서 론
고혈압은 우리나라의 대표적인 만성 질환으로 2014년 국민건강통 계에 의하면 30세 이상의 성인에서 약 25.5%의 유병률을 보이고 있 다. 또한, 우리나라 성인의 사망 원인 중 2위와 3위인 뇌혈관 질환 및 심장 혈관 질환과 아주 밀접한 관계가 있다고 알려져 있어서,1,2) 고혈 압의 예방과 관리가 국민건강 증진에 매우 중요한 문제로 인식되고 있다.
고혈압의 예방과 동시에 치료가 될 수 있는 생활요법이 강조되기
도 하는데 운동과 체중조절, 식습관 개선, 금주와 금연 등이 바로 그 러한 방법들이다.3,4)
저염식은 대표적인 식습관 개선 방법으로서, 나트륨 과다 섭취가 혈압 상승의 원인이 된다는 연구 결과에 바탕을 두고 있다.5) 오랫동 안 저염식이 혈압 조절에 긍정적인 영향을 끼치는가에 대한 논란이 있어 왔고 여러 연구가 시행되어 왔다.
한편, 세계보건기구(World Health Organization)의 하루 나트륨 권 장량은 2,000 mg인데 2014년 국민건강영양조사를 통해 나타난 우리 나라 국민 1인당 1일 평균 나트륨 섭취량은 3,890 mg으로 권장량의 2 Received May 11, 2017 Accepted July 26, 2017
Corresponding author Won-Chul Yang Tel: +82-2-536-0740, Fax: +82-2-536-0740 E-mail: [email protected]
ORCID: http://orcid.org/0000-0001-5759-985X
Copyright © 2018 The Korean Academy of Family Medicine
This is an open-access article distributed under the terms of the Creative Commons At- tribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Original Article
https://doi.org/10.21215/kjfp.2018.8.3.359 eISSN 2233-9116
Korean J Fam Pract. 2018;8(3):359-363
Korean Journal of Family Practice
KJFP
한국 성인에서 혈압과 요중 나트륨과의 연관성
양원철*, 강병두, 유상은, 김정환, 류재열
세림병원 가정의학과
Association between Blood Presure and Urinary Sodium in Korean Adults
Won-Chul Yang*, Byung-Du Kang, Sang-Eun Yu, Joung-Hwan Kim, Jae-Yeol Ryu Department of Family Medicine, Serim Hospital, Incheon, Korea
Background: Hypertension, one of the most prevalent diseases in Korean adults, can cause stroke and other cardiovascular diseases that could be fatal.
Although sodium is recognized as a risk factor for hypertension, the current salt intake among Koreans is relatively high. We examined the relationship between blood pressure and urinary sodium levels in the general Korean population.
Methods: We analyzed data from the Korea National Health and Nutrition Examination Survey between 2014 and 2015 and included 5,898 participants in our study. Patients were divided into 5 groups based on SBP and DBP readings: ≥150 mmHg, 140–149 mmHg, 130–139 mmHg, 120–129 mmHg, and <120 mmHg. We evaluated the participants based on sex; age; body mass index; and glycosylated hemoglobin, total cholesterol, low-density lipoprotein, and triglyceride levels. Multiple logistic regression models were used to assess the association between urinary sodium and blood pressure. We calculated the odds ratios (ORs) for the urinary sodium-to-creatinine ratio.
Results: Urinary sodium-to-creatinine ratios showed a correlation with SBP (r=0.228, P<0.0001) and DBP (r=0.075, P<0.0001). ORs (95% confidence intervals [CI]) for the urinary sodium-to-creatinine ratio after adjustment were 1.00, 1.207 (95% CI, 0.991–1.469), 1.277 (95% CI, 1.00–1.632), 1.399 (95% CI, 1.015–1.927), and 2.89 (95% CI, 1.933–4.323) for the five SBP (DBP) groups and 1.00, 1.05 (95% CI, 0.669–1.646), 1.132 (95% CI, 0.72–1.78), 1.415 (95% CI, 0.89–2.25), and 1.407 (95% CI, 0.829–2.39) for the five SBP (DBP) groups, respectively.
