□증례보고□
전립선암은 매년 유병률이 증가하고 있는 남성 종양이지 만, 남성 유방암은 아주 드물게 발병하고 2002년 미국 보고 에 의하면, 1년간 1,500명이 새롭게 진단되며, 전체 종양에 의한 사망의 0.1%를 차지할 것으로 추정하였다.1남성 유방 암과 전립선암은 스테로이드 호르몬이 병인에 중요한 역할 을 한다는 것과 유전자 이상과 연관성을 가진다는 공통점 이 있다.2이러한 공통점에도 불구하고, 남성에서 두 종양이 병발한 증례의 보고는 드물다. 종래의 외국 연구에서는 남
성 유방암 또는 전립선암 중 하나의 원발 병소 종양이 먼저 진단된 후, 타목시펜 (tamoxifen) 또는 에스트로겐 치료를 시 행한 후 병발한 경우이나,3-5본 증례에서는 61세 남자 환자 로 남성유방암과 전립선암이 외인성 요인이 없이 같은 시 기에 진단된 동시성 (synchronous) 종양으로 문헌고찰과 함 께 보고하고자 한다.
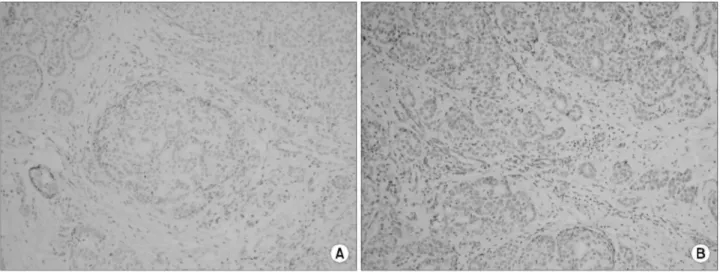
Fig. 1. (A) The tumor cell nests forming a solid mass, with pushing margin infiltrates into normal breast parenchyma (H&E, x100). (B) The tumor cells are large, with prominent nucleoli (H&E, x400).
남성에서 동시에 병발된 전립선암과 유방암
Male Patients with the Diagnoses of Synchronous Prostate and Breast Cancer
Chang Yell Lee, Chang Soo Park, Wan Lee, Hee Suk Kwak1, Mee Young Sol2, Moon Kee Chung
From the Departments of Urology, 1General Surgery and 2Pathology, Pusan National University College of Medicine, Busan, Korea
Prostate cancer and male breast cancer are similar in many ways, including the potential role of steroidal hormones in their pathogenesis and shared genetic abnormalities. However, the combination of these cancers in the same patient is rare. Herein, the case of a male patient, diagnosed with synchronous prostate and breast cancers, is reported. (Korean J Urol 2007;48:348-351)
Key Words: Synchronous neoplasms, Prostate cancer, Breast cancer
대한비뇨기과학회지 제 48 권 제 3 호 2007 부산대학교 의과대학
비뇨기과학교실, 1외과학교실,
2해부병리학교실
이창렬 박창수 이 완
곽희숙1 설미영2 정문기
접수일자:2006년 10월 30일 채택일자:2007년 1월 21일 교신저자: 정문기
부산대학교병원 비뇨기과 부산광역시 서구 아미동 1가 10번지
602-739
TEL: 051-240-7347 FAX: 051-247-5443 E-mail: mkchung@ pusan.
ac.kr
이 논문은 부산대학교 자유과제 학술연구 비 (2년)에 의하여 연구되었음.
348
이창렬 외:남성에서 동시에 병발된 전립선암과 유방암 349
증 례
61세 남자 환자는 체질량지수 (body mass index; BMI)가 22.86이었고, 음주력 및 간경변 등의 과거력은 없었다. 내원 3년 전부터 좌측 유방에 무통성 종물이 만져졌으나, 이에 관한 검사 및 치료는 하지 않았다. 1년 전 건강 검진에서 좌측 유방종물절제 조직검사를 시행하였고 병리조직검사 결과에서 침윤성 유관암으로 진단되었다 (Fig. 1). 또한 전 립선특이항원이 36.15ng/ml로 보고되어, 유방암치료 전에 전립선조직검사를 시행하였고, 우측 전엽 (5/10)에서 Gleason 점수 7 (4+3)인 선암으로 진단되었다. 골주사와 컴
퓨터단층촬영에서 전이 소견은 없었다.
먼저 변형 근치적 유방절제술을 시행하였고, 액와림프절 1곳 (1/6)에서 림프혈관계 침범 소견을 보였다. 조직학적으 로 중등도 분화도의 유관암이었으나, 상피내암종 소견은 없었다. 면역조직화학염색법에서 환자의 전립선암 조직 소 견과 비교하여 전립선특이항원, prostate associated protein antigen (PAP) 및 c-erbB2 염색 모두에서 음성이었고 (Fig. 2), 에스트로겐 수용체, 프로게스테론 수용체는 양성이었다. 이 후 4회에 걸쳐 독소루비신 (doxorubicin) 및 시클로포스파미 드 (cyclophosphamide) 항암치료를 하였고, 보조요법으로 술 후 9개월 동안 타목시펜을 경구 투여 중이다.
