Undergoing Percutaneous Coronary Intervention
Bon-Kwon Koo, MD, PhD; Katsuhisa Waseda, MD, PhD; Hyun-Jae Kang, MD, PhD;
Hyo-Soo Kim, MD, PhD; Chang-Wook Nam, MD, PhD; Seung-Ho Hur, MD, PhD;
Jung-Sun Kim, MD, PhD; Donghoon Choi, MD, PhD; Yangsoo Jang, MD, PhD;
Joo-Yong Hahn, MD, PhD; Hyeon-Cheol Gwon, MD, PhD; Myeong-Ho Yoon, MD, PhD;
Seung-Jea Tahk, MD, PhD; Woo-Young Chung, MD, PhD; Young-Seok Cho, MD, PhD;
Dong-Ju Choi, MD, PhD; Takao Hasegawa, MD; Toru Kataoka, MD; Sung Jin Oh, MD;
Yasuhiro Honda, MD; Peter J. Fitzgerald, MD, PhD; William F. Fearon, MD
Background—We sought to investigate the mechanism of geometric changes after main branch (MB) stent implantation and to identify the predictors of functionally significant “jailed” side branch (SB) lesions.
Methods and Results—Seventy-seven patients with bifurcation lesions were prospectively enrolled from 8 centers. MB intravascular ultrasound was performed before and after MB stent implantation, and fractional flow reserve was measured in the jailed SB. The vessel volume index of both the proximal and distal MB was increased after stent implantation. The plaque volume index decreased in the proximal MB (9.1⫾3.0 to 8.4⫾2.4 mm3/mm, P⫽0.001), implicating plaque shift, but not in the distal MB (5.4⫾1.8 to 5.3⫾1.7 mm3/mm, P⫽0.227), implicating carina shifting to account for the change in vessel size (N⫽56). The mean SB fractional flow reserve was 0.71⫾0.20 (N⫽68) and 43% of the lesions were functionally significant.
Binary logistic-regression analysis revealed that preintervention % diameter stenosis of the SB (odds ratio⫽1.05; 95% CI, 1.01 to 1.09) and the MB minimum lumen diameter located distal to the SB ostium (odds ratio⫽3.86; 95% CI, 1.03 to 14.43) were independent predictors of functionally significant SB jailing. In patients with ⱖ75% stenosis and Thrombolysis In Myocardial Infarction grade 3 flow in the SB, no difference in poststent angiographic and intravascular ultrasound parameters was found between SB lesions with and without functional significance.
Conclusions—Both plaque shift from the MB and carina shift contribute to the creation/aggravation of an SB ostial lesion after MB stent implantation. Anatomic evaluation does not reliably predict the functional significance of a jailed SB stenosis.
Clinical Trial Registration: http://www.clinicaltrials.gov. Unique Identifier: NCT00553670.
(Circ Cardiovasc Interv. 2010;3:113-119.)
Key Words: coronary disease 䡲 stenosis 䡲 stents 䡲 imaging 䡲 physiology
A
therosclerosis occurs frequently at the branching points of a coronary artery.1Percutaneous coronary interven- tion of these lesions is technically difficult and associated with higher event rates.2– 4 To develop improved strategies and devices, better insight into both the anatomic and func- tional aspects of bifurcation lesions is required.Editorial see p 94 Clinical Perspective on p 119
A side branch (SB) ostial stenosis is commonly aggravated after main branch (MB) stent implantation. This phenomenon
has long been believed to occur mainly because of the shift of MB plaque to the SB ostium (so-called “snowplowing”). A recent angiographic study, however, suggested that an alter- ation in the location of the carina, and not plaque shift, was the main mechanism for SB stenosis aggravation after MB stent implantation.5 We hypothesized that there could be some plaque shift and carina shift to the SB after MB stent implantation in bifurcation lesions.
To understand the clinical significance of SB ostial steno- sis, no matter what its mechanism, a functional evaluation is also needed, as previous reports have shown that there is a
Received June 17, 2009; accepted February 22, 2010.
From the Division of Cardiovascular Medicine, Interventional Cardiology, Stanford University Medical Center (B.K.K., K.W., Y.H., P.J.F., W.F.F.), Stanford, Calif; Department of Internal Medicine, Seoul National University Hospital (B.K.K., H.J.K., H.S.K.), Seoul, Korea; Department of Internal Medicine, Keimyung University Dongsan Medical Center (C.W.N., S.H.H.), Daegu, Korea; Department of Internal Medicine, Yonsei Cardiovascular Center (J.S.K., D.C., Y.J.), Seoul, Korea; Department of Medicine, Samsung Medical Center (J.Y.H., H.C.G.), Seoul, Korea; Department of Internal Medicine, Ajou University School of Medicine (M.H.Y., S.J.T.), Gyeonggi-Do, Korea; Department of Internal Medicine, Seoul National University Boramae Hospital (W.Y.C.), Seoul, Korea; Department of Internal Medicine, Seoul National University Bundang Hospital (Y.S.C., D.J.C.), Gyeonggi-Do, Korea; Department of Internal Medicine, Osaka City University Graduate School of Medicine (T.H., T.K.), Osaka, Japan; and Department of Internal Medicine, NHIC Ilsan Hospital (S.J.O.), Gyeonggi-Do, Korea.
