Implant placement in severely atrophic mandible using alveolar ridge splitting procedure and small block bone graft: A case report of 4-year follow-up
10
0
0
전체 글
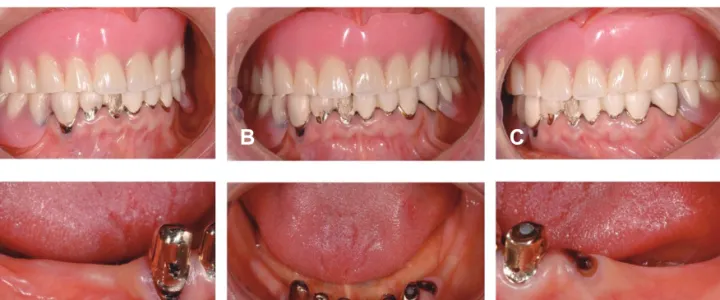
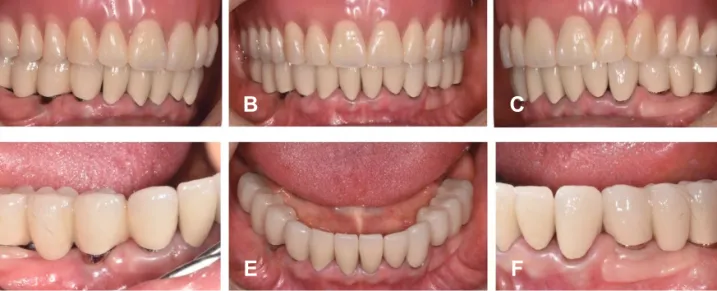
(2) 심하게 위축된 하악 구치부에 치조제 분할술과 블록형 골이식술을 이용한 임플란트 식립: 4년 관찰 증례보고. 65. alveolar bone maintenance, and protection of the adjacent teeth.4) However, the loss of teeth leads to absorption and atrophy of the alveolar bone.5,6) Due to the inevitable vertical and horizontal alveolar bone resorption, 26% of the total volume decreases in 1 year, whilst the width of the alveolar bone undergoes a volume reduction of 40-60% in 3 years. Morphological changes caused by such severe alveolar atrophy and resorption limit the successful placement of implants. Among various procedures of bone augmentation, alveolar ridge splitting has been reported to be a successful surgical method for increasing the narrow alveolar bone width.8) We report a case of 4 years following implant placement with ridge splitting and small autogenous bone graft in severly atrophic mandible.. Case Descriptions A 63-year-old female patient with poor mastication, frequent tongue and gingival soreness, and irritation caused by a mandibular denture visited the Department of Prosthodontics at the Veterans Health Service Medical Center to seek consultation regarding implants. Medical records confirmed a history of hypertensive drug use, while dental records showed a 3-year history of maxillary complete denture use and a 7-year history of mandibular double crown removable partial denture use.. A. B. C. D. E. F. Fig. 1. Clinical photos at the first visit. A. Lateral view of right side; B. Frontal view; C. Lateral view of left side; D. Lateral view of right posterior side; E. Occlusal view; F: Lateral view of left posterior side On intraoral examination, an asymmetric occlusal plane was detected. Fracture of facing was observed with mandibular double crown removable partial dentures. In addition, we noted secondary caries of the right mandibular canine, a coronal fracture in the left mandibular first premolar tooth, and severe atrophy in the bilateral mandibular molar area. (Fig. 1). Journal of the Korean Academy of Esthetic Dentistry.