전립선암은 3개월간의 남성호르몬차단요법 후, 신경보존
Fig. 2. Immunohistochemical staining for the prostate-specific antigen (PSA) (A) and prostate associated protein antigen (PAP) (B) showing negative reactions in a breast ductal carcinoma.
Fig. 3. (A) The small compact tumor cell nests infiltrating into the normal prostatic parenchyma (H&E, x200). (B) The tumor cells have prominent basophilic nucleoli, which are characteristic of a prostatic adenocarcinoma (H&E, x400).
350 대한비뇨기과학회지:제 48 권 제 3 호 2007
치골후 근치적 전립선절제술과 골반림프절절제술을 시행하 였다. 술 후 병리조직 결과에서 전립선에 국한된 선암으로 Gleason 점수는 7 (3+4)로 술 전 병리조직검사와 달랐다 (Fig.
3). 또한 면역조직화학염색법에서 전립선특이항원과 PAP 염 색에서는 양성이었고 (Fig. 4), c-erbB2 염색은 음성이었다. 현 재 12개월 동안 경과 관찰 중이며 재발 소견은 없다.
고 찰
전체 종양 환자 중 다발성 원발성 약성종양의 유병률은 0.83%로 그 빈도가 낮다.6대부분의 환자는 남성으로, 가장 흔하게 병발하는 종양은 후두암과 폐암이고, 그 다음은 구 순암과 후두암이다. 병발하는 종양 사이에는 유사한 병리 학적 인과관계를 가지고 있었다.6
남성 유방암과 전립선암이 병발하는 원인을 설명하기 위 한 몇가지 가능성을 제기할 수 있다. 첫 번째로 최근 인구의 노령화와 식생활의 서구화로 전립선암의 유병률이 급격히 증가하고 있는 실정이다. 이로 인해 건강 검진 시 전립선특 이항원검사 등에 의해 우연히 무증상의 전립선암이 진단되 는 경우가 높아졌다. 따라서 남성 유방암은 아주 드문 질환 이지만, 1차암 진단 후 병기 결정 중의 영상진단검사에서 나, 치료 후 경과 관찰 중에 쉽게 2차암이 조기 발견될 수 있을 것이다. 둘째로 두 종양 사이에 직접적인 연관성이 있 는 경우이다. 그 중 하나는 병인에서 스테로이드 호르몬이 중요한 역할을 한다는 것이다. 클라인펠터 증후군이나 간 경변 환자에서 에스트로겐이 과다하여 호르몬의 균형이 깨 지면, 남성 유방암의 위험성이 높아지는 것으로 알려져 있 다.7 Karlsson 등5은 전립선암에서 에스트로겐 치료를 시행
한 경우 선행성 (antecedent) 또는 속발성 (metachronous)으로 남성 유방암이 발병할 위험성이 평균 4배 높아진다고 보고 하였다. Leibowitz 등4은 남성 유방암과 전립선암이 병발한 10 례 중 5례에서 타목시펜 치료를 시행하였다고 보고하였다.
또 다른 하나의 병인에 대한 가설은 공통된 유전자 감수 성 (genetic susceptibility)을 두 종양이 가진다는 것이다. 조 기에 유방암이 발병한 환자의 남자 친족에서 유방암과 전 립선암의 위험성이 높다고 알려져 있다.4 Diez 등8은 남성 유방암의 4-40%에서 BRCA-2의 생식세포 돌연변이 (ger- mline mutation)와 연관성이 있다고 하였다. 가족력 연구에 서 조기 발병한 전립선암 환자에서는 BRCA-2 돌연변이는 2%에서 나타나며, 유방암과 난소암의 조기 발병과 높은 연 관성을 가지는 것으로 보고되었다.5다른 여러 가족력 연구 에서도 유방암과 전립선암의 연관성이 있었고,9 특히 유방 암 환자군에서 BRCA-2 돌연변이를 동반한 가족에 대한 Cohort 연구에서 전립선암의 상대위험도 (relative ratio)가 4.65로 높게 나왔다.10Sigurdsson 등6은 BRCA-2 돌연변이가 남성 유방암과 전립선암 병발의 유전적 원인 인자라고 주 장하였다.
그 외에도 안드로겐 수용체의 돌연변이, 특정 유전자 (genetic locus)의 이형 접합 (heterozygosity)의 소실, bcl-2 발 현 등과도 연관성이 있을 것이라 추정하였다.3여러 가설들 이 있지만 두 종양의 유전적 및 병리학적 인과관계를 설명 하기 위해 정확한 검증이 이루어진 것은 없었다. 남성 유방 암의 치료는 변형 유방절제술을 주로 시행하였고, 전립선 암은 체외방사선 치료를 시행하였다 (Table 1).3,4
본 증례는 동시성 다발성 원발성 종양으로 에스트로겐, 타목시펜 등의 호르몬치료를 시행하지 않았고, 가계 조사 Fig. 4. Immunohistochemical staining for the prostate-specific antigen (PSA) (A) and prostate associated protein antigen (PAP) (B) showing positive reactions.
