서론
, ,
, ,
1). 1988 Reaven
2) , ,
“X ”
. “ ”,
“Deadly Quarter”
중풍환자의 대사증후군 유병률에 대한 단면조사연구
박성욱, 이인환, 정우상, 문상관, 박정미, 고창남, 조기호, 김영석, 배형섭
경희대학교 한의과대학 심계내과학교실
Cross-sectional Study on Prevalence of Metabolic Syndrome in Stroke Patients
Seong-Uk Park, In-Whan Lee, Woo-Sang Jung, Sang-Kwan Moon, Jung-Mi Park, Chang-Nam Ko, Ki-Ho Cho, Young-Suk Kim, Hyung-Sup Bae
Department of Cardiovascular & Neurologic Diseases (Stroke Center), College of Oriental Medicine, Kyung-Hee University, Seoul, Korea.
Objectives : Metabolic syndrome (MetS) is associated with increasing risk of cardiovascular morbidity and mortality but the risk of stroke associated with the MetS is less well established. The objective of this study was to evaluate the prevalence of MetS in stroke patients.
Methods : We analyzed the data of 806 patients with acute ischemic stroke from Hanbang Stroke Registry supported by the Ministry of Science and Technology of Korea. Subjects' enrollment was done in the oriental medical hospitals of 4 universities located in the metropolitan region from April 2007 to August 2008. We analyzed all registered data and evaluated the prevalence of MetS and specific components of MetS.
Results : The prevalence of MetS in stroke patients according to American Heart Association/National Heart Lung and Blood Institute (AHA/NHLBI) criteria was 59.6%. The prevalence according to the International Diabetes Federation (IDF) criteria was 41.6%. The prevalence of female patients was higher than that of male patients (71.8%
vs 51% by AHA/NHLBI criteria; 61.7% vs 27.7% by IDF criteria). The prevalence of central obesity, low HDL cholesterol and hypertension was higher in female patients. There was no significant relationship between MetS and stroke subtype.
Conclusions : This work gives us the basic data on the association between MetS and risk of stroke. There should be the prospective cohort studies to evaluate MetS and the risk of stroke.
Key Words : Metabolic syndrome (MetS), Stroke, epidemiology
1998 (WHO)
3), 2001 NCEP ATP III
4).
National Health and Nutrition Exam- ination Survey III 4,700
5), 24.1%-41%
6-8,22)
. , ,
1.4 4.5
9-12)
.
2.1-2.5 13,14),
15-16)
.
,
.
4
.
연구방법
1. 연구대상
2007 4 1 2008 8 31
2 ,
,
(Brain-CT) (Brain MR)
4 .
2. 조사항목
(1) Large Artery Atherosclerosis (LAA) (2) Cardioembolism (CE)
(3) Small Vessel Occlusion (SVO)
(4) Stroke of other determined etiology (SOE) (5) Stroke of Undetermined etiology (SUE)
3. 대사증후군 진단기준
2001 National Cholesterol Education Program Adult Treatment Panel III(NECP-ATP )
4) 2005 American Heart Association/
National Heart Lung and Blood Institute(AHA/NHLBI)
19) 2005 (International Diabetes Federation, IDF)
20) .
2000 WHO West Pacific Region Inter- national Obesity Task Force -
(Asia-Pacific Criteria, APC)
90cm, 80 cm 21).
5 3
: 90cm, 80cm
: 150mg/dL
:
< 40mg/ dL, < 50mg/dL
: 130mmHg
85mmHg
: 100mg/dL
90cm, 80cm
4 2
: 150mg/dL
:
< 40mg/ dL, < 50mg/dL
: 130mmHg
85mmHg
: 100mg/dL
4. 통계방법
SPSS(Statistical Program for Social Science) 13.0 for Window ,
Student t-test, Chi-square test
. P-value 0.05
.
연구결과
1. 연구대상자들의 일반적인 특징
2007 4 1 2008 8 31
806 .
502
. 502
296 , 206 66.0±24.9
.
, . 85.6±11.0cm,
111.3±36.4 mg/dL
40.3±14.6 mg/dL 140.9±107.2 mg/dL (Table 1).