Correspondence to William F. Fearon, MD, Division of Cardiovascular Medicine, Interventional Cardiology, H2103, Stanford University Medical Center, 300 Pasteur Dr, Stanford, CA 94305. E-mail [email protected]
© 2010 American Heart Association, Inc.
Circ Cardiovasc Interv is available at http://circinterventions.ahajournals.org DOI: 10.1161/CIRCINTERVENTIONS.109.887406 113
discrepancy between the angiographic appearance and the physiological significance of “jailed” SB lesions.6,7 A more complete evaluation of the changes in plaque and vessel geometry that create the angiographic lumen change after stent implantation could clarify the mechanism of this phenomenon.
The primary aim of this study was to investigate the mechanism of geometric changes in the SB ostium after MB stent implantation in a coronary bifurcation and to identify the predictors of functionally significant SB stenosis by performing intravascular ultrasound (IVUS) and by measur- ing fractional flow reserve (FFR).
Methods Patient Population
Patients with de novo proximal or mid left anterior descending- diagonal coronary bifurcation lesions with a planned provisional SB intervention strategy were prospectively and consecutively enrolled from 8 centers (United States, Japan, and Korea). Each center was assigned to enroll 10 patients. The study protocol was approved by the institutional review board at each participating center, and all patients provided written, informed consent. To be included, the minimum diameter of the SB required was⬎2 mm, the SB vessel length was⬎40 mm, and the SB lesion length was ⬍10 mm by visual estimation. SBs without significant stenosis were also in- cluded in this study. Patients were excluded if any 1 of the following was present: ST-segment elevation myocardial infarction, left main stenosis, totally occluded lesion, angiographically visible thrombus, a significant lesion within the MB proximal to the stented segment, significant distal lesion (diameter stenosis⬎50%) at an SB, regional wall motion abnormalities of the stented artery and SB segments, left ventricular ejection fractionⱕ40%, serum creatinine ⱖ2 mg/dL, predilatation of the SB before the MB stent implantation, or a contraindication to adenosine. All patients underwent MB IVUS before and after MB stent implantation and FFR of the jailed SB lesions.
Study Procedure
Coronary stenting of the MB was performed with standard interven- tional techniques. Postdilatation of the MB stent was performed at the discretion of the operator. IVUS was performed in a standard fashion with an automated, motorized pullback system (0.5 mm/s) with commercially available imaging systems (Boston Scientific/
SCIMED, Minneapolis, Minn or Volcano Corporation, Rancho Cordova, Calif [N⫽4]). In the case of a very tight MB stenosis, predilatation with an undersized balloon was allowed before IVUS.
Intracoronary nitroglycerin (100 to 200g) was administered before each IVUS run.
FFR was measured in the SB after MB stenting with a 0.014-in.
pressure guide wire (PressureWire, Radi Medical Systems, Uppsala, Sweden) as previously described.6 The pressure wire was passed through the struts of the MB stent, and FFR was measured at least 5 mm distal to the jailed SB stenosis. Hyperemia was induced with an intracoronary bolus administration (⬎80 g) of adenosine or ATP. Lesions with FFR⬍0.75 were considered functionally signif- icant. FFR measurement was not mandatory in the case of an SB stenosis⬍50% or SB total occlusion (Thrombolysis In Myocardial Infarction 0 or 1 flow) after MB stent implantation. For those cases, a default value of 0.90 was recorded for an insignificant stenosis and 0.30 for a total occlusion.
Quantitative Coronary Angiography and IVUS Analysis
Both quantitative coronary angiography (QCA) and IVUS analysis were performed by an independent core laboratory at Stanford University Medical Center. QCA was performed before and after MB stent implantation by a single experienced observer, who was
blinded to the FFR value and IVUS findings. With use of the guiding catheter for calibration and an edge-detection system (Quant32, Sanders Data Systems, Palo Alto, Calif), the reference diameters, minimal lumen diameter, and lesion length were measured, and the percent diameter stenosis was calculated. MBs and SBs were analyzed separately. The proximal and distal MB was considered as a single vessel. For the percent diameter stenosis, average diameters of proximal and distal reference segments were used for MB lesions but only the distal reference diameter for the SB lesions. When SB flow was Thrombolysis In Myocardial Infarction grade 0 or 1 after MB stent implantation, the minimal lumen diameter was recorded as 0 mm. The angle of bifurcation was measured between the distal MB and SB.
Previous studies have suggested that the mechanism of SB lumen narrowing and plaque distribution is different depending on the location of a lesion in the MB.8,9Shimada et al8showed that more eccentric plaque with a negative remodeling was seen in bifurcation lesions located distal to the SB. Therefore, there would be more carina shift if the minimal lumen diameter is located at a distal MB.
The MB lesion was classified as type A when the site of minimal lumen diameter was located in the MB proximal to the takeoff of the SB, and as type B when it was located in the MB distal to the takeoff of the SB.
