절제된 액와부 림프절에 대한 전이된 림프절 의 비율을 10% 간격으로 총 여섯 개의 군으로 나누어서 이에 대 한 10년 무병생존율과 전체생존율을 얻어 통계적으로 의미 있는 비율을 구하였으며, 액와부 림프절 전이가 확인된 743명과 특히 그 중 종양의 크기가 5 cm 이하인 N1군 387명을 대상으로 림프- 혈관 침윤 유무, 조직학적 등급, 에스트로겐 수용체 유무, 종양의
크기, 절제된 액와부 림프절 개수, 절제된 액와부 림프절에 대한 전이된 림프절의 비율에 대해 전체생존율과 무병생존율에 대해 서 다변량 분석을 시행하였다.
결 과
1. 환자군
환자군에 대한 임상적 특성은 Table 1에 자세히 기술하였다.
환자들의 평균 연령은 46 (±10.3)세였다. 절제된 액와부 림프절 의 평균 개수는 20.3개였고, 전이된 림프절의 평균 개수는 5.8개 였다. 액와부 림프절 전이 환자들의 10년 전체생존율은 66.5%였 으며, 10년 무병생존율은 57.9%였다.
2. 단변량분석
환자들의 나이, 림프-혈관 침윤 유무, 조직학적 등급, 에스트로 Table 1. Characteristics of patients (n=743)
Characteristics No. of patients (%)
LN=lymph node.
Age
≤50 522 (70.2)
>50 221 (29.8)
Lymphovascuar invasion
No 482 (64.9)
Yes 261 (35.1)
Histologic grade
I 92 (12.4)
II 373 (50.2)
III 278 (37.4)
Estrogen receptor
Positive 528 (71.1)
Negative 215 (28.9)
Tumor stage
T1 247 (33.2)
T2 403 (54.2)
T3 93 (12.5)
N stage
N1 418 (56.3)
N2 195 (26.2)
N3 130 (17.5)
No. of dissected LN
≤20 390 (52.5)
>20 353 (47.5)
Ratio of metastatic/removed LNs
≤10% 240 (32.3)
≤20% 169 (22.7)
≤30% 93 (12.5)
≤40% 66 (8.9)
≤50% 42 (5.7)
>50% 133 (17.9)
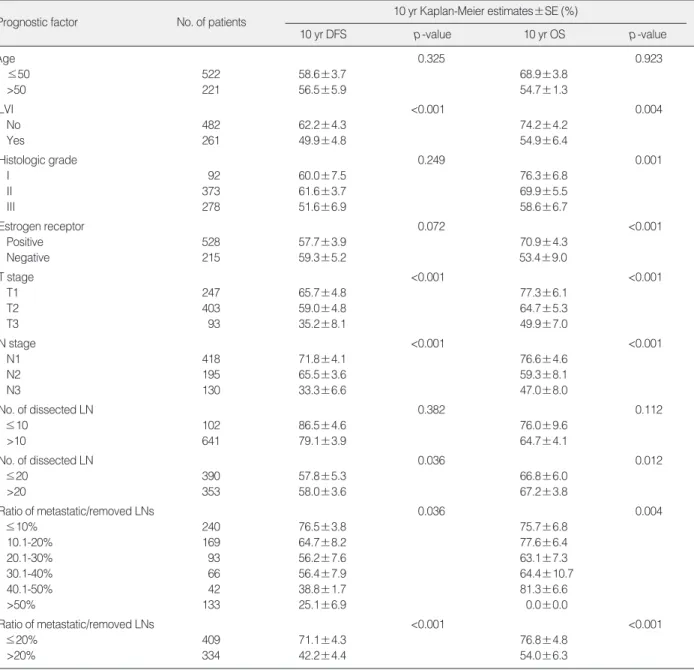
겐 수용체 유무, 종양의 크기, 절제된 액와부 림프절 개수, 절제 된 액와부 림프절에 대한 전이된 림프절의 비율을 전체생존율과 무병생존율에 대해서 단변량 분석을 시행하였다(Table 2). 환자 의 나이는 생존율과 상관이 없었다. 림프-혈관 침윤은 없는 경우 가 침윤이 있는 경우에 비해 전체생존율, 무병생존율 모두 더 높 았다(p<0.001, p=0.004). 조직학적 등급은 전체 생존율에 대해 서만 유의성을 보였다(p=0.001). 종양의 T 병기가 낮을수록 전체 생존율, 무병생존율 모두 유의하게 높았다(p<0.001, p<0.001).