2. 대사증후군 및 대사증후군의 각 구성요소별 유병률
AHA/NHLBI
59.6% , 71.8% 51%
. IDF
AHA/NHLBI
41.6% ,
61.7% 27.7%
. 76.3%
(67.5
Prevalence
Overall, n=502 Men, n=296 Women, n=206 Sociodemographic Characteristics
Mean Age, yr 66.0±24.9 63.3±12.3 69.9±35.7*
Men, % 59
Married, % 75.7 85.5 63.8*
Religion, % 56.8 50.7 66.3*
Education, yr 8.5±4.5 9.9±4.4 6.5±4.0*
Vascular risk factors
History of hypertension, % 65.3 60.9 73.0*
History of diabetes, % 29.5 29.3 30.2
History of hyperlipidemia, % 17.7 16.3 20.2
History of arrhythmia, % 6.2 5.5 7.7
History of IHD, % 8 5.1 12.3*
Current smoking, % 24.9 38.4 5.9*
Alcohol intake, % 29.5 45.4 6.8*
Waist circumference, cm 85.6±11.0 86.1±11.7 84.9±9.9
Body mass index, kg/m2 23.8±4.1 24.1±4.7 23.5±3.0
Waist/Hip ratio 0.94±0.1 0.95±0.11 0.92±0.08*
Fasting glucose, mg/dL 111.3±36.4 108.6±33.4 115.3±40.1*
HDL-cholesterol, mg/dL 40.3±14.6 39.7±15.7 41.2±12.8
Triglyceride, mg/dL 140.9±107.2 145.1±121.3 134.8±82.7
IHD: ischemic heart disease,
*: P<0.05 between men and women
Table 1. Baseline Sociodemographic Characteristics and Vascular Risk Factors of the Patients
Prevalence Overall,
n=502
Men, n=296
Women, n=206
WC, % (woman, 80cm; man, 90cm) 50.6 36.1 71.4*
TG, % 150mg/dL 32.5 33.4 31.1
HDL, % (woman, <50mg/dL; man, <40mg/dL) 67.5 58.1 81.1*
FBS 100mg/dL or being treated for DM, % 58.4 57.1 60.2
Hypertension, % 76.3 70.6 84.5*
Metabolic syndrome by AHA/NHLBI criteria, % 59.6 51.0 71.8*
Metabolic syndrome by IDF criteria, % 41.6 27.7 61.7*
MetS: metabolic syndrome, WC: Waist circumference, TG: Triglyceride, HDL: HDL-cholesterol, FBS: Fasting blood glucose, AHA/NHLBI:
American Heart Association/National Heart, Lung, and Blood Institute, IDF: International Diabetes Federation Hypertension: systolic 130mmHg or diastolic 85mmHg or being treated for hypertension
*: P<0.05 between men and women
Table 2. Prevalence of the MetS and Specific Components
%), (58.4%), (50.6%),
(32.5%) .
(36.1% vs 71.4%),
(58.1% vs 81.1%), (70.6% vs 84.5%) (Table 2).
3. 중풍의 아형분류와 대사증후군의 유병률
502
498 ,
.
498 460 (92.4%)
, 37 ,
1 . 457
TOAST Large Artery Atherosclerosis (LAA) 106 , Cardioembolism (CE) 36 , Small Vessel Occlusion (SVO) 311 , Stroke of other determined etiology (SOE) 2 , Stroke of Undete-
rmined etiology (SUE) 2 SVO
68.1%
.
(Table 4).