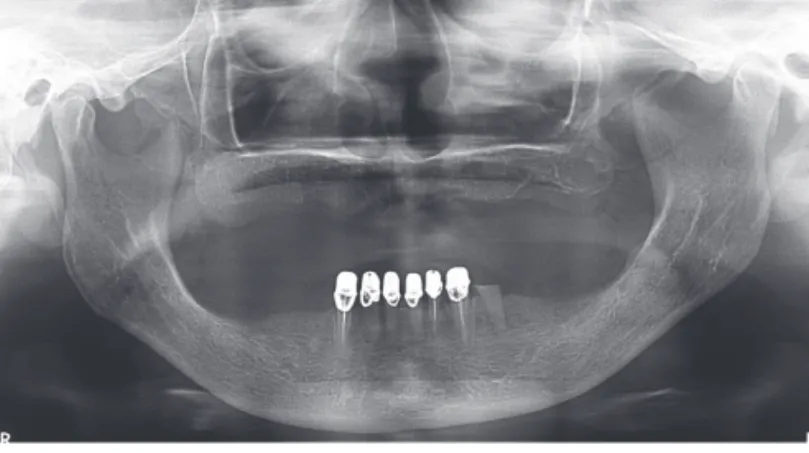
(3) 66. 2019, Vol. 28, Issue 2. Fig. 2. Panoramic radiographic at the first visit The initial treatment plan included reconstructing the maxillary denture to form a new occlusal plane; for the edentulous mandible, either an implant-assisted partial denture or an implant-supported prosthesis was considered. However, considering the patient´s discomfort with dentures and her financial situation, we decided to insert a complete maxillary denture and an implant-supported mandibular prosthesis. Accordingly, the anterior mandibular region was to be reconstructed, and a shortened dental arch (SDA) covering the first molar was planned for the severely atrophied posterior mandibular region. (Fig. 2). A. B. C. D. Fig. 3. Preoperative occlusal views of mandibular arch. A. Clinical photo; B. Cone beam computed tomograph showed severely atrophic mandibular ridge; C. Right posterior side; D. Left posterior side..
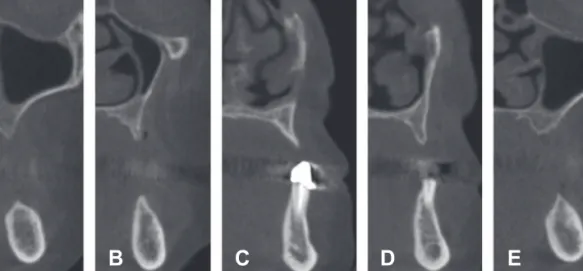
(4) 심하게 위축된 하악 구치부에 치조제 분할술과 블록형 골이식술을 이용한 임플란트 식립: 4년 관찰 증례보고. 67. Extraction of the crown-fractured left mandibular first premolar with immediate implant placement was planned. Severe alveolar resorption in the left mandibular first molar region was observed in the pre-operative cone-beam computed tomography (CBCT). (Fig. 3, 4) Consequently, an alveolar bone augmentation was planned. The right mandibular canine was hopelss due to severe caries, and thus, immediated implant placement was considered along with alveolar bone augmentation of the right posterior first molar.. A. B. C. D. E. Fig. 4. Preoperative cross-sectional views of mandibular arch. A. First molar area on right side; B. First premolar area on ridge side; C. Canine on right side; D. First premolar on left side; E. First molar area on left side.. Prior to surgery, the mouthwash was performed for 1 minute with chlorhexidine digluconate solution (Hexamedine Solution, Bukwang, Seoul, Korea), after which local anesthesia was applied to the surgical site using 2% lidocaine HCl and an epinephrine injection (Yuhan, Seoul, Korea) in the department of Periodontology. The mucoperiosteal flap was raised after making horizontal and vertical incisions. Internal tapered implants (OneQ, Dentis, Seoul, Korea) were placed in the mandibular left first premolar and right canine regions after extraction. Both of edentulous sites were subjected to severe resorption, with only less than 2 mm of residual alveolar ridge.. A. B. C. D. E. F. Fig. 5. Intraoperative clinical photos of left mandible. A. Flap reflection; B. Remained ridge < 2 mm; C. Immediated placement on premolar area and implant placement on molar area after ridge splitting; D. Mini-block bone fixation using one screw on molar area; E. Covering resorbable membrane after graft; F. Suturing Journal of the Korean Academy of Esthetic Dentistry.