Conclusion: Higher SBP was independently associated with a higher urinary sodium-to-creatinine ratio, which indicates an individual’s dietary sodium intake.
Keywords: Sodium; Hypertension; Diet
Won-Chul Yang, et al. Association between Blood Presure and Urinary Sodium in Korean Adults
Korean Journal of Family Practice
KJFP
배 가까이 높게 나타나고 있다.
이에, 나트륨 섭취량이 혈압과 어떤 상관 관계가 있을지 확인해 보 는 것은 중요하다고 판단된다. 이러한 배경을 바탕으로 본 연구에서 는 국민건강영양조사 자료를 통해 한국인에서 혈압과 요중 나트륨 의 관련성에 대해 알아보고자 한다.
방 법
1. 연구 대상
이 연구는 2014–2015년 국민건강영양조사의 자료를 활용하였다.
국민건강영양조사는 우리나라 국민의 건강 및 영양 상태에 관한 전 반적인 현황 및 추이를 종합적으로 파악하는 것을 목적으로 한 우 리나라 전체 인구를 대표하는 확률표본을 대상으로 이루어져 있다.
2014–2015년도 국민건강영양조사에 참여한 응답자 14,930명 중 만 30세 이상, 만성 콩팥병 제외, 당뇨병 제외, 혈압 조절제 복용자 제 외, 기타 응답 누락이나 무응답자를 제외한 5,898명을 본 연구의 대 상으로 하였다.
2. 연구 방법
국민건강영양조사는 조사항목에 따라 건강설문조사, 검진조사, 영양조사 3가지 부문으로 구성되어 있다. 연구 대상자들의 기본적 인 특성을 파악하고 나트륨 섭취량과 혈압 간의 관계를 알아보기 위 하여 건강설문조사 부문의 성별과 연령, 검진조사 부문의 체질량지 수(BMI) 및 혈압 및 혈액 검사자료를 사용하였다.
혈압 측정은 모든 대상자들은 5분의 간격을 두고 3회 측정하였고, 두 번째와 세 번째 측정한 혈압의 평균값을 사용하였다. 혈액검사는 최소 8시간 금식을 한 후 아침에 채혈을 하였으며, 소변 검사는 아침 첫 소변을 이용하였다.
나트륨 섭취량은 요중 나트륨 농도값을 요중 크레아티닌으로 보 정한 값(ratio of urine sodium to creatinine, NC RATIO)으로 치환하여 알아보기로 하였다.
3. 통계분석
수축기 혈압과 이완기 혈압을 모두 5개 군으로 나누었다. 수축기 혈압은 120 mmHg 미만, 120–129 mmHg, 130–139 mmHg, 140–149 mmHg, 150 mmHg 이상으로 나누었고, 이완기 혈압은 60 mmHg 미 Table 1. General characteristics according to SBP groups
Characteristic SBP (mmHg)
P-value*
<120 (n=3,732) 120–129 (n=1,038) 130–139 (n=603) 140–149 (n=299) ≥150 (n=226)
Sex (male) 42.6 (0.8) 63.6 (1.4) 59.7 (2.3) 54.6 (3.3) 51.7 (4) <0.0001
Age (y) 45.7±0.3 50.6±0.5 53.3±0.6 57.2±0.8 58.7±1.1 <0.0001†
BMI (kg/m2) 23.2±0.1 24.5±0.1 24.9±0.2 24.8±0.3 24.3±0.3 <0.0001
HbA1c (%) 5.52±0.01 5.69±0.03 5.69±0.03 5.72±0.04 5.77±0.07 <0.0001
TC (mg/dL) 191.6±0.7 201.5±1.3 198.9±1.8 203.1±2.6 199.1±3.3 <0.0001
LDL-C (mg/dL) 114.7±0.6 119.6±1.2 118.2±1.8 121.1±2.5 114.5±3.4 0.0007
TG (mg/dL) 127.8±2.2 167.9±5.5 166.6±6.5 160.7±6.9 185.8±14.1 <0.0001
UNa (mmol/L) 111.9±0.9 126.5±1.7 120±2.5 129.3±3.5 134.4±4.4 <0.0001