이창렬 외:남성에서 동시에 병발된 전립선암과 유방암 351
상 유방암의 가족력이 없었다. 따라서 병인에 대한 역학적 조사와 유전적 연관성에 대해서도 추가적인 연구가 필요할 것으로 생각한다. 또한 치료에 있어서도 다른 여러 증례와 비교하여, 특징적으로 남성 유방암과 전립선암 모두에서 근치적 절제술을 시행하였으므로 주의 깊은 경과 관찰이 필요할 것이다. 다발성 원발성 종양일지라도 치료방법, 술 후 생존율 등의 예후는 단일암과 차이는 없는 것으로 나타 났다.4따라서 남성 유방암과 전립선암의 병발이 진단된 경 우, 병인 규명을 위한 유전학적, 역학적 연구와 함께, 예후 향상을 위해 적절한 치료 방법의 선택과 추척 관찰을 시행 해야 할 것이다.
REFERENCES
1. Jemal A, Thomas A, Murray T, Thun M. Cancer statistics, 2002. CA Cancer J Clin 2002;52:23-47
2. Lopez-Otin C, Diamandis EP. Breast and prostate cancer: an analysis of common epidemiological, genetic, and biochemical features. Endocr Rev 1998;19:365-96
3. Ozet A, Yavuz AA, Komurcu S, Ozturk B, Safali M, Arpaci F, et al. Bilateral male breast cancer and prostate cancer: a
case report. Jpn J Clin Oncol 2000;30:188-90
4. Leibowitz SB, Garber JE, Fox EA, Loda M, Kaufman DS, Kantoff PW, et al. Male patients with diagnoses of both breast cancer and prostate cancer. Breast J 2003;9:208-12 5. Karlsson CT, Malmer B, Wiklund F, Gronberg H. Breast
cancer as a second primary in patients with prostate cancer- -estrogen treatment or association with family history of cancer? J Urol 2006;176:538-43
6. Sigurdsson S, Thorlacius S, Tomasson J, Tryggvadottir L, Benediktsdottir K, Eyfjord JE, et al. BRCA2 mutation in Icelandic prostate cancer patients. J Mol Med 1997;75:758-61 7. Sasco AJ, Lowenfels AB, Pasker-de Jong P. Review article:
epidemiology of male breast cancer. A meta-analysis of pub- lished case-control studies and discussion of selected aeti- ological factors. Int J Cancer 1993;53:538-49
8. Diez O, Cortes J, Domenech M, Pericay C, Brunet J, Alonso C, et al. BRCA2 germ-line mutations in Spanish male breast cancer patients. Ann Oncol 2000;11:81-4
9. Valeri A, Fournier G, Morin V, Morin JF, Drelon E, Mangin P, et al. Early onset and familial predisposition to prostate cancer significantly enhance the probability for breast cancer in first degree relatives. Int J Cancer 2000;86:883-7 10. Cancer risks in BRCA2 mutation carriers. The Breast Cancer
Linkage Consortium. J Natl Cancer Inst 1999;91:1310-6 Table 1. Treatment of patients with male breast cancer and prostate cancer
Patient No./age Prostate cancer diagnosis
Breast cancer Breast cancer Prostate cancer
at diagnosis
stage treatment treatment
of cancer PSA (ng/ml) Gleason score Clinical stage
Androgen ablation
1/47 years4 T1N0M0 MRM+tamoxifen 4.3 9 T2
+XRT
2/65 years4 T2N1M0 MRM+tamoxifen 15.3 8 T2 XRT
Lumpectomy+
3/72 years4 T1N0M0 1.8 6 T2 XRT
XRT+tamoxifen
4/62 years4 T1N0M0 MRM+tamoxifen 19.6 7 T2 XRT
5/69 years4 T2N0M0 MRM 6.0 6 T2 XRT
6/63 years4 T1N0M0 MRM 47.5 8 T3 XRT+tamoxifen
7/67 years4 T1N1M0 MRM+XRT 1.9 4 T1a None
8/66 years4 T1N0M0 MRM 11.8 7 T1c RP
MRM+XRT+
9/68 years4 T2N0M0 4.9 6 T1c None
tamoxifen
Metastatic disease
10/70 years4 T?N0M0 MRM N/A Poorly differentiated Orchiectomy
to bone
Metastatic disease Androgen ablation
11/67 years3 T?N1M0 MRM+XRT 20.8 6
to bone +XRT
12/61 years* T1N0M0 MRM 36.15 7 T2 RP
MRM: modified radical mastectomy, N/A: not applicable, PSA: prostate-specific antigen, RP: radical prostatectomy, XRT: external beam radiation therapy. *: author's case