IVUS analysis was done by an independent observer blinded to the clinical, FFR, and QCA information. Quantitative analyses were performed with computerized planimetry software (echoPlaque, Indec Systems Inc, Santa Clara, Calif) as previously described.10 Intraobserver variability has been reported previously.11 Minimal lumen area was measured at the narrowest luminal cross section, and the reference area at the most normal-looking cross section within 10 mm of the lesion without an intervening SB. The vessel remodeling ratio was defined as the ratio of the vessel area at the site of minimal lumen area and that of the reference site. Proximal reference was used for type A lesions and distal reference, for type B and SB lesions.
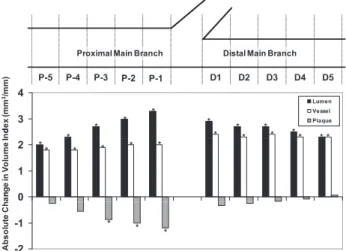
For the volumetric analysis, lumen and vessel areas were mea- sured at 1-mm intervals starting 5 mm distal to the takeoff of the SB and ending 5 mm proximal to the takeoff (Figure 1). Volumes were calculated by Simpson’s rule. The volume index was derived from each volume parameter according to the formula of volume/mea- sured length (mm3/mm). For poststenting IVUS measurement, the starting point of the proximal MB segment was determined by using the distance from the carina obtained from the prestenting IVUS analysis. To compare the changes in matched segments before and after stent implantation, both the proximal and distal MB segments were divided into 1-mm-long subsegments and numbered from 1 (nearest to the SB) to 5 (Figure 1). For each subsegment, vessel,
Proximal Main Branch Distal Main Branch
P 1 P 3 P 2
P 4
P 5 D1 D2 D3 D4 D5
3 4
Lumen Vessel Plaque
P-1 P-3 P-2
P-4
P-5 D1 D2 D3 D4 D5
dex (mm3/mm)
*
* *
*
*
* *
*
*
* *
* * *
0 1 2
nge in Volume Ind
** * * * *
-2 -1
Absolute Chan
* *
*
Figure 1. Absolute changes in volume indices according to the distance from an SB. *P⬍0.005; comparison between pre- and poststent implantation indices by repeated-measures ANOVA and post hoc test.
lumen, and plaque volume indices were calculated from the mean values of each available cross-sectional slice in the 1-mm-long segment.12
Statistical Analysis
Data are presented as means⫾SDs for continuous variables and frequency for categorical variables. Comparison of continuous vari- ables was performed with the Student t test. Repeated-measures ANOVA was conducted for the analysis of IVUS parameters by distance, and the probability value⬍0.005 was considered to be significant on post hoc test. Analysis of discrete variables was performed with the 2 test. Correlations between the FFR and angiographic and IVUS parameters were evaluated by Spearman correlation analysis. A binary logistic-regression analysis was per- formed to find the predictors of a functionally significant SB luminal narrowing after MB stenting. Angiographic parameters (vessel size, lesion severity, lesion length, bifurcation angle, and lesion location), which can influence the functional significance of SB narrowing, were included in this model. All statistical analyses were performed with SPSS version 11.0., and a probability value of⬍0.05 was considered statistically significant.
Results
From November 2007 to January 2009, 85 patients were enrolled, and 77 patients who met the inclusion criteria were included in this study. Clinical, angiographic, and procedural
characteristics are shown in Table 1. After exclusion of the cases with an intervening second SB (n⫽6) or inadequate images (n⫽15), MB IVUS was available in 58 patients for 2-dimensional analysis and in 56 patients for 3-dimensional analysis. In 7 cases, baseline IVUS was performed after predilatation (balloon size, 2.1⫾0.3 mm; balloon artery ratio, 0.75⫾0.14).
Two-Dimensional IVUS Analysis
Preinterventional 2-dimensional IVUS analysis results are shown in Table 2. At a reference segment, all IVUS param- eters were larger in type A lesions. At the site of minimum lumen area, vessel and plaque areas were larger in type A lesion. However, lumen area was not different between the 2 groups (type A versus type B, 2.0⫾1.1 versus 2.1⫾1.1, P⫽0.753). There was no difference in the remodeling ratio between the 2 groups (type A versus type B, 0.94⫾0.15 versus 0.97⫾0.17, P⫽0.529).
Three-Dimensional IVUS Analysis Before and After MB Stenting
Sequential 3-dimensional IVUS analysis was available in 56 patients (Table 3). In contrast to the other volume indices, the plaque volume index of the distal segment was not changed after stent implantation (5.4⫾1.8 versus 5.3⫾1.7 mm3/mm, P⫽0.227). When each 1-mm volume segment was compared, all changes in vessel and lumen volume indices after stent implantation were significant (P⬍0.005). However, the change in plaque volume index was significant only at P-1 to P-3 segments (P-1: 9.7⫾3.3 to 8.4⫾2.5 mm3/mm, P-2:
9.4⫾3.2 to 8.4⫾2.4 mm3/mm, P-3: 9.2⫾3.3 to 8.3⫾2.5 mm3/ mm; Figure 1).