UCREA (mg/dL) 155.2±1.7 157.9±2.8 145.9±5 133.2±5 114.6±5.7 <0.0001
NC RATIO 0.91±0.01 1.01±0.02 1.14±0.05 1.23±0.05 1.48±0.06 <0.0001
DBP (mmHg)
<60 (n=264) 60–69 (n=1,479) 70–79 (n=2,310) 80–89 (n=1,360) ≥90 (n=485)
Sex (male) 23.8 (3.1) 30.1 (1.3) 47.9 (1.2) 64 (1.4) 72.3 (2.1) <0.0001
Age (y) 48.6±1.2 47.8±0.5 48.1±0.3 48.4±0.4 48.5±0.5 0.7077†
BMI (kg/m2) 22.1±0.2 22.6±0.1 23.5±0.1 24.6±0.1 25.5±0.2 <0.0001
HbA1c (%) 5.5±0.03 5.5±0.01 5.56±0.01 5.69±0.03 5.64±0.03 <0.0001
TC (mg/dL) 183.1±2.4 187.4±0.9 193.5±0.8 201.9±1.1 204.8±1.8 <0.0001
LDL-C (mg/dL) 107.6±2.3 111.7±0.8 116.2±0.7 120.7±1 119.3±1.8 <0.0001
TG (mg/dL) 96.2±5.4 109.4±2.7 138.1±3.1 165±4.6 197.1±7.8 <0.0001
UNa (mmol/L) 110±3.6 112.3±1.5 115.4±1.2 120.7±1.6 126.1±2.6 <0.0001
UCREA (mg/dL) 140.3±6.5 145.2±2.6 154.7±2.1 156.1±2.6 158.8±4.3 0.0025
NC RATIO 1.05±0.06 0.98±0.02 0.95±0.01 1±0.02 1.05±0.05 0.1262
Values are presented as number (%) or mean±standard error, unless otherwise indicated.
SBP, systolic blood pressure; DBP, diastolic blood pressure; BMI, body mass index; HbA1c, glycosylated hemoglobin; TC, total cholesterol; LDL-C, low-density lipoprotein;
TG, triglyceride; UNa, urine sodium; UCREA, urine creatinine; NC RATIO, ratio of urine sodium to creatinine.
*P-value was calculated by analysis of variance except value marked by †. †By the chi-square test.
양원철 외. 한국 성인에서 혈압과 요중 나트륨과의 연관성 Korean Journal of Family Practice
KJFP
만, 60–69 mmHg, 70–79 mmHg, 80–89 mmHg, 90 mmHg 이상으로 나누었다. 각각의 군에 따른 임상적 특징들은 연속형 변수인 경우 평 균±표준편차, 범주형 변수인 경우 퍼센트로 표시하였다.
혈압에 영향을 줄 것으로 생각되는 인자들인 Age, BMI, glycosylat- ed hemoglobin (HbA1c), total cholesterol (TC), low-density lipoprotein cholesterol (LDL-C), triglycerides (TG)과 요중 나트륨과 Pearson 상관 분석을 하였고, 요중 나트륨을 크레아티닌으로 보정한 값인 요중 나 트륨/크레아니틴과의 상관분석을 하였다. 혈압군에 따른 요중 나트 륨의 연관성을 알아보기 위해 성별, 나이, BMI, HbA1c, TC, LDL-C, TG를 보정한 다중로지스틱 회귀분석을 통해 교차비(odds ratios, ORs)와 95% 신뢰구간(95% confidence intervals, 95% CIs)을 구하였다.
통계적 유의성은 P<0.05일 경우 유의한 것으로 보았으며, 통계 분석 은 SAS statistical version 9.3 (SAS Institute Inc., Cary, NC, USA)을 통해 수행하였다.