(5) 68. 2019, Vol. 28, Issue 2. Corticotomy was performed using a piezo electric system (Surgybone®, Silfradent, Sofia, Italy) on the narrowed, lingual side of the alveolar crest. After alveolar splitting, the alveolar ridge was expanded using a tapered osteotome (Osteotome Palti, Stoma, Emminger, Germany) and a tapered expansion kit (ESSET®, Osstem, Seoul, Korea). All remaining implants were placed at the same time during alveolar ridge splitting. After alveolar ridge splitting, the buccal cortical bone was partially fractured in bilateral first molar region, exposing the implant thread. The left first molar area was posteriorly extended to the flap, and a small block-shaped autogenous bone measuring 10×6 mm was taken from the ramus, and a fixation using only one screw (Autoscrew, Jeil medical, Seoul, Korea) was conducted.9) (Fig. 5) The right first molar site was prepared by cortical bone fracture following alveolar ridge splitting. Similar to the right side, the fractured buccal plate was fixed with the screwe. After implantation, a xenograft (THE Graft, Purgo, Seoul, Korea) was placed in the space between the implant and alveolar ridge. Above this, an absorbent collagen barrier (Ossix®plus, Datum Dental Ltd, Telrad, Israel) was positioned. (Fig. 6). A. B. C. D. E. F. Fig. 6. Intraoperative clinical photos of right mandible. A. Flap reflection; B. Remained ridge < 2 mm; C. Ridge splitting using piezo electric device; D. Fixation the fractured buccal bone of molar area using screw; E. Covering resorbable membrane after graft; F. Suturing. After making the diagnostic cast via preliminary impressions, an occlusion rim was made, and the occlusal plane was set considering the Camper’s plane and inter-pupillary line; following calculation of the vertical height by considering the physiological stable position. Recoding centric relation was achieved by a bilateral manipulation. Subsequently, a temporary maxillary denture was made as per the general guidelines and seated in the oral cavity. For the mandibular region, extended temporary bridge was delivered. After 5 months, a second surgery was performed on each side. The left first premolar region, which was one of the immediate implant sites, showed mild resorption, but no additional bone graft was performed considering the shape of the surrounding bone; instead, biotype improvement using free gingival graft from the left palatal region was conducted to prevent additional resorption. In the posterior first molar region, bone regeneration was observed around the screw. (Fig. 7).
(6) 심하게 위축된 하악 구치부에 치조제 분할술과 블록형 골이식술을 이용한 임플란트 식립: 4년 관찰 증례보고. A. B. 69. C. Fig. 7. Clinical photos of left mandible. A. lateral view at uncovering surgery; B. Free gingival graft after connection of healing abutments; C. 6 weeks postoperative lateral view Following this, a fixed temporary restoration was fabricated for the mandibular implants. Using a self-polymerizing acrylic (Trayplast NF, Vertex Dental, Zeist, Netherlands), an individual tray was made; using additional polymerization type silicone impression material (Imprint II Regular body, 3M, St. Paul, MN, USA), impressions were made at the fixture level, and a working cast was made. After the occlusion rim was made from the working cast, the interarch relation was determined using the temporary denture of the maxilla and the mandibular anterior teeth . Implant abutments were made by cutting off the ready-made abutments; Cement-retained temporary prosthesis were made and regularly evaluated via occlusal adjustment. After using the temporary prosthesis of the maxilla and mandible for 2 months, the patient showed no signs of discomfort; therefore, the final prosthesis was placed. (Fig. 8, 9, 10). A. B. C. D. E. F. Fig. 8. Clinical photos of 8 weeks after delivering final prosthesis. A. Lateral view of right side; B. Frontal view; C. Lateral view of left side; D. Lateral view of right posterior side; E. Occlusal view; F: Lateral view of left posterior side.. Journal of the Korean Academy of Esthetic Dentistry.