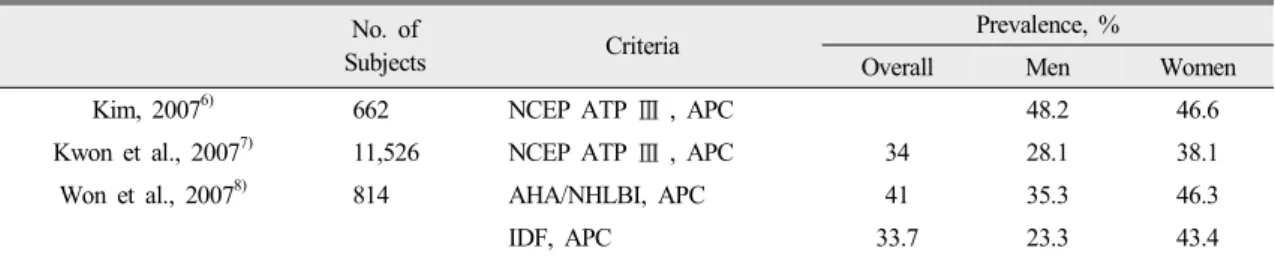
No. of
Subjects Criteria Prevalence, %
Overall Men Women
Kim, 20076) 662 NCEP ATP , APC 48.2 46.6
Kwon et al., 20077) 11,526 NCEP ATP , APC 34 28.1 38.1
Won et al., 20078) 814 AHA/NHLBI, APC 41 35.3 46.3
IDF, APC 33.7 23.3 43.4
MetS: metabolic syndrome, NCEP ATP: National Cholesterol Education Program Adult Treatment Panel, APC: Asia-Pacific Criteria, AHA/NHLBI: American Heart Association/National Heart, Lung, and Blood Institute, IDF: International Diabetes Federation Table 3. Previous Prevalence Studies on the MetS among Korean Population
Prevalence
Overall, n=498 With MetS, n=301 Without MetS, n=197 Stroke subtype
ICH, % 7.4 5.6 10.2
SAH, % 0.2 0.3 0.0
CI, % 92.4 94.0 89.8
Overall, n=457 With MetS, n=281
Without MetS, n=176 TOAST (in CI)
LAA, % 23.2 24.2 21.6
CE, % 7.9 8.2 7.4
SVO, % 68.1 66.9 69.9
SOE, % 0.4 0.4 0.6
SUE, % 0.4 0.4 0.6
MetS: metabolic syndrome, CI: cerebral infarction, LAA: Large Artery Atherosclerosis, CE: Cardioembolism, SVO: Small Vessel Occlusion, SOE: Stroke of other determined etiology, SUE: Stroke of Undetermined etiology
*: P<0.05 between men and women
Table 4. Prevalence of the MetS according to Stroke Subtype
고찰
,
, 1998 2001 ,
1998 22.5% 2001 24.1%
22).
9-12)
,
13-16)
.
4
.
AHA/NHLBI 59.6%
.
24.1% 22),
7,8) (Table
3),
.
23) 2 151
NCEP ATP , APC
69.8%, IDF 50.9%
, 24)
2 71
IDF 42.3%
.
(AHA/NHLBI 71.8% vs 51%, IDF 61.7% vs 27.7%).
.
7) 40
(40 28.8%, 50 26.6%, 60 26.6%, 70
18.1%) , 50
(40 28.7%, 50 43.3%, 60 49.4%, 70 46.4%)
, 8)
6)
. 66.0±24.9
.
. 2000
WHO West Pacific Region International Obesity
Task Force -
90cm, 80 cm . IDF
102 cm,
88 cm, 94 cm, 80 cm ,
90 cm, 80cm ,
85 cm, 90 cm .
90
cm , 85 cm
25).
51.0%, 67.0% (AHA/NHLBI
) 43.7% 27.7%(IDF )
.
,
92.4% .
4:1 15-20%
,
26)
40%
.
7.6% ,
.
SVO 68.1%
.
,
,
.
,
.
참고문헌
1. Wilson PWF, Kannel WB, Silbershartz H, D'A- gostino RB: Clustering of metabolic factors and coronary heart disease. Arch Intern Med. 1999;
159:1104-9.
2. Reaven GM. Role of insulin resistance in human disease. Diabetes 1988;37(12):1595-607.
3. Alberti KG, Zimmet PZ: Definition, diagnosis and classification of diabetes mellitus and its complications. Part 1. Diagnosis and classification of diabetes mellitus provisional report of a WHO consultation. Diabet. Med. 1998;15:539-53.
4. Executive summary of the third report of the
National Cholesterol Education Program (NCEP) expert panel on detection, evaluation, and treat- ment of high blood cholesterol in adults (Adult Treatment Panel III). JAMA 2001;285:2486-97.
5. Ford ES, Giles WH, Dietz WH. Prevalence of the metabolic syndrome among us adults: findi- ngs from the third National Health and Nutrition Examination Survey. JAMA. 2002;287:356-59.
6. . ;
: (HAS).
2007;8(4):369-71.