결 과
SBP와 DBP를 혈압 수치에 따라 5개의 군으로 나눈 임상적인 특징 은 Table 1과 같다. SBP가 증가할수록 Age, HbA1c, 요중 나트륨이 증 가하였고, DBP가 증가할수록 BMI, HbA1c, TC, LDL, TG, 요중 크레 아티닌이 증가하였다.
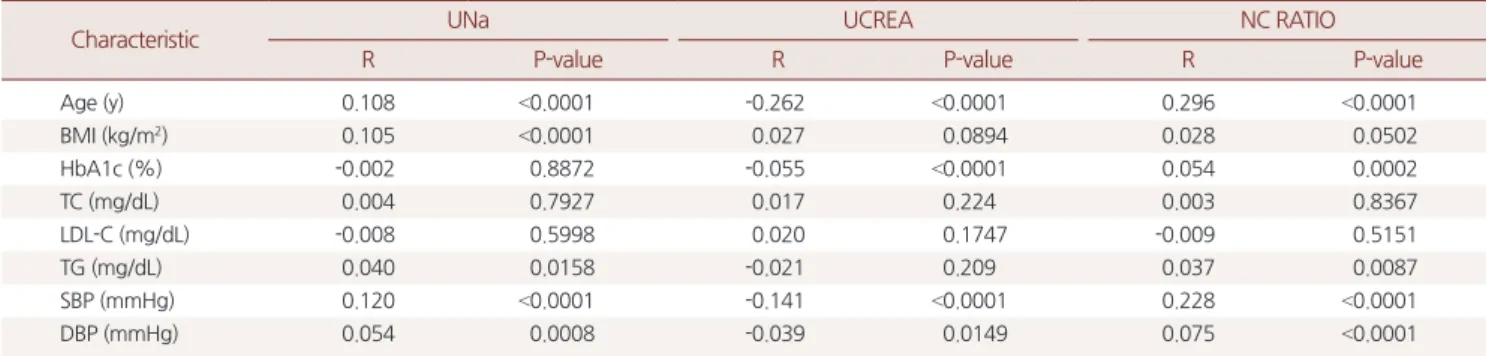
요중 나트륨/크레아티닌 값과 혈압 변화에 영향을 줄 것으로 생각 되는 인자들인 Age, BMI, HbA1c, TC, LDL-C, TG간의 상관 관계를 확인해본 결과, Age, HbA1c, TG가 유의한 양의 상관 관계를 보였다 (Table 2).
SBP<120 mmHg 군을 기준으로 할 때 SBP가 높아질수록 NC RATIO의 ORs는 높아졌다. SBP의 각 혈압군에서 보정한 다중 로지 스틱 회귀분석에서 OR, 1.207 (95% CI, 0.991–1.469) OR, 1.277 (95% CI, 1.000–1.632), OR, 1.399 (95% CI, 1.015–1.927), OR, 2.89 (95% CI, 1.933–
4.323)이었다. DBP<120 mmHg 군을 기준으로 할 때 DBP가 높아질수 록 NC RATIO의 ORs는 높아졌으나 유의하지 않았다. DBP군에서는 OR, 1.05 (95% CI, 0.669–1.646), OR, 1.132 (95% CI, 0.72–1.78), OR, 1.415 (95% CI, 0.89–2.25), OR, 1.407 (95% CI, 0.829–2.39)이었다(Table 3).
고 찰
나트륨은 인간에게 꼭 필요한 필수 영양소이자, 신장에서 조절되 어 우리 몸의 체액 균형을 맞추는데 큰 역할을 하는 무기질이다. 인 체 내에서 나트륨이 부족하면 수분 과잉으로 부종 상태가 나타나는 저나트륨혈증을 일으켜, 두통, 혼수, 근육 경련 등의 증상을 나타낼 수 있다. 반면 나트륨 과잉 섭취는 고혈압,5) 골다공증,6) 심장병,7) 뇌졸 중,8) 위암,9) 만성신부전10)의 발생과 연관이 있다고 알려져 있다.