액와부 림프절을 10개 이하로 절제한 경우를 10개 초과 절제한
경우와 비교하였을 때, 전체생존율과 무병생존율은 의미가 없었 으나, 20개를 기준으로 비교하였을 때에는 20개 초과 절제한 경 우가 전체생존율 및 무병생존율이 유의하게 높았다(p=0.036, p=0.012). 절제된 액와부 림프절에 대한 전이된 림프절의 비율 을 10% 간격으로 나누어 비교하였을 때 무병생존율에 대해서는 10%, 30%, 50%에서 의미가 없었으며(p=0.600, p=0.063, p<
0.054), 20%와 40%에서 의미가 있었고(p<0.001, p<0.001), 전체생존율을 비교하였을 때는 10%, 30%, 40%에서 의미가 없 었으며(p=0.496, p=0.104, p<0.061), 20%와 50%에서 의미
Table 2. Univariate analysis of DFS and OS by prognostic factors, for patients with axillary LN(+) (n=743)
Prognostic factor No. of patients 10 yr Kaplan-Meier estimates±SE (%)
10 yr DFS p-value 10 yr OS p-value
Age 0.325 0.923
≤50 522 58.6±3.7 68.9±3.8
>50 221 56.5±5.9 54.7±1.3
LVI <0.001 0.004
No 482 62.2±4.3 74.2±4.2
Yes 261 49.9±4.8 54.9±6.4
Histologic grade 0.249 0.001
I 92 60.0±7.5 76.3±6.8
II 373 61.6±3.7 69.9±5.5
III 278 51.6±6.9 58.6±6.7
Estrogen receptor 0.072 <0.001
Positive 528 57.7±3.9 70.9±4.3
Negative 215 59.3±5.2 53.4±9.0
T stage <0.001 <0.001
T1 247 65.7±4.8 77.3±6.1
T2 403 59.0±4.8 64.7±5.3
T3 93 35.2±8.1 49.9±7.0
N stage <0.001 <0.001
N1 418 71.8±4.1 76.6±4.6
N2 195 65.5±3.6 59.3±8.1
N3 130 33.3±6.6 47.0±8.0
No. of dissected LN 0.382 0.112
≤10 102 86.5±4.6 76.0±9.6
>10 641 79.1±3.9 64.7±4.1
No. of dissected LN 0.036 0.012
≤20 390 57.8±5.3 66.8±6.0
>20 353 58.0±3.6 67.2±3.8
Ratio of metastatic/removed LNs 0.036 0.004
≤10% 240 76.5±3.8 75.7±6.8
10.1-20% 169 64.7±8.2 77.6±6.4
20.1-30% 93 56.2±7.6 63.1±7.3
30.1-40% 66 56.4±7.9 64.4±10.7
40.1-50% 42 38.8±1.7 81.3±6.6
>50% 133 25.1±6.9 0.0±0.0
Ratio of metastatic/removed LNs <0.001 <0.001
≤20% 409 71.1±4.3 76.8±4.8
>20% 334 42.2±4.4 54.0±6.3
DFS=disease free survival; OS=overall survival; LN=lymph node; LVI=lymphovascular invasion.
가 있었다(p<0.001, p=0.001). 절제된 액와부 림프절 개수는 20% 초과인 경우 평균 21개, 20% 이하인 경우는 20개로 차이가 없었다.