FFR Versus Angiographic and IVUS Parameters FFR was available in 68 SB lesions. The pressure wire failed to recross the SB in 7 cases and dissection (⬎type B) occurred in 3 cases. The mean FFR was 0.71⫾0.20, and 29 lesions (43%) were functionally significant. FFR was⬍0.75 in 18 of 33 lesions (54.5%) withⱖ75% diameter stenosis and in 10 lesions (29.4%) with⬍75% stenosis.
Table 1. Clinical, Angiographic, and Procedural Characteristics Patient Characteristics
Age, y 60⫾10
Male 52 (68)
Stable angina 35 (46)
Diabetes 22 (29)
Previous revascularization 12 (16)
Angiographic and procedural characteristics Bifurcation type (medina classification)
1,1,1 20 (26)
1,0,1 13 (17)
0,1,1 11 (14)
Y type (angle⬍70 degrees) 69 (90)
MB stent
Cypher/TAXUS/Xience V 43 (56)/15 (20)/4 (5)
Diameter/length, mm 3.1⫾0.4/29.6⫾11.9
SB intervention 35 (46)
Quantitative coronary angiography Preintervention
MB reference diameter, mm 3.1⫾0.5
MB percent stenosis, % 63⫾14
MB lesion length, mm 19.5⫾10.3
SB reference diameter, mm 2.1⫾0.4
SB percent stenosis, % 45⫾20
SB lesion length, mm 5.9⫾4.4
Post-MB stent implantation
MB percent stenosis, % 8.0⫾8.9
SB percent stenosis, % 71⫾17
Jailed SB FFR 0.71⫾0.20
Values are expressed as n (%) or mean⫾SD.
Table 2. Preinterventional 2-Dimensional IVUS Measurements
Total
Type A Lesion (n⫽27)
Type B Lesion
(n⫽31) P * Reference segment
Lumen area, mm2 5.5⫾2.4 6.4⫾2.6 4.7⫾2.0 0.007 Vessel area, mm2 11.5⫾4.0 13.8⫾4.0 9.4⫾2.7 ⬍0.001 Plaque area, mm2 6.0⫾2.8 7.5⫾2.8 4.8⫾2.1 ⬍0.001 MLA site
Lumen area, mm2 2.0⫾1.1 2.0⫾1.1 2.1⫾1.1 0.753 Vessel area, mm2 10.7⫾3.7 12.7⫾3.7 8.8⫾2.5 ⬍0.001 Plaque area, mm2 8.7⫾3.5 10.7⫾3.6 6.7⫾2.3 ⬍0.001 Remodeling ratio 0.96⫾0.16 0.94⫾0.15 0.97⫾0.17 0.529 Values are expressed as n (%) or mean⫾SD.
*Type A vs type B.
MLA indicates minimum lumen area.
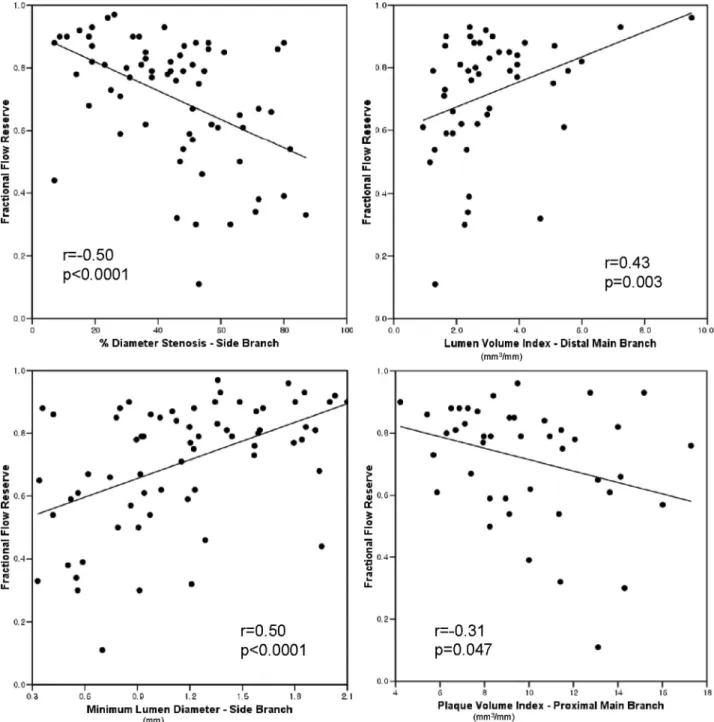
Among preintervention angiographic and IVUS parameters, SB minimal lumen diameter (r⫽0.50, P⬍0.0001), SB percent stenosis (r⫽⫺0.50, P⬍0.0001), lumen volume index of the distal MB (r⫽0.43, P⫽0.003), and plaque volume index of the
proximal MB (r⫽⫺0.31, P⫽0.047) were correlated with SB FFR (Figure 2). When preintervention angiographic and IVUS parameters were compared, functionally signif- icant lesions had more severe SB lesion (% diameter stenosis 54⫾20% versus 37⫾18%, P⬍0.0001), more fre- quent type B lesion (56% versus 44%, P⫽0.04), less lumen volume index at the distal MB (2.3⫾1.1 versus 3.6⫾1.8 mm3/mm, P⫽0.01), and more plaque burden at the MB (proximal MB, 80⫾8% versus 73⫾10%, P⫽0.03, distal MB, 73⫾10% versus 61⫾12%, P⫽0.002; Table 4). Binary logistic-regression analy- sis revealed that preintervention percent diameter stenosis of the SB (odds ratio⫽1.05; 95% CI, 1.01 to 1.09) and a type B lesion (odds ratio⫽3.86; 95% CI, 1.03 to 14.43) were independent angiographic predictors of functionally significant SB jailing (Table 5).