혈압은 심박출량과 말초혈관저항에 의해 결정되며 나트륨이 이 두 가지 요인에 모두 관여하여 혈압에 영향을 끼친다고 알려져 있다.
첫째로, 나트륨 섭취량이 증가하여 나트륨 이온이 혈관 내에 과잉 축적되면 삼투압이 증가하여 혈액량이 증가하게 되고 이는 혈압 상 승을 야기시킨다.11,12) 둘째로, 나트륨 섭취량 증가는 endogenous oua- bain의 분비를 자극시켜 Na+ pump의 활성화를 저하시키고 세포 내 Na+ 농도 증가를 야기시킨다. 이에 Na+/Ca2+ exchanger를 통해 Ca2+ 농 도가 증가되며, 이는 세동맥벽의 수축을 야기시켜 혈압이 올라가게 된다고 설명한다.13,14)
이러한 이론적 연구에 바탕을 두고 요나트륨과 혈압간의 상관성 을 증명하려는 연구도 많이 이루어졌다.
유럽인을 대상으로 한 혈압과 요나트륨간의 상관성 연구에서 요 나트륨/크레아티닌이 증가할수록 평균 동맥압과 평균 정맥압이 상 승함이 증명되었고,15) 정상 혈압인 일본인을 대상으로 한 혈압과 요 나트륨간의 상관성 연구에서 요나트륨과 수축기 혈압과 양의 상관 성이 증명되기도 하였다.16)
Table 2. Partial correlation of the NC RATIO
Characteristic UNa UCREA NC RATIO
R P-value R P-value R P-value
Age (y) 0.108 <0.0001 -0.262 <0.0001 0.296 <0.0001
BMI (kg/m2) 0.105 <0.0001 0.027 0.0894 0.028 0.0502
HbA1c (%) -0.002 0.8872 -0.055 <0.0001 0.054 0.0002
TC (mg/dL) 0.004 0.7927 0.017 0.224 0.003 0.8367
LDL-C (mg/dL) -0.008 0.5998 0.020 0.1747 -0.009 0.5151
TG (mg/dL) 0.040 0.0158 -0.021 0.209 0.037 0.0087
SBP (mmHg) 0.120 <0.0001 -0.141 <0.0001 0.228 <0.0001
DBP (mmHg) 0.054 0.0008 -0.039 0.0149 0.075 <0.0001
NC RATIO, ratio of urine sodium to creatinine; UNa, urine sodium; UCREA, urine creatinine; BMI, body mass index; HbA1c, glycosylated hemoglobin; TC, total cholester- ol; LDL-C, low-density lipoprotein; TG, triglyceride; SBP, systolic blood pressure; DBP, diastolic blood pressure.
Pearson's partial correlation coefficient. Adjusted by sex.
Won-Chul Yang, et al. Association between Blood Presure and Urinary Sodium in Korean Adults
Korean Journal of Family Practice
KJFP
나트륨 섭취량과 혈압과의 관계에 대한 연구 역시 여러 그룹에서 보고된 바 있다. Fotherby 와 Potter17)의 연구에 의하면 노인 고혈압 환 자에서 저염식을 한 경우 누운 자세로 측정한 수축기 혈압이 의미있 게 낮아졌다고 보고하였고, Kobayashi와 Kajiwara18)은 경계성 고혈압 환자군에서 중등도의 염분 제한식이를 시행한 결과 수축기 혈압과 이완기 혈압 모두 낮아졌음을 보고하였다. Graudal 등19)은 백인, 흑 인, 아시아인을 대상으로 한 저염식 실행연구 결과 정상혈압군에서 1%, 고혈압군에서 3.5%의 혈압 감소가 있었음을 보고하였다.