7. , , , , ,
, , .
; ,
. 2007;8(4):353-5.
8. , , , , ,
, , , , .
National Cholesterol Education Program International Diabetes Federation
. 2007;31(3):284-292.
9. Hanley AJ, Karter AJ, Williams K, Festa A, D'Agostino RB Jr, Wagenknecht LE, affner SM: Prediction of type 2 diabetes mellitus with alternative definitions of the metabolic syndrome:
the Insulin Resistance Atherosclerosis Study.
Circulation 2005;13;112:3713-21.
10. Hsia J, Bittner V, Tripputi M, Howard BV.
Metabolic syndrome and coronary angiographic disease progression: the women’ angiographic vitamin and estrogen trial. Am Heart J. 2003;
146:439-45.
11. Lakka H, Laaksonen D, Lakka T, Niskanen L, Kumpusalo E, Tuomilehto J, Salonen J. The metabolic syndrome and total and cardiovascular disease mortality in middle-aged men. JAMA.
2002;288:2709-716.
12. Malik S, Wong ND, Franklin S, Kamath TV,
L’talian G, Pio JR, Williams GR. Impact of metabolic syndrome on mortality from coronary artery heart disease, cardiovascular disease, and all causes in United States adults. Circulation.
2004;110:1245-250.
13. Koren-Morag N, Goldbourt U, Tanne D. Relation between the metabolic syndrome and ischemic stroke or transient ischemic attack: a prospective cohort study in patients with atherosclerotic cardiovascular disease. Stroke 2005;36:1366-71.
14. Kurl S, Laukkanen JA, Niskanen L, Laaksonen D, Sivenius J, Nyyssonen K, Salonen JT: Meta- bolic syndrome and the risk of stroke in middle -aged men. Stroke 2006;37:806-11.
15. Sone H, Mizuno S, Fujii H, Yoshimura Y, Yamasaki Y, Ishibashi S, Katayama S, Saito Y, Ito H, Ohashi Y, Akanuma Y, Yamada N: Is the diagnosis of metabolic syndrome useful for predicting cardiovascular disease in Asian diabetic patients? Analysis from the Japan Diabetes Complications Study. Diabetes Care 2005;28:1463 -71.
16. McNeill AM, Rosamond WD, Girman CJ, Golden SH, Schmidt MI, East HE, Ballantyne CM, Heiss G: The Metabolic syndrome and 11-year risk of incident cardiovascular disease in the Atherosclerosis Risk in Communities Study. Diabetes Care 2005;28:385-90.
17. Adams HP Jr, Bendixen BH, Kappelle LJ. Cla- ssification of subtype of acute ischemic stroke.
Definitions for use in a multicenter clinical trial.
TOAST. Trial of Org 10172 in Acute Stroke Treatment. Stroke 1993;24(1):35-41.
18. Gordon DL, Bendixen BH, Adams HP Jr, Clarke W, Kappelle LJ, Woolson RF. Interphysicain
agreement in the diagnosis of subtypes of acute ischemic stroke: implications for clinical trials.
The TOAST Investigators. Neurology 1993;43 (5):1021-27.
19. Grundy SM: Metabolic syndrome scientific stat- ement by the American Heart Association and the National Heart, Lung, and Blood Institute.
Arterioscler Thromb Vasc Biol 2005;25:2243-4.
20. Alberti KG, Zimmet P, Shaw J: IDF Epidemiology Task Force Consensus Group: The metabolic syndrome- a new worldwide definition. Lancet 2005;366:1059-62.
21. Western Pacific Regional Office of the World Health Organization, The International Obesity Task Force. The Asia-Pacific perspective: redefining obesity and its treatment. 2000
22. Lim S, Park KS, Lee HK, Cho SI: Changes in the characteristics of metabolic syndrome in Korea over the period 1998-2001 as determined by Korean National Health and Nutrition Exami- nation Surveys. Diabetes Care 2005;28:1810-2.
23. , , . 2
(WHO, NCEP-ATP 3,
IDF) .
2008;32(2):157-164.
24. , , , , ,
. 2
. 2006;30
(6):442-9.
25. , , , , ,
.
. 2006;15(1):1-9.
26. , , , .
. 1999;28(4):
509-513.