3. 다변량분석
림프-혈관 침윤 유무, 조직학적 등급, 에스트로겐 수용체 유무, 종양의 크기, 절제된 액와부 림프절 개수, 절제된 액와부 림프절 에 대한 전이된 림프절의 비율에 대해 전체생존율과 무병생존율 에 대해서 다변량 분석을 시행하였다(Table 3). 림프-혈관 침윤 이 있는 경우, 무병생존율은 유의하게 낮았으나(p=0.031), 전체 생존율에는 별다른 영향을 주지 않았다. 조직학적 등급은 생존율 에 대해 통계학적 유의성을 보이지 않았다. 에스트로겐 수용체 유 무에 따른 생존율 차이를 보았을 때, 림프-혈관 침윤과는 달리 무 병생존율에 대해서는 차이가 없었고(p=0.687), 전체생존율은 에 스트로겐 수용체가 없는 경우가 더 낮았다(p=0.001). 종양의 크 기를 보았을 때, T1과 T2는 차이가 없었으나, T2에 비해 T3의 경우에는 무병생존율 및 전체생존율이 낮아 모두 의미 있는 차이
를 보였다(p=0.002, p=0.001). 전이된 액와부 림프절 개수에서 는 N병기가 올라갈수록 전체생존율은 차이가 없었으나, 무병생 존율은 의미있게 낮아졌다(p=0.005, p=0.035). 절제된 액와부 림프절에 대한 전이된 림프절의 비율을 보았을 때, 20% 이하인 경우가 20% 초과인 경우보다 무병생존율 및 전체생존율이 통계 학적으로 의미 있게 높았다(p<0.001, p<0.001).
종양 크기가 5 cm 이하인 N1군 387명을 대상으로 림프-혈관 침윤 유무, 조직학적 등급, 에스트로겐 수용체 유무, 종양의 크기, 절제된 액와부 림프절 개수, 절제된 액와부 림프절에 대한 전이된 림프절의 비율에 대해 전체생존율과 무병생존율에 대해서 다변 량 분석을 시행하였다(Table 4). 림프-혈관 침윤 유무, 조직학적 등급, 종양의 크기, 절제된 액와부 림프절 개수에 대해서는 무병 생존율, 전체생존율에 대해 모두 통계학적 차이가 없었다. 에스 트로겐 수용체가 있는 경우가 없는 경우에 비해 무병생존율은 유 의하게 높았으나(p=0.044), 전체생존율은 차이가 없었다. 절제 된 액와부 림프절에 대한 전이된 림프절의 비율을 보았을 때, 전 체생존율은 차이가 없었으나(p=0.173), 20% 이하인 경우가 20% 초과인 경우보다 무병생존율이 의미 있게 더 높았다(p=
0.027).
LVI
No 1.00 1.00 0.183
Yes 1.62 (1.04-2.52) 0.031 1.26 (0.89-1.76) Histologic grade
I 1.00 1.00
II 1.10 (0.72-1.69) 0.661 1.03 (0.52-1.67) 0.828 III 1.27 (0.60-2.69) 0.520 1.18 (0.66-2.10) 0.566 Estrogen receptor
Negative 1.00 1.00 0.001
Positive 0.94 (0.70-1.27) 0.687 2.03 (1.43-2.89) T stage
T1 1.00 1.00
T2 1.06 (0.76-1.46) 0.746 1.39 (0.89-2.15) 0.140 T3 1.91 (1.27-2.87) 0.002 2.45 (1.45-4.13) 0.001 N stage
N1 1.00 1.00
N2 1.67 (0.99-2.82) 0.005 1.66 (0.90-3.07) 0.108 N3 2.51 (1.33-4.74) 0.035 2.03 (0.95-4.31) 0.066 No. of dissected LN
≤20 1.00 1.00 0.163
>20 0.97 (0.65-1.58) 0.933 0.78 (0.56-1.10) Ratio of metastatic/removed LNs
≤20% 1.00 1.00
>20% 2.63 (1.96-3.53) <0.001 2.57 (1.77-3.72) <0.001 Table 3. Multivariate analysis of DFS and OS by prognostic factors, for patients with axillary LN(+) (n=743)
Prognostic factor
10 yr DFS Hazard ratio
(95% CI)
p- value
10 yr OS Hazard ratio
(95% CI) p- value
DFS=disease free survival; OS=overall survival; LN=lymph node; CI=
confidence interval; LVI=lymphovascular invasion.