반면, 노인에게서의 나트륨 섭취가 심혈관질환이나 심부전의 발 생 및 사망률과 연관 없다는 연구 발표가 있었고,20) 나트륨 섭취량 제한이 심혈관질환 시 사망률의 감소로 이어진다는 강력한 증거가 없다는 연구 결과도 있었다.21)
또한, 2013년 미국의학회(Institute Of Medicine, IOM)에서는 미국 인을 위한 식사지침(Dietary Guidelines for Americans)에서 권고한 하 루 2,300 mg/day 이하의 나트륨 섭취가 심장질환, 뇌졸중 그리고 다 른 모든 사망원인을 높이거나 낮춘다는 증거가 부족하다고 하였다.
2013년 미국심장협회(American Heart Association, AHA)에서는 나트 륨 섭취량을 2,400 mg/day로 권고하기도 하는 등 최근 나트륨 섭취 권고량에 대한 기준이 완화되고 있는 움직임도 있어서 나트륨 섭취 제한이 가져오는 이점에 대한 논쟁이 진행되고 있다고 할 수 있겠다.
본 연구는 몇 가지 한계가 있다. 첫째, 단면 연구라 요중 나트륨과 혈압 증가 사이의 선후 인과 관계를 파악할 수 없다. 둘째, 고혈압을 유발할 수 있는 모든 인자를 사실상 통제하기 어려워서 그 정확성이 떨어질 수 있다. 예를 들면 본 연구에서는 혈압에 영향을 끼칠 수 있
는 인자로서 음주나 흡연에 대한 보정 연구는 이루어지지 않았다. 셋 째, 일반적으로 금식 후 오전에 채취된 소변은 다른 시간대의 소변보 다 더 농축된다. 따라서 요중 나트륨 농도 수치가 정확하게 측정되지 않았을 가능성도 배제하지 못한다.
결론적으로 만성콩팥병, 당뇨병이 없는 30세 이상 성인에서 SBP 가 증가할수록 요나트륨의 농도가 높았고, DBP와는 유의한 상관 관 계를 보이지 않았다. 이를 통해, 나트륨섭취가 증가할수록 고혈압의 위험도가 높아진다고 판단할 수 있겠다. 단, 요나트륨의 농도와 DBP 간에는 유의한 상관성을 보이지 않아서 이에 대한 연구가 더 필요하 다고 생각된다.
요 약
연구배경:
고혈압은 한국 성인에서 가장 흔한 질병 중 하나이다. 그 리고 치명적일 수 있는 뇌졸증이나 다른 심장혈관질환을 일으킬 수 있다. 나트륨 과잉섭취는 고혈압의 위험인자로 알려져 있으나 현재 한국인들의 나트륨 섭취는 굉장히 높은 편이다. 이에 본 연구에서는 당뇨 및 만성 신장질환이 없는 한국 성인에서의 요중 나트륨과 혈압 과의 관계를 알아보고자 한다.방법:
2014–2015년의 한국 국민건강영양조사 자료를 분석하였으며 총 5,898명을 대상으로 연구하였다. 수축기 혈압은 150 mmHg 이상, 140–149 mmHg, 130–139 mmHg, 120–129 mmHg, 120 mmHg 미만으 로, 이완기 혈압은 90 mmHg 이상, 80–89 mmHg, 70–79 mmHg, 60–69 mmHg, 60 mmHg 미만인 다섯 그룹으로 나누었다. 혈압에 영향 Table 3. Multivariate logistic regression
Variable SBP (mmHg)
P-value
<120 120–129 130–139 140–149 ≥150
Model 1 1 (reference) 1.344
(1.141, 1.584)
1.795 (1.445, 2.229)
2.138 (1.592, 2.871)
4.485 (3.269, 6.155)
<0.0001
Model 2 1 (reference) 1.233
(1.028, 1.478)
1.458 (1.16, 1.832)
1.433 (1.06, 1.935)
3.01 (2.11, 4.293)
<0.0001
Model 3 1 (reference) 1.207
(0.991, 1.469)
1.277 (1, 1.632)
1.399 (1.015, 1.927)
2.89 (1.933, 4.323)
<0.0001
DBP (mmHg)
<60 60–69 70–79 80–89 ≥90
Model 1 1 (reference) 0.956
(0.655, 1.395)
0.911 (0.625, 1.328)
0.992 (0.682, 1.441)
1.032 (0.684, 1.558)
0.8502
Model 2 1 (reference) 1.06
(0.719, 1.562)
1.111 (0.752, 1.641)
1.365 (0.921, 2.024)
1.519 (0.977, 2.36)
0.0276
Model 3 1 (reference) 1.05
(0.669, 1.646)
1.132 (0.72, 1.78)
1.415 (0.89, 2.25)
1.407 (0.829, 2.39)
0.0703
Values are presented as odds ratio (95% confidence interval).
