남성 성기능 장애
MALE SEXUAL DYSFUNCTION
“The penis does not obey the order of its master, who tries to erect or shrink it at will. Instead, the penis erects freely while its master is asleep. The penis must be said to have its own mind, by any stretch of the imagination.”
-Leonardo da Vinci -
학습목적 : 성기능에 대한 신경생리 , 혈역동 , 약물학을 이해하여 발기부전에 대한 원인과 치료원칙을 파악할 수 있게 한다 .
학습목표 ( 한국의과대학장협의회 ) - 음경발기의 기전을 설명한다 .
- 음경발기의 3 가지 형태를 설명한다 . - 남성 성기능장애의 원인을 분류한다 , - 남성 성기능장애의 진단법을 열거한다 학습목표 : ( 대한비뇨기과학회 )
1. 남성의 성기능 생리를 설명한다 .
2. 남성 성기능 장애의 원인을 열거한다 .
3. 남성 성기능 장애의 진단방법과 치료방법을 열거한다 .
4. 지속성 음경발기증 (priapism) 을 정의하고 원인을 열거한다 . 5. 지속성 음경발기증의 응급 치료법을 설명한다 .
6. 혈정액 ( Hematospermia ) 의 원인 및 치료에 대해 설명한다 .
▪ Corpora cavernosa Support corpus spongiosum and glans
▪ Tunica albuginea (of corpora
cavernosa) Contains and protects erectile tissue Promotes rigidity of the corpora cavernosa
Participates in veno-occlusive mechanism
▪ Smooth muscle Regulates blood flow into and out of the sinusoids
▪ Ischiocavernosus muscle Pumps blood distally to hasten erection Provides additional penile rigidity during rigid erection
phase
▪ Bulbocavernosus muscle Compresses the bulb to help expel semen
▪ Corpus spongiosum Pressurizes and constricts the urethra lumen to allow
forceful expulsion of semen
▪ Glans Acts as a cushion to lessen the impact of the penis on
female organs
Provides sensory input to facilitate erection and
enhance pleasure
Facilitates intromission because of its cone shape
Penile Components and their Function during
erection
Figure 21-1 Artist's cross-sectional drawing
of the penis, depicting the inner circular and
outer longitudinal layers of the tunica albuginea as well as the
intracavernous pillars. The
longitudinal layer is absent in the ventral groove housing the corpus spongiosum.
Figure 21-2 Micrograph of the human tunica
albuginea, showing the interwoven elastic
fibers and the finer collagen fibers.
(Hart stain,=100.)
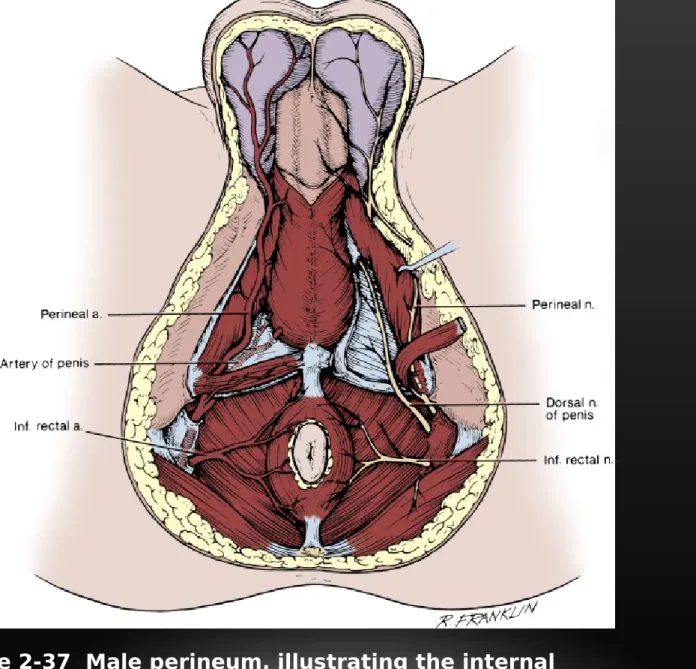
Figure 2-37 Male perineum, illustrating the internal pudendal artery and its branches on the left and the pudendal nerve and its branches on the right
I. Physiology of penile erection
1. Innervation of the Penis 1) Peripheral nerve
(1) sympathetic( T12-L2 ); detumescence, emission, ejaculation
sympathetic chain --- superior hypogastric plexus --- hypogastric n.--- pelvic plexus --- cavernous n.