LVI
No 1.00 1.00
Yes 1.08 (0.63-1.84) 0.774 1.26 (0.61-2.61) 0.527 Histologic grade
I 1.00 1.00
II 1.82 (0.76-4.32) 0.135 1.77 (0.52-5.97) 0.360 III 2.01 (0.81-5.01) 0.723 2.24 (0.64-7.80) 0.206 Estrogen receptor
Negative 1.00 1.00
Positive 0.55 (0.31-0.98) 0.044 0.84 (0.44-1.63) 0.612 T stage
T1 1.00 1.00
T2 1.05 (0.65-1.71) 0.721 1.12 (0.51-1.48) 0.564 No. of dissected LN
≤20 1.00 1.00
>20 0.81 (0.48-1.35) 0.419 0.79 (0.41-1.55) 0.494 Ratio of metastatic/removed LNs
≤20% 1.00 1.00
>20% 2.34 (1.10-4.98) 0.027 1.05 (0.68-1.76) 0.173 Table 4. Multivariate analysis of DFS and OS by prognostic factors, for patients with T1 or 2 and N1 stage (n=387)
Prognostic factor
10 yr DFS Hazard ratio
(95% CI) p- value
10 yr OS Hazard ratio
(95% CI) p- value
DFS=disease free survival; OS=overall survival; CI=confidence interval;
LVI=lymphovascular invasion; LN=lymph node.
고 찰
이번 연구에서는 림프절 전이가 있는 유방암 환자들을 대상으 로 절제된 액와부 림프절에 대한 전이된 림프절의 비율을 10% 간 격으로 총 여섯 개의 군으로 나누어서 각각의 림프절 전이군에 대 한 10년 무병생존율과 전체생존율을 얻어 절제된 액와부 림프절 에 대한 전이된 림프절의 비율 20%가 통계적으로 의미 있다는 것 을 확인하였으며, 다변량 분석을 하였을 때 20% 이하인 경우가 20% 초과인 경우보다 무병생존율 및 전체생존율이 통계학적으 로 의미 있게 높았다(Fig 1). 종양의 크기가 5 cm 이하인 N1군에 서는 전체생존율은 차이가 없었으나, 20% 이하인 경우가 20%
초과인 경우보다 무병생존율이 통계학적으로 의미 있게 더 높았 다(Fig 2).
현재 일반적으로 전이된 액와부 림프절 개수를 기준으로 4개 이상의 림프절에 전이가 있을 때 방사선 치료를 시행하지만, 최근
의 여러 연구들에서 절제된 림프절과 전이된 림프절의 비율도 전 이된 액와부 림프절 개수와 더불어 중요한 예후 인자 중 하나라고 알려지고 있다.(6-9) Katz 등(12)은 종양의 크기가 5 cm 이하인 N1군 1,031명의 환자를 다변량 분석한 결과, 10개 이하의 림프절 을 제거한 경우와 종양의 크기가 4 cm를 넘는 경우에서 의미 있게 재발이 많다고 보고하였고, 또 다른 연구를 통하여 종양의 크기가 5 cm 초과, 4개 이상의 전이된 액와부 림프절, 20% 초과의 전이 림프절 비율을 의미 있는 예후인자로 발표하였다.(13) Truong 등(18)은 N1군 542명을 대상으로 절제된 림프절과 전이된 림프 절의 비율에 따른 국소 재발, 원위부 재발과 전체생존율을 다변량 분석을 통해 분석하였는데, 절제된 림프절과 전이된 림프절의 비 율 25%를 예후 인자의 기준으로 삼고 비율이 25% 초과인 환자 는 수술 후 추가적 방사선 치료와 더욱 적극적인 전신적 치료가 필요하다고 주장하였다. Fortin 등(20)은 유방 부분절제술과 액 와부 림프절 곽청술을 시행받고 T1-T2의 액와부 림프절 전이가
Fig 1. Disease-free survival and overall survival by the ratio of metastatic/removed axillary lymph nodes with the cut-off value of 20% in the breast cancer patients with positive axillary lymph node(s) (n=743).
Disease free survival
1.0
0.8
0.6
0.4
0.2
0.0
0 20 40 60 80 100 120 140
Time (months)
p=0.028
>20%
≤20%
>20%
≤20%
A
Overall survival
1.0
0.8
0.6
0.4
0.2
0.0
0 20 40 60 80 100 120 140
Time (months)
p<0.001
B
Fig 2. Disease-free survival and overall survival by the ratio of metastatic/removed axillary lymph nodes with the cut-off value of 20% in the patients with T1-2 and N1 breast cancer (n=387).