Table 3. Changes in IVUS Volume Indices (mm3/mm) After Stent Implantation
Proximal Segment P
Distal Segment
P
Pre Post Pre Post
LVI 4.0⫾2.0 6.7⫾2.0 ⬍0.0001 3.5⫾1.5 6.1⫾2.1 ⬍0.0001 PVI 9.1⫾3.0 8.4⫾2.4 0.001 5.4⫾1.8 5.3⫾1.7 0.227 VVI 13.2⫾3.6 15.1⫾3.5 ⬍0.0001 9.0⫾2.5 11.3⫾3.1 ⬍0.0001
LVI indicates lumen volume index; PVI, plaque volume index; VVI, vessel volume index.
Figure 2. Correlation between FFR of jailed SB lesion and preintervention angiographic and IVUS parameters.
When poststenting parameters were evaluated, the post- stent SB minimal lumen diameter (r⫽0.65, P⬍0.0001) and the poststent SB percent diameter stenosis (r⫽⫺0.62, P⬍0.0001) were correlated with SB FFR. Neither vessel volume index change in the distal MB (r⫽⫺0.17, P⫽0.27) nor plaque volume index change in the proximal MB (r⫽0.07, P⫽0.67) was correlated with SB FFR.
Among the SB lesions with ⱖ75% diameter stenosis, lesions with functionally significant stenosis (n⫽18) had greater SB poststent percent diameter stenosis (79.6⫾3.3%
versus 87.4⫾10.7%, P⫽0.008) and smaller minimal lumen diameter (0.45⫾0.07 versus 0.26⫾0.22 mm, P⫽0.002) than those with functionally insignificant stenosis (n⫽15). How- ever, after exclusion of 7 patients with slow flow (Thrombol- ysis In Myocardial Infarction grade ⱕ1), no differences in poststent angiographic parameters were found between the 2 groups. Furthermore, no difference was found in the amount of change in SB stenosis after stenting (poststent % diameter stenosis⫺prestent % diameter stenosis) and that in vessel volume index of the distal MB and plaque volume index of the proximal MB.
Discussion
The first aim of this study was to define the mechanism of SB jailing by IVUS. However, regardless of the mechanism, what is clinically relevant is whether the lesion has functional
significance or not. Therefore, we added physiological eval- uation as a second part of this study.
Mechanism of Geometric Changes After MB Stent Implantation
A recent angiographic study suggested that the main mecha- nism for the aggravation of an SB ostial stenosis after MB stenting is an alteration in the geometry of the carina (carina shift).5However, the degree of carina shift can be influenced by the response of the plaque in the distal MB to stent deployment. Previous IVUS studies have shown that lumen enlargement after stenting results from movement of plaque and vessel enlargement in nonbifurcation lesions.13–15
In our study, plaque volume index of the distal MB did not change after stent implantation. This result suggests that the lumen increase in the distal MB is primarily due to enlarge- ment of the vessel and not plaque shift, supporting the concept that the degree of luminal narrowing of an SB after stenting the MB is a result of carina shift. However, in the proximal MB, plaque area changed significantly after stent implantation, particularly in the region closest to the ostium of the SB. Although, plaque shift to the SB ostium was not observed directly, our results provide indirect evidence of plaque shift from the proximal segment of the MB into the SB ostium after MB stent implantation. Previous IVUS studies revealed that a longitudinal plaque redistribution, especially to a distal segment, is the main component of plaque area change after stent implantation.13–15 On the basis of these results, SB jailing can occur both by carina shift and plaque shift. The different response of the plaque according to its location may be due to the differences in plaque character and the pattern of plaque distribution and remodeling.8,16 –19
Anatomy Versus Functional Significance
In addition to an artifact by overlapping stent struts, SB ostial lesions have unique characteristics. SB ostial lesions are usually eccentric owing to the uneven distribution of shear stress.20,21 Furthermore, because carina shifting results in a single directional compression of the SB ostium, this phe- nomenon makes the stenosis even more eccentric (Figure 3).