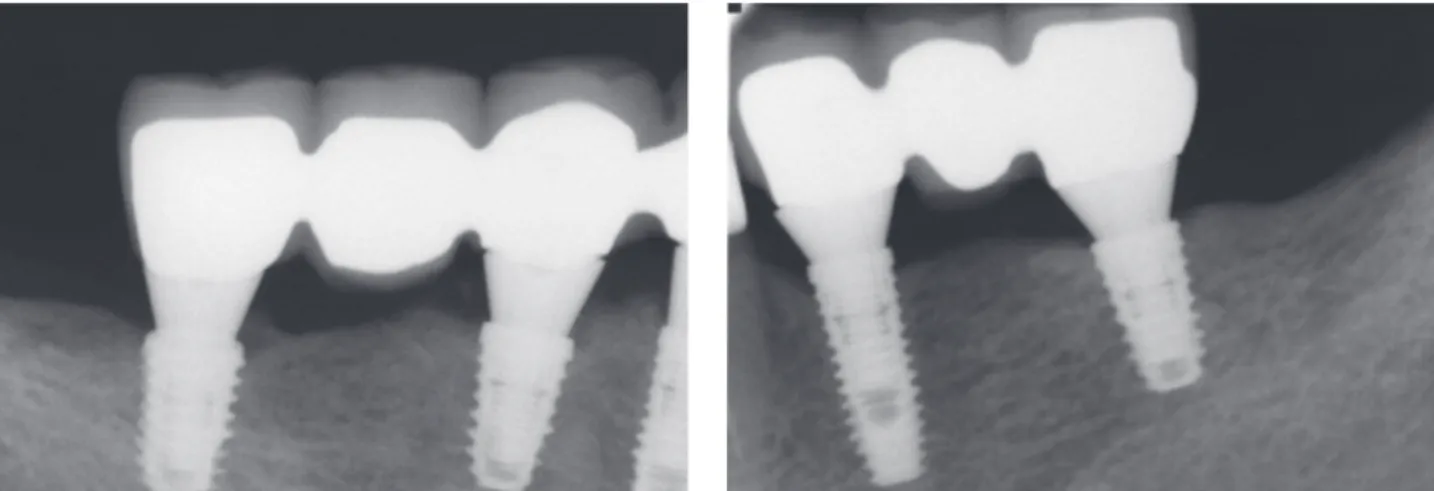
(7) 70. 2019, Vol. 28, Issue 2. Fig. 9. Panoramic radiographic at the 1-year follow-up after loading.. Fig. 10. Intraoral periapical radiographics at the 1-year follow-up after loading.. To evaluate the degree of marginal bone resorption after bone remodeling, panoramic images and intraoral periapical radiographs were evaluated for up to 4 years after prosthesis placement, and a stable marginal bone level was observed. (Fig. 11, 12, 13, 14).
(8) 심하게 위축된 하악 구치부에 치조제 분할술과 블록형 골이식술을 이용한 임플란트 식립: 4년 관찰 증례보고. A. B. C. D. E. F. 71. Fig. 11. Clinical photos of 4-year follow-up after loading. A. Lateral view of right side; B. Frontal view; C. Lateral view of left side; D. Lateral view of right posterior side; E. Occlusal view; F: Lateral view of left posterior side.. Fig. 12. Panoramic radiographic at the 4-year follow-up after loading.. Fig. 13. Intraoral periapical radiographics at the 4-year follow-up after loading. Journal of the Korean Academy of Esthetic Dentistry.
(9) 72. 2019, Vol. 28, Issue 2. Fig. 14. Facial profile photo at the 4-year follow-up after loading.. Discussion and Conclusion. Considering the bone quality and type of resorption, the ridge splitting in the maxilla is an excellent procedure with minimal technical complications and a high success rate.10) However, more than 6.8% of studies have reported fractures of the cortical fragments, resorption, and nerve damage. The majority of studies on alveolar fractures within 3 mm suggest that more considerations may be needed in the mandibular region.11) Various techniques have been developed, and the development of piezo electric devices have made it possible to widen the alveolar ridge even if the residual bone is dense or if there is a lack of cancellous bone between the cortical bones. Nonetheless, in the mandibular posterior region, which is often composed of dense bones with severe atrophy due to bone resorption, the risk of fracture is high with lowered stability of the implant. In such a case of wide bone resorption, without an additional maintenance device, the stability of the bone graft material cannot be guaranteed; thus, using an autogenous bone graft is an excellent method for space maintenance. In the operation of the mandibular posterior area, the flap is easily accessible to the ramus bone, from which high quality autogenous bone can be obtained, compared to other parts. A small autologous bone block can be used with particulated bone graft material using one screw for bone regeneration instead of a large autologous bone with two screws9) The tapered implant design, along with the piezo electric and ridge expansion devices, can minimize buccal bone fracture, even in severely atrophic mandibular areas. Further, a proper grafted keratinized gingiva seems to provide a stable environment on right side. The bone level of right side is the stable, but the premolar area exhibits gingival recession, which should be considered with additional gingival graft. This report demonstrates a case of functional and aesthetic restoration in a patient through a collaboration.. References 1. Barone A, Orlando B, Cingano L, Marconcini S, Derchi G, Covani U. A randomized clinical trial to evaluate and compare implants placed in augmented versus non‐augmented extraction sockets: 3‐year results. Journal of periodontology. 2012 Jul 1;83(7):836-46. 2. Misch CE, Suzuki JB. Tooth extraction, socket grafting, and barrier membrane bone regeneration. Contemporary Implant Dentistry, 3rd ed. St. Louis: Mosby. 2008:870-904. 3. Horváth A, Mardas N, Mezzomo LA, Needleman IG, Donos N. Alveolar ridge preservation. A systematic review..