Model 1: non adjusted. Model 2: sex, age, BMI adjusted. Model 3: sex, age, BMI, HbA1c, TC, LDL-C, TG adjusted.
SBP, systolic blood pressure; DBP, diastolic blood pressure; BMI, body mass index; HbA1c, glycosylated hemoglobin; TC, total cholesterol; LDL-C, low-density lipopro- tein; TG, triglyceride.
양원철 외. 한국 성인에서 혈압과 요중 나트륨과의 연관성 Korean Journal of Family Practice
KJFP
을 끼치는 요소인 성별, 나이, 체질량지수, 당화혈색소, 총콜레스테 롤, LDL 콜레스테롤, 중성지방의 평균을 비교하고, 요중 나트륨과의 상관 관계를 확인하였다. 다중 로지스틱 회귀분석을 통해 요중 나트 륨/크레아티닌에 대한 교차비를 구하고 유의한지 알아보았다.
결과:
요중 나트륨/크레아티닌 수치는 수축기 혈압과 이완기 혈압은 모두 양의 상관성을 보였다. 연령, 성별, 체질량지수, 당화혈색소, 총 콜레스테롤, 저밀도지단백질, 중성지방을 보정한 다중 로지스틱 회 귀분석 결과에서 요중 나트륨/크레아티닌의 수치가 높을수록 수축 기 혈압이 통계적으로 유의하게 높았으나, 이완기 혈압은 의미 있는 결과를 보여주지 않았다.결론:
당뇨 및 만성 신장질환이 없는 30세 이상의 성인에서 수축기 혈압이 높을수록 나트륨 섭취량의 척도인 요중 나트륨/크레아티닌 수치가 높았다.중심단어:
나트륨; 고혈압; 식습관REFERENCES
1. Messerli FH, Schmieder RE, Weir MR. Salt. A perpetrator of hypertensive target organ disease? Arch Intern Med 1997; 157: 2449-52.
2. He FJ, MacGregor GA. Salt, blood pressure and cardiovascular disease. Curr Opin Cardiol 2007; 22: 298-305.
3. Campbell NR, Burgess E, Choi BC, Taylor G, Wilson E, Cléroux J, et al. Life- style modifications to prevent and control hypertension. 1. Methods and an overview of the Canadian recommendations. Canadian Hypertension So- ciety, Canadian Coalition for High Blood Pressure Prevention and Control, Laboratory Centre for Disease Control at Health Canada, Heart and Stroke Foundation of Canada. CMAJ 1999; 160(9 Suppl): S1-6.
4. Khan NA, Hemmelgarn B, Herman RJ, Bell CM, Mahon JL, Leiter LA, et al.
The 2009 Canadian hypertension education program recommendations for the management of hypertension: part 2--therapy. Can J Cardiol 2009;
25: 287-98.
5. Blaustein MP, Hamlyn JM. Signaling mechanisms that link salt retention to hypertension: endogenous ouabain, the Na+ pump, the Na+/Ca2+ exchanger and TRPC proteins. Biochim Biophys Acta 2010; 1802: 1219-29.
6. Park SM, Jee J, Joung JY, Cho YY, Sohn SY, Jin SM, et al. High dietary sodium intake assessed by 24-hour urine specimen increase urinary calcium excre- tion and bone resorption marker. J Bone Metab 2014; 21: 189-94.