(2) parasympathetic( S2-4 ); tumescence
pelvic n. (nervi ergentes)---pelvic n.---pelvic plexus--- cavernous n.
(3) Somatic
pudendal n.
2) Central mechanisms:
brain exert a modulatory influence over spinal reflex (1) Reflexogenic erectile mechanism
pudendal afferent --- sacral pelvic parasympathetic efferent
(2) Psychogenic erectile mechanism
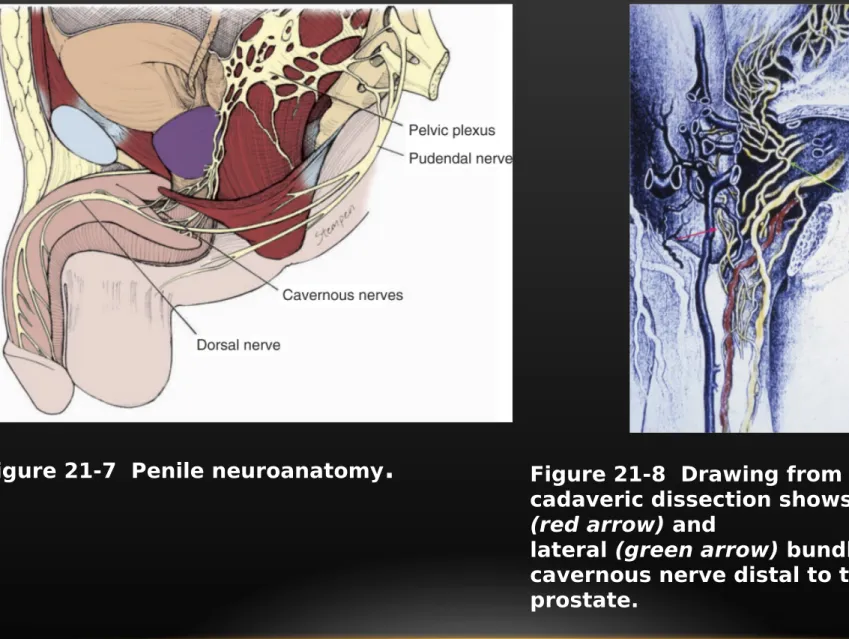
Figure 21-7 Penile neuroanatomy
.
Figure 21-8 Drawing from a human cadaveric dissection shows the medial (red arrow) andlateral (green arrow) bundles of the cavernous nerve distal to the
prostate.
Table 21-3 -- Brain Centers Involved in Sexual Function
Level Region Function
Forebrain Medial amygdala Control sexual motivation
Stria terminalis
Pyriform cortex Inhibits sexual drive (hypersexuality when destroyed)
Hippocampus Involved in penile erection
Right insula and inferior frontal
cortex Increased activity during visually evoked sexual stimulation\ (sexual arousal)
Left anterior cingulate cortex
Hypothalam
us Medial preoptic area (MPOA) Ability to recognize a sexual partner, integration of
hormonal and sensory cues
Paraventricular nucleus (PVN) Facilitates penile erection (through oxytocin neurons to
lumbosacral spinal autonomic and somatic efferents)
Brain stem Nucleus paragigantocellularis Inhibits penile erection (through serotonin neurons to
lumbosacral spinal neurons and interneurons) A5-catecholaminergic cell group Noradrenergic innervation of anterior horn motor
neurons
to perineal striated muscles
Locus ceruleus
Midbrain Periaqueductal gray Relay center for sexually relevant stimuli
2. Anatomy and Hemodynamics of Penile Erection
1) Arterial supply
internal iliac a. internal pudendal a. dorsal a.
cavernous (deep) a.
bulbourethral a.
2) Venous supply
superficial dorsal v. saphenous v.
deep dorsal v.
cavernous v. emissary v. periprostatic plexus internal pudendal v.
urethral v.