Disease free survival
1.0
0.8
0.6
0.4
0.2
0.0
0 20 40 60 80 100 120 140
Time (months)
p=0.027
>20%
≤20%
A
Overall survival
1.0
0.8
0.6
0.4
0.2
0.0
0 20 40 60 80 100 120 140
Time (months)
p=0.173
B
>20%
≤20%
확인된 1,372명의 환자를 대상으로 전이 림프절이 1개에서 3개인 경우와 4개 이상인 경우 나누어 절제된 림프절과 전이된 림프절 의 비율을 조사하고 절제된 림프절과 전이된 림프절의 비율이 유 의한 예후 인자라고 보고하였는데, 액와부 전이 림프절이 1개에 서 3개인 경우는 절제된 림프절과 전이된 림프절의 비율이 40%
를 초과한 경우 재발이 높고, 4개 이상인 경우는 절제된 림프절과 전이된 림프절의 비율이 50%를 초과한 경우 재발이 높다고 하였 다. 여러 연구들에서 보고하는 절제된 림프절과 전이된 림프절의 비율의 기준이 다른 것은 아마도 환자군과 통계 방법의 차이가 원 인이라고 생각되나, 절제된 림프절과 전이된 림프절의 비율이 중 요한 예후 인자라는 주장에는 다름이 없다. 본 연구에서는 다변량 분석을 통하여 종양의 크기가 5 cm 초과인 경우와 전이된 림프절 의 비율이 20% 초과인 경우가 재발과 전체생존율에 좋지 않은 영 향을 미치는 것을 확인할 수 있었다.
Kuru 등(19)은 변형 근치적 유방절제술을 시행 받고 액와부 림 프절 전이가 확인된 801명의 유방암 환자를 조사하여, 절제된 림 프절과 전이된 림프절의 비율이 25% 초과되는 경우가 25% 이하 인 경우에 비해 유의하게 생존율이 낮다고 보고하였으며, 절제된 림프절의 개수가 15개 이상인 경우와 절제된 림프절 중 전이가 되 지 않은 림프절의 개수가 15개 이상인 경우는 생존율이 향상된다 고 발표하였으나, 수술 후 보조적 방사선 치료에 대한 결정에 논 란이 되는 종양의 크기가 5 cm 이하인 N1군에 대해서는 조사된 바 없었다. 이번 연구에서는 5 cm 이하인 N1군에 대해서도 절제 된 림프절과 전이된 림프절의 비율이 무병생존율에 영향을 주는 예후 인자임을 확인하였지만, 전체생존율에 대해서는 의미를 찾 지 못하였다. 하지만, 환자군의 수가 더 많아지고, 추적관찰 기간 이 더 길어진다면 전체생존율에서도 의미를 가질 수도 있지 않을 까 생각된다.
결 론
액와부 림프절 전이가 발견된 유방암 환자들에서 수술 후 액와 부 전이 림프절의 비율이 20% 초과인 경우가 20% 이하인 경우 보다 유의하게 좋지 않은 무병생존율을 나타낸다. 따라서, 절제 된 림프절과 전이된 림프절의 비율은 중요한 예후 인자이며, 종양 의 크기가 5 cm 이하인 N1군에서 절제된 림프절과 전이된 림프 절의 비율이 20% 초과라면 수술 후 보조적 방사선 치료를 고려할 필요가 있다고 사료된다.
참고문헌
1. Fitzgibbons PL, Page DL, Weaver D, Thor AD, Allred DC, Clark
GM, et al. Prognostic factors in breast cancer. College of American Pathologists Consensus Statement 1999. Arch Pathol Lab Med 2000;
124:966-78.
2. Singletary SE, Allred C, Ashley P, Bassett LW, Berry D, Bland KI, et al. Staging system for breast cancer: revisions for the 6th edition of the AJCC Cancer Staging Manual. Surg Clin North Am 2003;
83:803-19.
3. Atkinson EN, Brown BW, Montague ED. Tumor volume, nodal status, and metastasis in breast cancer in women. J Natl Cancer Inst 1986;76:171-8.
4. Carter CL, Allen C, Henson DE. Relation of tumor size, lymph node status, and survival in 24,740 breast cancer cases. Cancer 1989;63:
181-7.