7. Pfister R, Michels G, Sharp SJ, Luben R, Wareham NJ, Khaw KT. Estimated urinary sodium excretion and risk of heart failure in men and women in the EPIC-Norfolk study. Eur J Heart Fail 2014; 16: 394-402.
8. Gardener H, Rundek T, Wright CB, Elkind MS, Sacco RL. Dietary sodium and risk of stroke in the Northern Manhattan study. Stroke 2012 ;43: 1200- 5.
9. Dias-Neto M, Pintalhao M, Ferreira M, Lunet N. Salt intake and risk of gas- tric intestinal metaplasia: systematic review and meta-analysis. Nutr Cancer 2010; 62: 133-47.
10. Liu N, Sun W, Xing Z, Ma F, Sun T, Wu H, et al. Association between sodium intakes with the risk of chronic kidney disease: evidence from a meta-analy- sis. Int J Clin Exp Med 2015; 8: 20939-45. eCollection 2015.
11. Blaustein MP, Zhang J, Chen L, Hamilton BP. How does salt retention raise blood pressure? Am J Physiol Regul Integr Comp Physiol 2006; 290: R514- 23.
12. Freis ED. Salt, volume and the prevention of hypertension. Circulation.
1976; 53: 589-95.
13. Blaustein MP. Sodium ions, calcium ions, blood pressure regulation, and hy- pertension: a reassessment and a hypothesis. Am J Physiol 1977; 232: C165- 73.
14. Blaustein MP. The role of Na-Ca exchange in the regulation of tone in vas- cular smooth muscle. In: Casteels R, Godfraind T, Rüegg JC, editors. Inter- national Symposium on Excitation-Contraction Coupling in Smooth Mus- cle (1977: Louvain, Belgium). Excitation-contraction coupling in smooth muscle : proceedings of the International Symposium on Excitation-Con- traction Coupling in Smooth Muscle held in Louvain, Belgium, 12-14 July, 1977 and the Erwin-Riesch Symposium in Heidelberg, Germany, 15-16 July 1977 Amsterdam; New York: Elsevier/North-Holland, 1977. Amsterdam;
New York: Elsevier/North-Holland; 1977. p. 101-8.
15. Khaw KT, Bingham S, Welch A, Luben R, O’Brien E, Wareham N, et al. Blood pressure and urinary sodium in men and women: the norfolk cohort of the European prospective investigation into cancer (EPIC-Norfolk). Am J Clin Nutr 2004; 80: 1397-403.
16. Umesawa M, Yamagishi K, Noda H, Ikeda A, Sawachi S, Muraki I, et al. The relationship between sodium concentrations in spot urine and blood pres- sure increases: a prospective study of Japanese general population: the circu- latory risk in communities study (CIRCS). BMC Cardiovasc Disord 2016;
16: 55.
17. Fotherby MD, Potter JF. Effects of moderate sodium restriction on clinic and twenty-four-hour ambulatory blood pressure in elderly hypertensive subjects. J Hypertens 1993; 11: 657-63.
18. Kobayashi Y, Kajiwara N. Treatment of borderline hypertension--moderate salt restriction in the treatment of borderline hypertension. Jpn Circ J 1983;
47: 268-75.
19. Graudal NA, Hubeck-Graudal T, Jurgens G. Effects of low sodium diet ver- sus high sodium diet on blood pressure, renin, aldosterone, catecholamines, cholesterol, and triglyceride. Cochrane Database Syst Rev 2011; (11):
CD004022.
20. Kalogeropoulos AP, Georgiopoulou VV, Murphy RA, Newman AB, Bauer DC, Harris TB, et al. Dietary sodium content, mortality, and risk for cardio- vascular events in older adults: the health, aging, and body composition (Health ABC) study. JAMA Intern Med 2015; 175: 410-9.
21. Taylor RS, Ashton KE, Moxham T, Hooper L, Ebrahim S. Reduced dietary salt for the prevention of cardiovascular disease. Cochrane Database Syst Rev 2011; (7): CD009217.