3) Sinusoidal system
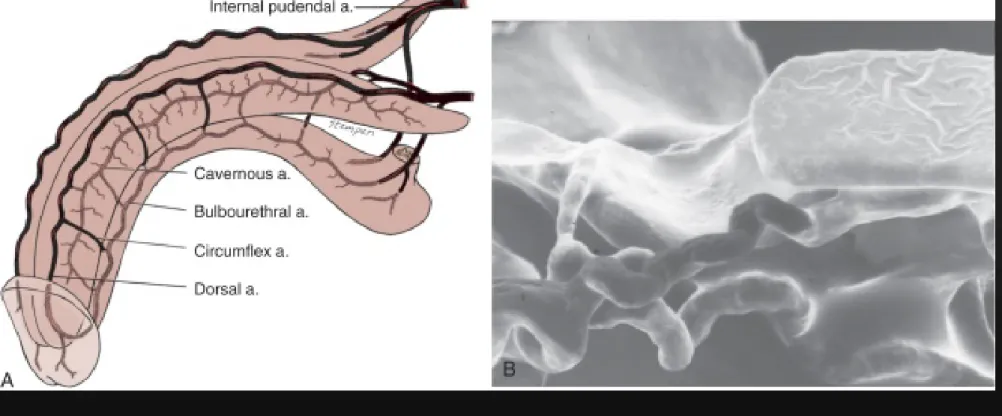
Figure 21-3 A, Penile arterial supply. B, Scanning electron micrograph of a human penile cast showing helicine arteries opening directly into the
sinusoids without intervening capillaries
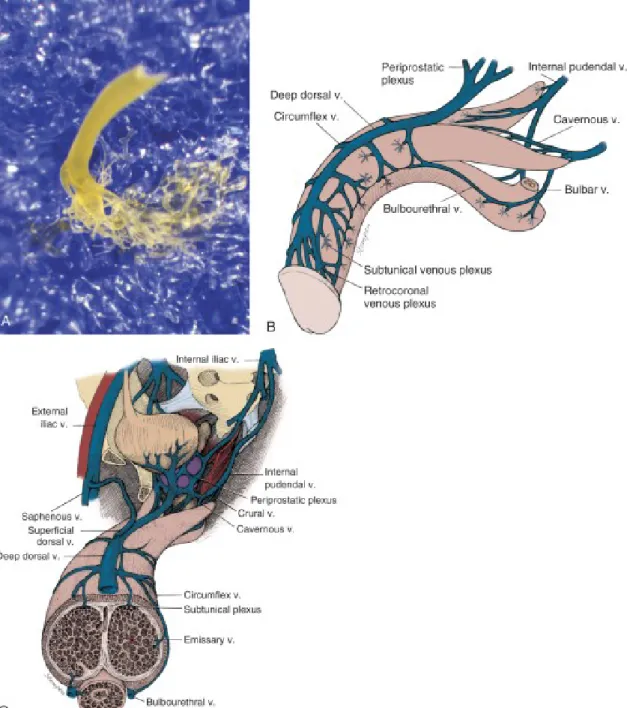
Figure 21-4 A, Photograph of
an emissary vein with subtunical
venous plexus of a human penile cast. The cast was made by
injecting blue material into the
corpus cavernosum and yellow
material into the deep dorsal vein. The skin and tunica albuginea
were then digested away with
KOH solution. B, and C, Penile
venous drainage.
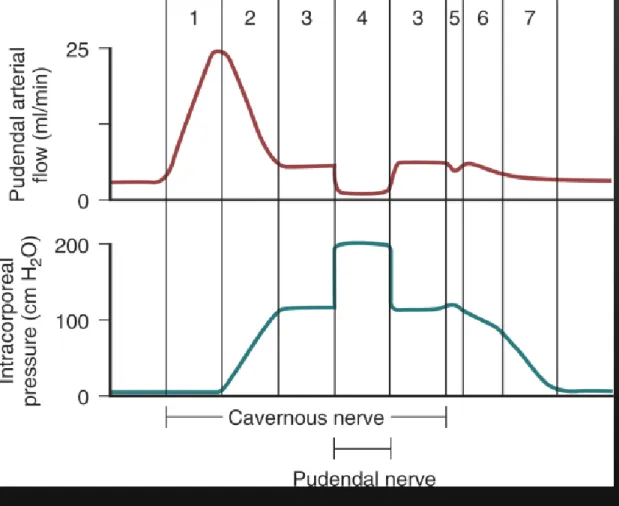
Figure 21-6 Blood flow and intracavernous pressure changes during the seven phases of penile erection and detumescence: 0, flaccid; 1, latent; 2, tumescence; 3, full erection; 4, rigid erection; 5, initial detumescence;
6, slow detumescence; 7, fast detumescence.