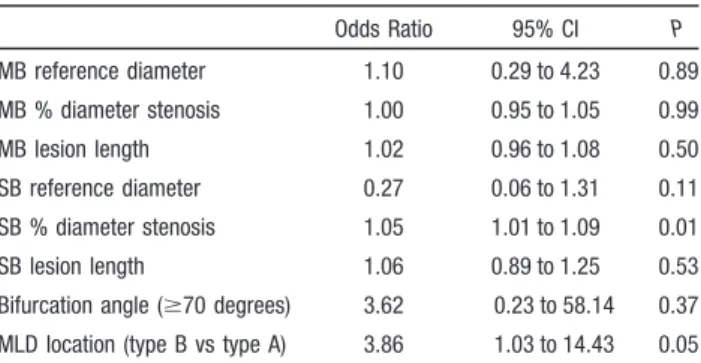
As the SB ostial stenosis cannot be evaluated by 2 true orthogonal angiographic views due to an overlap with the MB, angiographic minimal lumen diameter of an eccentric Table 5. Preinterventional Angiographic Predictors of
Functionally Significant SB Stenosis After MB Stent Implantation
Odds Ratio 95% CI P
MB reference diameter 1.10 0.29 to 4.23 0.89 MB % diameter stenosis 1.00 0.95 to 1.05 0.99
MB lesion length 1.02 0.96 to 1.08 0.50
SB reference diameter 0.27 0.06 to 1.31 0.11 SB % diameter stenosis 1.05 1.01 to 1.09 0.01
SB lesion length 1.06 0.89 to 1.25 0.53
Bifurcation angle (ⱖ70 degrees) 3.62 0.23 to 58.14 0.37 MLD location (type B vs type A) 3.86 1.03 to 14.43 0.05
MLD indicates minimum lumen diameter.
Table 4. Comparison of Preintervention Angiographic and IVUS Parameters Between Functionally Significant and Nonsignificant Jailed SBs
Angiographic Parameters
FFR⬍0.75 (N⫽28)
FFRⱖ0.75
(N⫽39) P
Main branch
Reference diameter, mm 3.0⫾0.6 3.0⫾0.4 1 Minimal lumen diameter, mm 1.0⫾0.4 1.2⫾0.4 0.15
% diameter stenosis 65⫾13 61⫾14 0.27
Side branch
Reference diameter, mm 2.1⫾0.5 2.2⫾0.4 0.33 Minimal lumen diameter, mm 0.9⫾0.4 1.4⫾0.4 ⬍0.001
% diameter stenosis 54⫾20 37⫾18 ⬍0.001
Type B lesion 19 (56) 15 (44) 0.04
Bifurcation angle, degrees 44⫾19 46⫾11 0.62 IVUS parameters
FFR⬍0.75 (N⫽22)
FFRⱖ0.75
(N⫽30) P
Proximal MB
Lumen volume index, mm3/mm 2.6⫾1.1 3.4⫾1.5 0.08 Vessel volume index, mm3/mm 13.2⫾3.5 12.7⫾3.5 0.67 Plaque volume index, mm3/mm 10.6⫾3.1 9.4⫾3.1 0.21
Plaque burden, % 80⫾8 73⫾10 0.03
Distal MB
Lumen volume index, mm3/mm 2.3⫾1.1 3.6⫾1.8 0.01 Vessel volume index, mm3/mm 8.3⫾2.0 9.4⫾2.7 0.14 Plaque volume index, mm3/mm 6.0⫾1.5 5.8⫾2.0 0.69
Plaque burden, % 73⫾10 61⫾12 0.002
SB ostial lesion usually underestimates the true lumen area.
In our study, the angiographic determinants of a functionally significant SB lesion were the preintervention SB percent diameter stenosis and the presence of a type B lesion, reflecting the degree of underlying disease and carina shift, respectively. SB FFR was correlated with the parameters representing underlying SB disease (SB minimal lumen diameter and SB % stenosis), carina shift (lumen volume index of the distal MB), and plaque shift (plaque volume index of the proximal MB, plaque burden in the MB).
However, the degree of underestimation of the SB lumen area can be different in each case, according to the relative contribution of each component (amount and location of underlying plaque, degree of remodeling, bifurcation angle, and the extent of plaque and carina shift) on luminal narrow- ing of the SB. Indeed, after exclusion of the lesions with slow flow, no difference in poststent angiographic parameters was found between functionally significant and nonsignificant SB lesions in patients with angiographically tight SB stenoses.
Limitations
There are several limitations to our study. The sample size is relatively small, and both IVUS and FFR evaluations were not available in all patients. IVUS of the SB after MB stenting was not performed, thus limiting our evaluation of the anatomic changes in the SB ostium. However, it is difficult to perform IVUS of the SB and obtain adequate images through undilated struts. It is not clear from this study that the clinical outcome of the ostial SB lesion, whether or not functionally significant, is correlated with IVUS findings. QCA was not performed with a dedicated bifurcation analysis system.
Compared with a previous study,6the proportion of function- ally significant stenoses in patients with angiographically tight stenoses was larger in this study. The difference may reflect the difficulty in assessing the SB ostial stenosis by QCA. The SB ostium after MB stenting is generally small and frequently overlaps the MB. Manual correction to accurately detect the edge is subject to interindividual variability.
However, it is not known whether the angiographic parame- ters measured by a dedicated bifurcation QCA system are
correlated better with the functional significance of jailed SB lesions. Some patients underwent predilation before the IVUS, and in a small number of patients a different IVUS system was used. However, analyzing the data without these patients included did not affect the results. Finally, the SB lesions included in this study were relatively short ostial lesions; therefore, the results cannot be directly applied to diffuse or multiple SB lesions.
In conclusion, aggravation of SB luminal narrowing after MB stent implantation results from both plaque shift and carina shift. However, it is difficult to predict the functional significance of each jailed SB lesion on the basis of anatomic characteristics owing to the complex mechanism of luminal narrowing and its individual variability.
