Immediate Effect of Anterior-to-posterior Talocrural Joint Mobilization with Elastic Taping on Balance Ability in Stroke Patients
7
0
0
전체 글
(3)
(4)
(5)
(6)
(7)
수치

관련 문서
Conclusion: Aromatherapy with neroli essential oil had a difference in brain wave and brain utilization ability according to the MBTI personality type
The result suggested that a taekwon aerobics program had a positive effect on the increase of growth hormone in blood lipid in middle school girls.. The
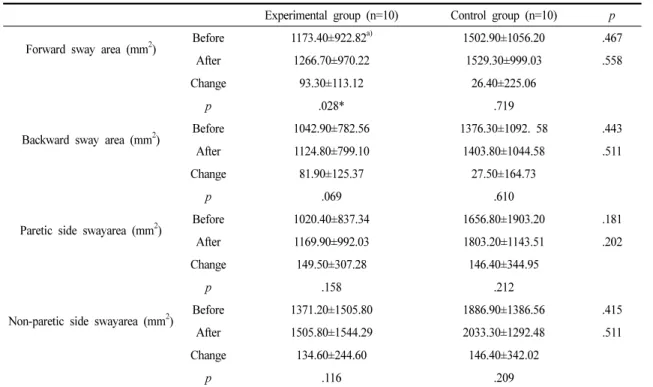
Third, for the change in balance ability according to core training and plyometric training, the core group showed a significant difference in travel area
Based on the above results, participation in judo sports clubs has a positive effect on the body composition of elementary school students, which
Figure 12.3.1a shows a simply-supported, linearly-elastic, simple beam with a transverse load Q applied at its midspan and a compressive load P directed along its centroidal
- Divergence: independent of (initial a.o.a) and airfoil camber the increase in aerodynamic moment about the elastic axis due to an arbitrary change in a.o.a is equal
The study consisted of applying the taping measures to 10 professional golfers and observe its effects, before and after such measure. The taping was applied
In this study, we developed a non-toxic titanium alloy with low elastic modulus in order to improve biocompatibility, and the surface characteristics of