(10) 심하게 위축된 하악 구치부에 치조제 분할술과 블록형 골이식술을 이용한 임플란트 식립: 4년 관찰 증례보고. 73. Clinical oral investigations. 2013 Mar 1;17(2):341-63. 4. Simion M, Baldoni M, Zaffe D. Jawbone enlargement using immediate implant placement associated with a splitcrest technique and guided tissue regeneration. International Journal of Periodontics & Restorative Dentistry. 1992 Dec 1;12(6). 5. Pikos MA. Block autografts for localized ridge augmentation: Part II. The posterior mandible. Implant dentistry. 2000;9(1):67-75. 6. Lee DW, Lee JW, Lim HC, Kang KL, Choi SH, Yu JA. Simultaneous Block Bone Grafting Using “L-Shaped Notch” Preparation in Mandible: Case Series and 1-Year Follow-up. Implant dentistry. 2015 Oct 1;24(5):625-30. 7. Milinkovic I, Cordaro L. Are there specific indications for the different alveolar bone augmentation procedures for implant placement? A systematic review. International journal of oral and maxillofacial surgery. 2014 May 1;43(5):606-25. 8. Ella B, Laurentjoye M, Sedarat C, Coutant JC, Masson E, Rouas A. Mandibular ridge expansion using a horizontal bone-splitting technique and synthetic bone substitute: an alternative to bone block grafting?. International Journal of Oral & Maxillofacial Implants. 2014 Jan 1;29(1). 9. Vercellotti T. Piezoelectric surgery in implantology: a case report: a new piezoelectric ridge expansion technique. International Journal of Periodontics & Restorative Dentistry. 2000 Aug 1;20(4). 10. Basa S, Varol A, Turker N. Alternative bone expansion technique for immediate placement of implants in the edentulous posterior mandibular ridge: a clinical report. International Journal of Oral & Maxillofacial Implants. 2004 Jul 1;19(4). 11. Jensen OT, Cullum DR, Baer D. Marginal bone stability using 3 different flap approaches for alveolar split expansion for dental implants: a 1-year clinical study. Journal of Oral and Maxillofacial Surgery. 2009 Sep 1;67(9):1921-30.. 심하게 위축된 하악 구치부에 치조제 분할술과 블록형 골이식술을 이용한 임플란트 식립: 4년 관찰 증례보고 심한 치조골의 위축과 흡수로 인한 형태학적 변화는 임플란트의 성공적인 식립과 임플란트의 골유착에 영향을 미친다. 이를 극복하기 위한 다양한 골증대술 중 치조제분할술은 좁은 치조골 폭을 성공적으로 증대시키는 수술방법으로 보고되 었다. 또한 다양하게 개발되는 임플란트 디자인과 치조제 팽창 기구 등은 심하게 흡수된 위축된 하악부위에서도 협측골 파절을 최소화할 수 있다. 가철성 부분의치의 사용으로 심하게 흡수된 하악 구치부에 치조제 분할술과 최소 크기의 블록형 골이식술을 이용해 한개의 스크류로 수용부의 고정을 획득한 후 동시적 접근법을 이용한 골이식 증례를 보고 하고자 한다. 보철과와 치주과의 협업으로 환자의 기능과 심미를 회복해준 증례로 사료된다. 키워드: 치조제 분할술, 동시식립, 블록형 골이식, 협진. Journal of the Korean Academy of Esthetic Dentistry.
(11)
수치

+5


관련 문서