Sources of Funding
This work was supported by grants from CardioVascular Research Foundation, Korea (CVRF), the Innovative Research Institute for Cell Therapy (IRICT: A062260), and the Korea Health 21 R&D Project (0412-CR02-0704-0001), Ministry of Health & Welfare, South Korea.
Disclosures
None.
References
1. Stary HC. Evolution and progression of atherosclerotic lesions in coronary arteries of children and young adults. Arteriosclerosis. 1989;9:
I-19 –I-32.
2. Al Suwaidi J, Berger PB, Rihal CS, Garratt KN, Bell MR, Ting HH, Bresnahan JF, Grill DE, Holmes DR Jr. Immediate and long-term outcome of intracoronary stent implantation for true bifurcation lesions.
J Am Coll Cardiol. 2000;35:929 –936.
3. Colombo A, Moses JW, Morice MC, Ludwig J, Holmes DR Jr, Spanos V, Louvard Y, Desmedt B, Di Mario C, Leon MB. Randomized study to evaluate sirolimus-eluting stents implanted at coronary bifurcation lesions. Circulation. 2004;109:1244 –1249.
4. Sheiban I, Albiero R, Marsico F, Dharmadhikari A, Tzifos V, Pagnotta P, Montorfano M, Leonardo F, Saba P, Di Mario C, Colombo A. Immediate and long-term results of “T” stenting for bifurcation coronary lesions.
Am J Cardiol. 2000;85:1141–1144.
5. Vassilev D, Gil R. Relative dependence of diameters of branches in coronary bifurcations after stent implantation in main vessel–importance of carina position. Kardiol Pol. 2008;66:371–378.
Figure 3. Angiographic and IVUS find- ings of carina shift. This figure shows the angiogram (left), cross-sectional IVUS image at the level of the carina (middle), and longitudinal IVUS image (right) before (upper panels) and after (lower panels) MB stent implantation. After stent implantation, the carina (white arrow) is shifted to the SB side, and this shift results in the eccentric luminal nar- rowing of the SB ostium. Minimal lumen diameter of the SB was 0.54 mm and 0.6 mm by QCA and IVUS measurement, respectively. FFR of the jailed SB was 0.87. White line in the SB of preinterven- tion longitudinal image is a 0.014-in. cor- onary wire (*).
6. Koo BK, Kang HJ, Youn TJ, Chae IH, Choi DJ, Kim HS, Sohn DW, Oh BH, Lee MM, Park YB, Choi YS, Tahk SJ. Physiologic assessment of jailed side branch lesions using fractional flow reserve. J Am Coll Cardiol. 2005;46:633– 637.
7. Koo BK, Park KW, Kang HJ, Cho YS, Chung WY, Youn TJ, Chae IH, Choi DJ, Tahk SJ, Oh BH, Park YB, Kim HS. Physiological evaluation of the provisional side-branch intervention strategy for bifurcation lesions using fractional flow reserve. Eur Heart J. 2008;29:726 –732.
8. Shimada Y, Courtney BK, Nakamura M, Hongo Y, Sonoda S, Hassan AH, Yock PG, Honda Y, Fitzgerald PJ. Intravascular ultrasonic analysis of atherosclerotic vessel remodeling and plaque distribution of stenotic left anterior descending coronary arterial bifurcation lesions upstream and downstream of the side branch. Am J Cardiol. 2006;98:193–196.
9. Badak O, Schoenhagen P, Tsunoda T, Magyar WA, Coughlin J, Kapadia S, Nissen SE, Tuzcu EM. Characteristics of atherosclerotic plaque dis- tribution in coronary artery bifurcations: an intravascular ultrasound anal- ysis. Coron Artery Dis. 2003;14:309 –316.
10. Kataoka T, Grube E, Honda Y, Morino Y, Hur SH, Bonneau HN, Colombo A, Di Mario C, Guagliumi G, Hauptmann KE, Pitney MR, Lansky AJ, Stertzer SH, Yock PG, Fitzgerald PJ. 7-Hexanoyltaxol- eluting stent for prevention of neointimal growth: an intravascular ultrasound analysis from the Study to COmpare REstenosis rate between QueST and QuaDS-QP2 (SCORE). Circulation. 2002;106:1788 –1793.
11. Nakamura M, Yock PG, Bonneau HN, Kitamura K, Aizawa T, Tamai H, Fitzgerald PJ, Honda Y. Impact of peri-stent remodeling on restenosis: a volumetric intravascular ultrasound study. Circulation. 2001;103:
2130 –2132.
12. Serruys PW, Degertekin M, Tanabe K, Russell ME, Guagliumi G, Webb J, Hamburger J, Rutsch W, Kaiser C, Whitbourn R, Camenzind E, Meredith I, Reeves F, Nienaber C, Benit E, Disco C, Koglin J, Colombo A. Vascular responses at proximal and distal edges of paclitaxel-eluting stents: serial intravascular ultrasound analysis from the TAXUS II trial.
Circulation. 2004;109:627– 633.