5. Sauerbrei W, Royston P, Bojar H, Schmoor C, Schumacher M.
Modelling the effects of standard prognostic factors in node-positive breast cancer. German Breast Cancer Study Group (GBSG). Br J Cancer 1999;79:1752-60.
6. Recht A, Edge SB, Solin LJ, Robinson DS, Estabrook A, Fine RE, et al. Postmastectomy radiotherapy: clinical practice guidelines of the American Society of Clinical Oncology. J Clin Oncol 2001;19:
1539-69.
7. Recht A, Edge SB. Evidence-based indications for postmastectomy irradiation. Surg Clin North Am 2003;83:995-1013.
8. Truong PT, Olivotto IA, Whelan TJ, Levine M. Clinical practice guidelines for the care and treatment of breast cancer: 16. Locore- gional post-mastectomy radiotherapy. CMAJ 2004;170:1263-73.
9. Overgaard M, Nielsen HM, Overgaard J. Is the benefit of postma- stectomy irradiation limited to patients with four or more positive nodes, as recommended in international consensus reports? A sub- group analysis of the DBCG 82 b&c randomized trials. Radiother Oncol 2007;82:247-53.
10. Overgaard M, Jensen MB, Overgaard J, Hansen PS, Rose C, An- dersson M, et al. Postoperative radiotherapy in high-risk postmeno- pausal breast-cancer patients given adjuvant tamoxifen: Danish Breast Cancer Cooperative Group DBCG 82c randomised trial.
Lancet 1999;353:1641-8.
11. Ragaz J, Olivotto IA, Spinelli JJ, Phillips N, Jackson SM, Wilson KS, et al. Locoregional radiation therapy in patients with high-risk breast cancer receiving adjuvant chemotherapy: 20-year results of the British Columbia randomized trial. J Natl Cancer Inst 2005;97:
116-26.
12. Katz A, Strom EA, Buchholz TA, Thames HD, Smith CD, Jhingran
A, et al. Locoregional recurrence patterns after mastectomy and doxorubicin-based chemotherapy: implications for postoperative irradiation. J Clin Oncol 2000;18:2817-27.
13. Katz A, Buchholz TA, Thames H, Smith CD, McNeese MD, The- riault R, et al. Recursive partitioning analysis of locoregional recur- rence patterns following mastectomy: implications for adjuvant irra- diation. Int J Radiat Oncol Biol Phys 2001;50:397-403.
14. Wallgren A, Bonetti M, Gelber RD, Goldhirsch A, Castiglione-Ger- tsch M, Holmberg SB, et al. Risk factors for locoregional recurrence among breast cancer patients: results from International Breast Cancer Study Group Trials I through VII. J Clin Oncol 2003;21:1205-13.
15. van der Wal BC, Butzelaar RM, van der Meij S, Boermeester MA.
Axillary lymph node ratio and total number of removed lymph nodes:
predictors of survival in stage I and II breast cancer. Eur J Surg Oncol 2002;28:481-9.
16. Megale Costa LJ, Soares HP, Gaspar HA, Trujillo LG, Santi PX, Pereira RS, et al. Ratio between positive lymph nodes and total dis- sected axillaries lymph nodes as an independent prognostic factor
for disease-free survival in patients with breast cancer. Am J Clin Oncol 2004;27:304-6.
17. Vinh-Hung V, Verschraegen C, Promish DI, Cserni G, Van de Steene J, Tai P, et al. Ratios of involved nodes in early breast cancer. Breast Cancer Res 2004;6:R680-8.
18. Truong PT, Berthelet E, Lee J, Kader HA, Olivotto IA. The prognostic significance of the percentage of positive/dissected axillary lymph nodes in breast cancer recurrence and survival in patients with one to three positive axillary lymph nodes. Cancer 2005;103:2006-14.
19. Kuru B. Prognostic significance of total number of nodes removed, negative nodes removed, and ratio of positive nodes to removed nodes in node positive breast carcinoma. Eur J Surg Oncol 2006;
32:1082-8.
20. Fortin A, Dagnault A, Blondeau L, Vu TT, Larochelle M. The im- pact of the number of excised axillary nodes and of the percentage of involved nodes on regional nodal failure in patients treated by breast-conserving surgery with or without regional irradiation. Int J Radiat Oncol Biol Phys 2006;65:33-9.