3. Mechanisms of Penile Erection
1) flaccid state
arteries & arterioles are tortuous & constricted sinusoidal compliance increase
2) erection state
arterial smooth muscle relax & resistance drop to minimum sinusoidal compliance decrease
compressed against non-compliant tunica albuginea
compressed emissary vein
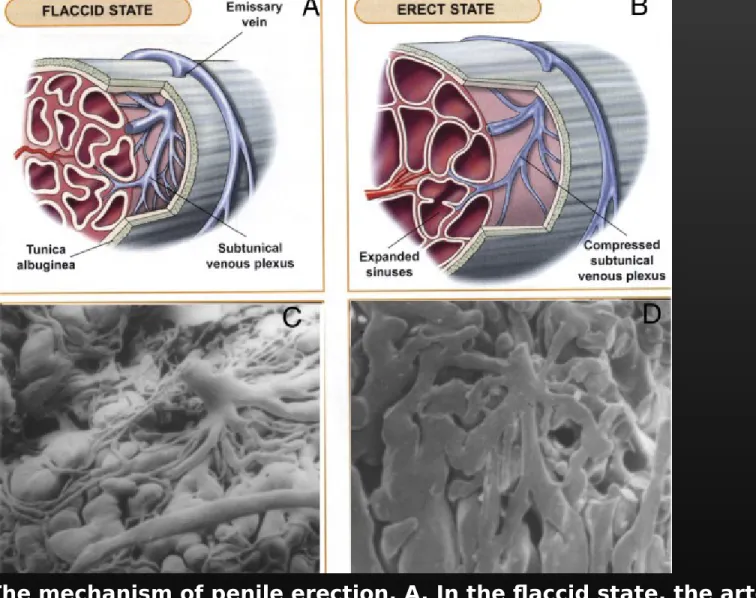
Figure 21-5 The mechanism of penile erection. A, In the flaccid state, the arteries, arterioles, and
sinusoids are contracted. The intersinusoidal and subtunical venous plexuses are wide open, with free
flow to the emissary veins. B, In the erect state, the muscles of the sinusoidal wall and the arterioles
relax, allowing maximal flow to the compliant sinusoidal spaces. Most of the venules are compressed
between the expanding sinusoids. The larger venules are sandwiched and flattened between the distended
sinusoids and the tunica albuginea. This effectively reduces the venous capacity to a minimum.
C, and D, Scanning electron micrographs of casts of a canine subtunical venous plexus in the flaccid and erect states, respectively.
4. Hormones & Sexual Function m ale sexual maturation
maintain sexual interest, seminal emission
5. Neurotransmitter & the Pharmacology of Erection
1) Adrenergic; intracavernous smooth muscle contraction, detumescence 2) Cholinergic; smooth muscle relaxation, erection
(1) inhibition of adrenergic nerve via inhibitory interneuron
(2) release of EDRF (endothelium-derived relaxing factor) from cholinergic nerve terminal
(3) nonadrenergic-noncholinergic (NANC) NO release
c-GMP accumulation
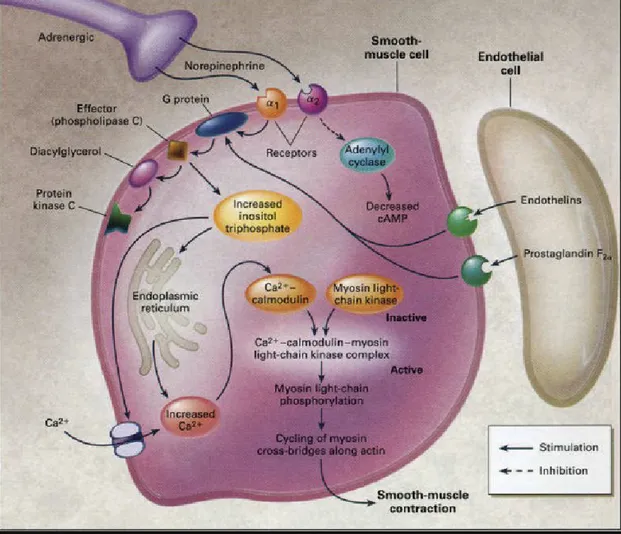
Figure 21-9 Molecular mechanism of penile smooth muscle contraction.
Norepinephrine from
sympathetic nerve endings and endothelins and prostaglandin F2α from the endothelium activate receptors on smooth muscle cells to initiate the cascade of reactions that eventually result in
elevation of intracellular calcium concentrations and smooth muscle contraction. Protein kinase C is a regulatory component of the Ca2+- independent, sustained phase of agonist-induced
contractile responses. (From Lue TF: Erectile dysfunction. N Engl J Med 2000;342:1802-1813. Copyright © 2000 Massachusetts Medical Society.)
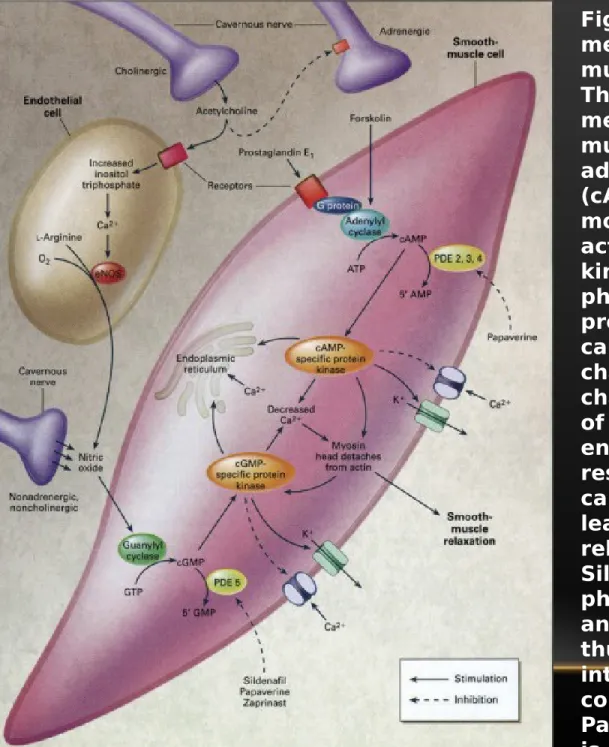
Figure 21-11 Molecular
mechanism of penile smooth muscle relaxation.
The intracellular second
messengers mediating smooth muscle relaxation, cyclic
adenosine monophosphate (cAMP) and cyclic guanosine monophosphate (cGMP),
activate their specific protein kinases, which
phosphorylate certain proteins to
cause opening of potassium channels, closing of calcium channels, and sequestration of intracellular calcium by the endoplasmic reticulum. The resultant fall in intracellular calcium
leads to smooth muscle relaxation.
Sildenafil inhibits the action of phosphodiesterase 5 (PDE5) and
thus increases the intracellular
concentration of cGMP.
Papaverine is a nonspecific phosphodiesterase
inhibitor. eNOS, endothelial nitric
oxide synthase; GTP, guanosine
triphosphate. (From Lue TF:
Erectile dysfunction. N Engl J Med 2000;342:1802-1813.
Copyright © 2000
Massachusetts Medical Society.)
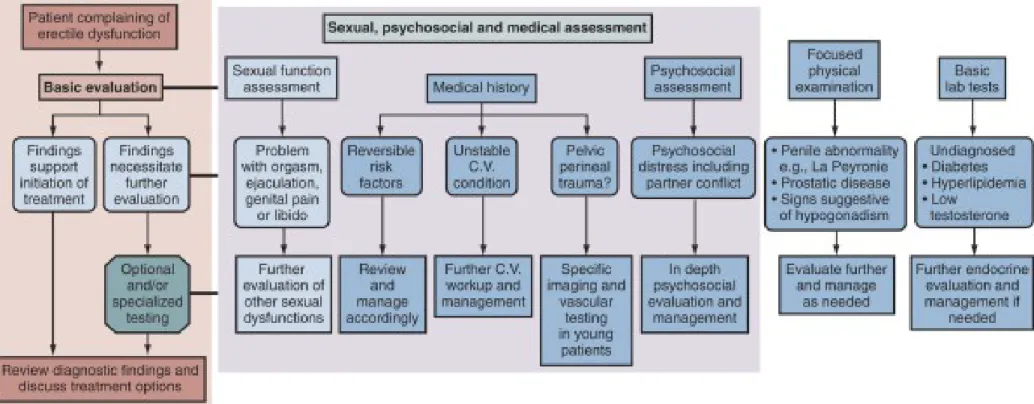
II. Diagnosis
Main Treatments Diagnostic Tests
Before 1970 Psychosexual therapy Psychosexual history 1970s Penile prosthesis
psychosexual therapy Medical
psychosexual history sleep lab
1980s Yohimbine
intracavernous transurethral therapy
vacuum device
History
physical examination testosterone,
duplex ultrasound
DICC (goal-directed approach) 1990s-
Present Oral phosphodiesterase-5
inhibitors Process-of-care model
1st ICUD algorithm
2nd ICUD algorithm (patient-centered approach)
Table 22-1 -- Evolution in the Diagnostic Workup for ED
DICC, dynamic infusion cavernosometry and cavernosography.
ICUD, International Consultation on Urological Diseases.
* Goal-directed approch
HISTORY & PHYSICAL EXAM
PSYCHOLOGICAL EVALUATION Tx OPTIONS DISCUSSED
serum testosterone NPT
Prolactin Visual sex
sti,ulation
Glycosylated Hgb
2nd Visit Partial or No Response
Full 30’ Erection Pharmacologic Intracavernosal (evenafter exercise) injection
Duplex Doppler of Penile Arteries
2' Intracavernosal Injection Psychological Rx
Intracavernosal Rx Regimen
R/O Neurogenic Impotence Arterial disease No arterial disease
Vacuum Device Therapy
Pudendal arteriography
Cavernosography
(only if surger is planned)
& Cavernosometry
if venous surgery planned
Penile Prosthesis
Figure 22-1 Diagnostic algorithm for ED recommended by the ICSM.
1. Arterial impotence
1) PBI (penile brachial index)
Penile Systolic Blood Pressure/brachial systolic pressure=PBI
normal >0.8, Impotent male <0.6
2) Intracavernous injection of vasoactive amine
3) Duplex sonography and pulsed Doppler analysis peak systolic velocity (PSV) > 25 cm / sec
end diastolic velocity (EDV) < 5 cm / sec
resistive index = PSV-EDV/PSV
Figure 22-7 Artist's conception of the changes
in diameter and flow waveform in the cavernous arteries induced by
intracavernous injection of
prostaglandin E1 in a potent young man as
demonstrated by duplex ultrasound.
Forceful
concentric pulsations are particularly noticeable during full erection.
F
igure 21-6 Blood flow andintracavernous pressure changes during the seven phases of penile erection and detumescence: 0, flaccid; 1, latent; 2, tumescence; 3, full erection; 4, rigid
erection; 5, initial detumescence; 6, slow detumescence; 7, fast detumescence.
Figure 22-5 Collateral circulation connecting the right dorsal artery (RDA) to the right
cavernous artery (RCA) and the left cavernous artery (LCA) is shown by color duplex
ultrasound in a longitudinal view.
4) Internal iliac or pudendal arteriography
2. Venous Impotence & Disease of Cavernous Smooth Muscle
Dynamic infusion cavernosometry and cavernosography (DICC)
3. Neurologic Impotence 1) Somatic nervous system
2) Autonomic nervous system 3) Central nervous system
occur during a most REM sleep, also present during non- REM sleep
3-4 episode per night 90 min interval 20-25% to total sleep time ( 1.5 hour )
disrupted by sleep apnea, periodic leg movement,
nocturnal myoclonus
(1) mercury strain gauge (2) stamp
(3) Rigiscan
penile base > 3 cm, penile tip > 2 cm
rigidity 70% or greater, enable to intromission
Figure 21-13 A functional classification of impotence. Note that it is unlikely for an individual patient's impotence to derive solely from one source. Most cases have a psychogenic component of varying degree, and systemic
diseases and pharmacologic effects can be concomitant and causative.
(Modified from Carrier S, Brock G, Kour NW, Lue TF: Pathophysiology of erectile dysfunction. Urology 1993;42:468-481, with permission of Exerpta Medica, Inc.)
Figure 22-2 Treatment algorithm for ED
recommended by the ICSM.
1. Vascular surgery 1) Arterial origin
relieve of stenosis or occlusion of extrapenile artery (internal iliac, internal pudendal, dorsal artery)
epigastric-corporeal anastomosis epigastric artery to deep dorsal vein 2) Venous origin
ligation superficial and deep dorsal vein
repair of fistula between glans & cavernous body
epigastric artery to deep dorsal vein
2. Penile prosthesis
1) Semirigid, Malleable, Mechanical/Interdigitating 2) Inflatable
a. Single component
b. Two component
c. Threee component
3. Pharmacotherapy
1) Intracavernous injection of vasoactive agents papaverine, phentolamine, prostaglandin E1 Trimix
2) Phosphodiesterase type 5 (PDE5) inhibitor 3) other drugs
yohimbine testosterone
4. Vaccum suction device
Male sexual dysfunction involving emission, ejaculation & orgasm
1. Physiology of Emission , Ejaculation, & Orgasm
pudendal nerve --- upper lumbar spinal sympathetic nuclei hypogastric nerve --- activate secretion and transport sperm
somatoefferent of pudendal nerve to contract bulbocavernous
muscle
emission ; semen into bulbous urethra
ejaculation ;
2. Disorders Affecting Emission, Ejaculation, &
Orgasm
1) Causes
bilateral sympathectomy at L2 level
high bilateral retroperitoneal lymphadenectomy retrograde ejaculation
2) Treatment
elimination of alpha blocking agent alpha sympathomimetics
electroejaculation
3. Premature ejaculation desensitization
squeezing technique
application of local anesthetics or condom
PRIAPISM 1. Type
1) high flow 2) low flow 2. Causes
1. unknown(60%) : prolonged sexual stimulation
2. associated disease : Leukemia, sickle cell disease, pelvic tumor, pelvic infection
3. penile trauma
4. spinal cord trauma
5. use of medication
3. Pathogenesis & clinical findings
Erection Priapism
Involved portion corpora cavernosa orpora cavernosa corpus spongiosum
glans
Cause vasodilation of penile a. obstruction of venous outflow venoarterial disturbance
Sexual desire present absent
pain absent
present (ischemic)
duration minutes to hours hours to days
High-flow priapism Low-flow priapism
Characteristics painless, high PO2, bright red bloodpainful, low PO2, dark blood
not so rigid penisrigid penis, soft glans Mechanism pain, perineal trauma 로 인한 venous outflow가 차단되면서
Cavernosoarterial shunt blood stasis 로 인 한 hypoxia
Etiology trauma, idiopathic veno-occlusive disease Medical status not so emergency emergency
Treatment embolization disease specific
Figure 22-6 A, Color duplex ultrasonograph in a patient with high-flow
priapism shows turbulent flow within the corpus cavernosum resulting from rupture of a branch of the left cavernous artery. B, On selective penile
arteriography, a ruptured branch of the cavernous artery is seen filling the cavity.
4. Treatment : Urologic emergency
1) sedation followed by enema of ice-saline solution 2) Ketamine hydrochloride I.V. or I.M.
3) epidural or spinal anesthesia
4) sludged blood evacuation with large needle 5) shunting fistula
6) management of primary disease
HEMOSPERMIA ( BLOODY EJACULATION )
not uncommon complaint of middle aged men usually the wife recognize the symptoms
1. Causes
1) hyperplasia of mucosa of seminal vesicle 2) adenomatous polyp
3) prostatic intraductal carcinoma 4) utricular cyst
1. Treatment
1) diethylstilbestero
2) electrocoagulation of granulation of posterior urethra 3) needle aspiration of utricular cyst
First
Author Year of
Report Number of
Subjects Age in Years
(range) Flaccid Length (cm)
Stretched (S) or Erect
(E) Length (cm) Country
Kinsey 1948 2770 20-59 9.7 15.5 (E) United
States
Bondil 1992 905 17-91 10.7 16.74 (S) France
Da Ros 1994 150 NA NA 14.5 (E) Brazil
Wessells 1996 80 21-82 8.85 12.45 (S), 12.89
(E) United States Ponchiett
i 2001 3300 17-19 9 12.5 (S) Italy
Ajmani 1985 320 17-23 8.16 NA Nigeria
Schneider 2001 111 18-19 8.6 14.48 (E) Germany
32 40-68 9.22 14.18 (E)
Awwad 2003 271 (N) 17-83 9.3 13.5 (S) Jordan
109 (ED) 22-68 7.7 11.6 (S)
E, erect length; ED, erectile dysfunction; N, normal; NA, not available; S, stretch length
.
Table 21-1 -- Penile Length in Adults
Modified from Awwad Z, Abu-Hijleh M, Basri S, et al: Penile measurements in normal adult Jord anians and in patients with erectile dysfunction. Int J Impot Res 2005;17:191-195.