13. Ahmed JM, Mintz GS, Weissman NJ, Lansky AJ, Pichard AD, Satler LF, Kent KM. Mechanism of lumen enlargement during intracoronary stent
implantation: an intravascular ultrasound study. Circulation. 2000;
102:7–10.
14. Maehara A, Takagi A, Okura H, Hassan AH, Bonneau HN, Honda Y, Yock PG, Fitzgerald PJ. Longitudinal plaque redistribution during stent expansion. Am J Cardiol. 2000;86:1069 –1072.
15. von Birgelen C, Mintz GS, Bose D, Baumgart D, Haude M, Wieneke H, Neumann T, Brinkhoff J, Jasper M, Erbel R. Impact of moderate lesion calcium on mechanisms of coronary stenting as assessed with three- dimensional intravascular ultrasound in vivo. Am J Cardiol. 2003;
92:5–10.
16. Baptista J, di Mario C, Ozaki Y, Escaned J, Gil R, de Feyter P, Roelandt JR, Serruys PW. Impact of plaque morphology and composition on the mechanisms of lumen enlargement using intracoronary ultrasound and quantitative angiography after balloon angioplasty. Am J Cardiol. 1996;
77:115–121.
17. Finet G, Weissman NJ, Mintz GS, Satler LF, Kent KM, Laird JR, Adelmann GA, Ajani AE, Castagna MT, Rioufol G, Pichard AD.
Mechanism of lumen enlargement with direct stenting versus predila- tation stenting: influence of remodelling and plaque characteristics assessed by volumetric intracoronary ultrasound. Heart. 2003;89:84 –90.
18. Fujii K, Carlier SG, Mintz GS, Wijns W, Colombo A, Bose D, Erbel R, de Ribamar Costa J Jr, Kimura M, Sano K, Costa RA, Lui J, Stone GW, Moses JW, Leon MB. Association of plaque characterization by intra- vascular ultrasound virtual histology and arterial remodeling. Am J Cardiol. 2005;96:1476 –1483.
19. Rodriguez-Granillo GA, Serruys PW, Garcia-Garcia HM, Aoki J, Val- gimigli M, van Mieghem CA, McFadden E, de Jaegere PP, de Feyter P.
Coronary artery remodelling is related to plaque composition. Heart.
2006;92:388 –391.
20. Kimura BJ, Russo RJ, Bhargava V, McDaniel MB, Peterson KL, DeMaria AN. Atheroma morphology and distribution in proximal left anterior descending coronary artery: in vivo observations. J Am Coll Cardiol. 1996;27:825– 831.
21. Malek AM, Alper SL, Izumo S. Hemodynamic shear stress and its role in atherosclerosis. J Am Med Assoc. 1999;282:2035–2042.
CLINICAL PERSPECTIVE
To develop improved strategies and devices for coronary bifurcation lesions, better insight into both the anatomic and functional aspects of bifurcation lesions is required. We sought to investigate the mechanism of geometric changes after MB stent implantation and to identify the predictors of functionally significant jailed SB lesions with both IVUS and FFR.
IVUS analyses showed that SB jailing can occur both by carina shift and plaque shift. Angiographic determinants of a functionally significant SB lesion were the preintervention SB percent diameter stenosis and the MB minimum lumen diameter located distal to the SB ostium, reflecting the degree of underlying disease and carina shift, respectively.
However, it was difficult to predict the functional significance of each jailed SB lesion. This study showed the complex mechanism of SB jailing and its individual variability, which explains the difficulty of angiographic assessment in evaluating the functional significance of a jailed SB.
William F. Fearon
Choi, Takao Hasegawa, Toru Kataoka, Sung Jin Oh, Yasuhiro Honda, Peter J. Fitzgerald and Gwon, Myeong-Ho Yoon, Seung-Jea Tahk, Woo-Young Chung, Young-Seok Cho, Dong-Ju Seung-Ho Hur, Jung-Sun Kim, Donghoon Choi, Yangsoo Jang, Joo-Yong Hahn, Hyeon-Cheol
Bon-Kwon Koo, Katsuhisa Waseda, Hyun-Jae Kang, Hyo-Soo Kim, Chang-Wook Nam,
Print ISSN: 1941-7640. Online ISSN: 1941-7632
Copyright © 2010 American Heart Association, Inc. All rights reserved.
Avenue, Dallas, TX 75231
is published by the American Heart Association, 7272 Greenville Circulation: Cardiovascular Interventions
doi: 10.1161/CIRCINTERVENTIONS.109.887406 2010;3:113-119 Circ Cardiovasc Interv.
http://circinterventions.ahajournals.org/content/3/2/113
World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://circinterventions.ahajournals.org//subscriptions/
is online at:
Circulation: Cardiovascular Interventions Information about subscribing to
Subscriptions:
http://www.lww.com/reprints
Information about reprints can be found online at:
Reprints:
document.
Answer
Permissions and Rights Question and under Services. Further information about this process is available in the
permission is being requested is located, click Request Permissions in the middle column of the Web page Clearance Center, not the Editorial Office. Once the online version of the published article for which
can be obtained via RightsLink, a service of the Copyright Circulation: Cardiovascular Interventions
in
Requests for permissions to reproduce figures, tables, or portions of articles originally published Permissions: