서 론
국내의 매독감염은 1970년대 이후 급격히 감소하여 2000년에는 Venereal Disease Research Laboratory (VDRL)와 fluorescent treponemal antibody absorption test (FTA-ABS) 동시 양성 324
DOI 10.3343/kjlm.2007.27.5.324
324
자동화 매독검사인 Mediace Rapid Plasma Reagin과 Treponema pallidum Latex Agglutination 양성 결과 분석
Analysis of Positive Results in Mediace Rapid Plasma Reagin and Treponema pallidum Latex Agglutination as the Automated Syphilis Test
Hee Jin Huh, M.D.
1, Kyo Kwan Lee, M.D.
1, Eu Suk Kim, M.D.
2, and Seok-Lae Chae, M.D.
1Departments of Laboratory Medicine1and Internal Medicine2, College of Medicine, Dongguk University, Gyeonggi Province, Korea 허희진1∙이교관1∙김의석2∙채석래1
동국대학교 의과대학 진단검사의학교실1, 내과학교실2
324 324
Background : We compared the results of automated and quantitative methods for the diagnosis of syphilis, Mediace Rapid Plasma Reagin (RPR) and Mediace Treponema pallidum Latex Aggluti- nation (TPLA) (Sekisui Chemical Co., Ltd, Japan) with those of conventional methods.
Methods :Sera from 3,896 persons who had health checkups between December 2005 and November 2006 were included in the evaluation of positive rates and biological false positives (BFP) for Mediace RPR and TPLA. In addition, 134 patients’ sera positive for automated Mediace RPR or TPLA were tested for VDRL and TPHA. Discrepancies between TPLA and TPHA results were con- firmed by the RecomBlot Treponemal IgG/IgM (Mikrogen GmbH, Germany). Automated Mediace RPR and TPLA were performed using the Hitachi 7600 chemistry autoanalyzer (Hitachi, Japan). Sam- ples with positive Mediace RPR and negative TPLA results were defined as BFP.
Results :Positive rate of automated Mediace RPR was 0.23% (9/3,896). BFP of the Mediace RPR was 0.18%. Positive rate of automated TPLA was 1.62% (37/2,284). Among the 134 patients’ sera, 33 (24.6%) showed a discrepancy between conventional VDRL and automated Mediace RPR results:
Among 31 Mediace RPR(+)/VDRL(-) sera, 13 were positive and 18 were negative for TPLA. The remaining 2 sera of discrepancy with Mediace RPR(-)/VDRL(+) were all positive for TPLA. There were seven sera that showed a discrepancy between automated TPLA and TPHA results: Two sera with Mediace RPR(+)/TPLA(-)/TPHA(+) showed negative recomBlot Treponemal IgG/IgM results, and among five sera with TPLA(+)/TPHA(-), three demonstrated IgG or IgM by recomBlot Trepone- mal IgG/IgM.
Conclusions :The results of comparison data demonstrated that automated TPLA results had a high concordance with recomBlot Treponemal IgG/IgM results. Moreover, there are additional advan- tages of automated methods such as quantitative detection, low infection risk, and no influence by human handling. (Korean J Lab Med 2007;27:324-9)
Key Words : Automated Mediace RPR, TPLA, VDRL, TPHA
접 수: 2007년 2월 10일 접수번호:KJLM2017 수정본접수: 2007년 8월 16일
게재승인일: 2007년 9월 23일 교 신저 자: 채 석 래
우 411-773 경기도 고양시 일산동구 식사동 814 동국대학교 의과대학 진단검사의학교실 전화: 031-961-7890, Fax: 031-961-7902 E-mail: [email protected]
률이 0.2%로 감소되었다고 보고되고 있지만, 질병관리본부의 표 본감시체계 통계자료에 따르면 그 이후 매독환자는 점차 증가추세 를 보이고 있다[1]. 그러므로 공혈자 검사나 건강검진, 침습적인 시술 전 검사 등으로 시행되고 있는 매독검사는 여전히 중요한 검 사이다.
비트레포네마검사(nontreponemal test)와 트레포네마검사(tre- ponemal test) 두 가지 검사법으로 구분되는 혈청학적 방법은 매독의 선별검사뿐만 아니라 확진검사로 가장 유용하게 이용되고 있다[2]. 매독진단을 위한 지침은 다양해서 효소면역법(enzyme immunoassay)을 선별검사에 이용하거나 비트레포네마검사와 트 레포네마검사를 동시에 선별검사로 적용하는 경우도 있지만[3], 주로 비트레포네마검사인 VDRL, card rapid plasma reagin (RPR) 등을 선별검사에 트레포네마검사인 FTA-ABS, Tre- ponemal pallidum particle agglutination (TP-PA), T. pal- lidum hemagglutination assay (TPHA) 등을 확진검사에 이용 하고 있다[4]. 이처럼 매독진단을 위한 검사법이 다양하고 두 방 법의 검사를 진단에 이용 해야 하는 이유는, 한가지 혈청학적 검 사만으로는 과거 감염과 현증을 구별할 수 없고, 비트레포네마검 사가 생물학적 위양성과 발병초기와 말기 매독에 위음성을 보이 는 문제가 있고, 트레포네마검사도 위음성과 위양성의 가능성이 있기 때문이다[5].
또한, 국내에서 주로 이용되는 수기법인 VDRL, TPHA, FTA- ABS 등은 검사시간이 오래 걸리고 검사자 간 결과판독에 차이를 보이며 감염의 위험이 있는 단점이 있어, 생물학적 위양성의 가 능성을 최소화하고 민감하면서 간단하게 검사할 수 있는 자동화 기법이 필요한 실정이다. 최근 라텍스 응집 비탁법을 기본으로 생화학 자동분석기로 검사할 수 있고 정량 가능한 비트레포네마 검사 시약인 MediaceTM RPR (Sekisui Chemical Co., Ltd, Osaka, Japan; 이하 Mediace RPR)과 트레포네마검사 시약인 MediaceTM TPLA (T. pallidum latex agglutination, Sekisui Chemical Co.; 이하 TPLA)시약이 개발 수입되어 국내에 도입 되었다.
이에 저자들은 Mediace RPR과 TPLA 시약을 국내에서 매 독진단을 위해 많이 이용되는 VDRL, TPHA와 비교하기 위해 건강검진 환자를 대상으로 Mediace RPR과 TPLA의 양성률과 위양성률, 생물학적 위양성률을 평가하였다. 또, 자동화 검사 양 성으로 판정된 환자 검체를 기존의 방법으로 검사하고 결과차이 를 보이는 예들은 확인검사를 시행하여 자동화 검사 양성 결과를 분석하였다.
재료 및 방법
1. 대상2005년 12월부터 2006년 11월까지 동국대일산병원에서 건강검
진을 위해 Mediace RPR을 시행한 3,897예를 연구 대상으로 Mediace RPR의 양성률과 위양성률, 생물학적 위양성률을 산출 하였고, TPLA를 시행한 2,284예를 대상으로 TPLA의 양성률과 위양성률을 산출하였다. 같은 기간에 Mediace RPR 또는 TPLA 검사가 의뢰된 환자 검체 중 하나 또는 모두에서 양성 결과를 보 인 134예를 연구대상으로 다시 전통적인 방법의 VDRL와 TPHA 를 시행하였다. 134예는 남자 62예, 여자 72예였으며, 연령 분포 는 0-84세(중앙값 49세)였다. Mediace RPR과 VDRL 결과의 차이를 보인 예들은 TPLA와 TPHA 검사를 통해 확인하였고, TPLA와 TPHA 결과의 차이를 보인 예들은 recomBlot Tre- ponemal IgG/IgM 검사를 시행하였다. 환자의 병록을 찾아서 임 상 진단과의 상관성을 분석하였다.
2. 자동화 매독 검사법인 Mediace RPR과 TPLA 검사
Mediace RPR 시약과 TPLA 시약을 이용하여 Hitachi 7600 automated chemistry analyzer (Hitachi, Tokyo, Japan)로 측 정하였다. Mediace RPR의 결과치가 1.0 R.U. 이상인 경우와, TPLA의 결과치가 10.0 T.U. 이상인 경우 양성으로 판정하였다.
Mediace RPR 양성인 예는 지질항원이 첨가되어 있지 않고 라텍 스만으로 구성된 시약인 lipid antigen free latex 시약으로 검사 를 시행하였다. 이 검사에서 양성이라면 라텍스에 대한 비특이적 항체의 존재 때문에 결과 양성을 보인 것이므로 음성인 경우만 최 종 양성으로 판정하였다. Mediace RPR lipid antigen free latex 시험 전 양성이었으나, 최종 음성으로 판정된 경우는“위양성”으 로 정의하였다. Mediace RPR 최종 양성 예에서 TPLA 음성인 경우“생물학적 위양성”으로 정의하였다. TPLA 양성인 예는 매 독항원으로 구성된 TPLA 중화시약으로 검사를 시행한 후 다음 의 식으로 계산하여 0.5 이상인 경우 최종 양성으로 판정하였다:
(TPLA 결과-TPLA 중화시험결과)/TPLA 결과. 중화시험 결과 최종 음성으로 판정된 경우는“위양성”으로 정의하였다.
3. VDRL, TPHA 검사
Mediace RPR 또는 TPLA 검사에서 양성을 보인 134예를 대상으로 기존의 검사방법인 VDRL (BD Diagnostics, Franklin Lakes, NJ, USA)과 TPHA (Asanpharm, Seoul, Korea) 검 사를 제조사의 설명서에 따라 시행하였다. VDRL은 희석하지 않 은 검체에서 양성을 보이는 경우 양성으로 판정하였다. TPHA는 1:80 희석에서 육안 관찰하여 적혈구의 응집이 있는 경우 양성으 로 판정하였고, 1:40이나 1:20에서만 양성인 경우는 약양성으로 판정하였다.
4. 매독 항체 검출을 위한IgG/IgM immunoblot 검사 TPLA와 TPHA 결과의 차이를 보인 예들을 대상으로 Re-
comBlot Treponemal IgG/IgM (Mikrogen GmbH, Martin- seried, Germany) 검사를 제조사의 설명서에 따라 진행하였다.
RecomBlot Treponemal IgG/IgM는 T. pallidum 항원인 Tp 47, TmpA, TP 37, TP 17, Tp 15에 대한 IgG 또는 IgM 항체 를 검출하는 western blotting 법이다. 판정은 각 항원 별 항체유 무를 점수로 환산하여 IgG인 경우 2점 이하는 음성, 3-4점은 경 계양성(borderline positive), 5점 이상은 양성으로 판정하였고, IgM의 경우 2점 이하는 음성, 3점은 경계양성, 4점 이상은 양성 으로 판정하였다.
5. 통계처리
Mediace RPR과 VDRL의 결과와 TPLA와 TPHA 결과는 Fisher’s exact test로 비교하였고, Mediace RPR과 TPLA의 결과치는 Mann-Whitney Test로 비교하였다. P<0.05를 통계학 적으로 유의한 차이가 있는 것으로 간주하였다. 통계는 SPSS 11.5 (SPSS, Chicago, USA)를 이용하였다.
결 과
1. Mediace RPR, TPLA의 양성률, 위양성률 및 생물학적 위양성률
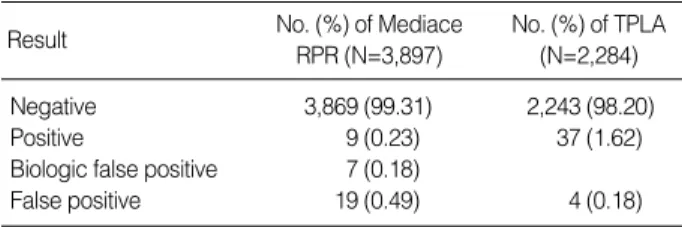
Mediace RPR 검사를 시행한 3,896예에서 양성결과를 보인 28예 중 lipid antigen free latex 검사를 통해 19예가 위양성으 로 판정되어 최종 Mediace RPR 양성률은 0.23% (9/3,896)이
었다. Mediace RPR 최종 양성예에서 TPLA가 음성인 예는 7예 로 판정되어 생물학적 위양성률은 0.18% (7/3,896)였다. Medi- ace RPR과 TPLA 검사 동시 양성률은 0.05% (2/3897)였다.
TPLA의 최종 양성률은 1.62% (37/2284)였다(Table 1).
건강검진으로 Mediace RPR 검사를 시행한 예의 lipid anti- gen free latex 검사 전 양성 중 67.9% (19/28)는 위양성이고 TPLA의 중화시험 전 양성 중 9.8% (4/41)는 위양성이었다.
Mediace RPR 또는 TPLA 양성인 134예 중 Mediace RPR lipid antigen free latex 검사 전 양성은 88예였고 이중 40예가 위양성으로 판정되어 40.9%는 위양성이었다. Mediace RPR 최 종 양성으로 판정된 48예 중 19예는 TPLA 음성으로 39.6%는 생물학적 위양성이었다(Table 2).
2. Mediace RPR과 VDRL결과 비교
Mediace RPR 양성 예의 중앙값은 1.5 R.U. (1-1177.6)였고, 위양성으로 판정된 40예의 lipid antigen free latex 검사 전 중앙 값은 1.3 R.U. (1-9.6)였다(P>0.05). 위양성으로 판정된 40예는 모두 VDRL 음성이었다(Table 3). Mediace RPR 양성이고 TPLA 양성인 29예의 중앙값은 1.8 R.U. (1-1177.6)이고, 생물학 적 위양성을 보인 19예의 중앙값은 1.3 R.U. (1-2.3)였다(P=0.03).
24.6% (33/134)는 Mediace RPR과 VDRL 결과가 일치하지 않았다(P<0.05). Mediace RPR 음성이고 VDRL 양성인 2예는 모두 TPLA와 TPHA 양성이었다. Mediace RPR 양성이고 VDRL 음성인 31예 중 13예는 TPLA 양성이고 나머지는 음성 이었고, 14예는 TPHA 양성이고 나머지는 음성이었다.
Result No. (%) of Mediace
RPR (N=3,897)
No. (%) of TPLA (N=2,284)
Negative 3,869 (99.31) 2,243 (98.20)
Positive 9 (0.23) 37 (1.62)
Biologic false positive 7 (0.18)
False positive 19 (0.49) 4 (0.18)
Table 1.Positive rates of Mediace RPR and TPLA
Abbreviations: RPR, Rapid Plasma Reagin; TPLA, Treponema pallidum Latex Agglutination.
Mediace RPR result
No. of cases with indicated TPLA result Negative False positive Positive Total
Negative 0 4 42 46
False positive 34 4 2 40
Positive 19 0 29 48
Total 53 8 73 134
Table 2.Comparison of Mediace RPR and TPLA results
Abbreviations: RPR, Rapid Plasma Reagin; TPLA, Treponema pallidum Latex Agglutination.
VDRL result No. of cases with indicated Mediace RPR Result Negative False positive Positive Total
Negative 44 40 31 115
Positive 2 0 17 19
Total 46 40 48 134
Table 3.Comparison of VDRL and Mediace RPR results
Abbreviations: RPR, Rapid Plasma Reagin; VDRL, Venereal Disease Research Laboratory.
TPHA result No. of cases with indicated TPLA result Negative False positive Positive Total
Negative 51 8 5 64
Weak positive 2 0 5 7
Positive 0 0 63 63
Total 53 8 73 134
Table 4.Comparison of TPHA and TPLA results
Abbreviations: TPLA, Treponema pallidum Latex Agglutination; TPHA, Treponema pallidum hemmagglutination assay.
3. TPLA와 TPHA결과 비교
TPLA 양성 예들의 중앙값은 73.5 T.U. (10-12800)였고, TPLA 중화시험 결과 위양성으로 판정된 8예의 중화시험 전 중 앙값은 55.5 T.U. (15-252)였다(P>0.05). 위양성으로 판정된 8 예는 모두 TPHA 음성이었다(Table 4). TPLA 양성 73예 중 5예는 매독으로 진단된 예였고, 8예는 치료된 매독이었고, 18예는 매독이 의심되는 예였고, 43예는 기타 진단이었다.
5.2% (7/134)에서 TPLA와 TPHA 결과가 일치하지 않았다 (P<0.05).
4. TPLA와 TPHA 결과에 차이를 보인 예의IgG/IgM immunoblot 결과
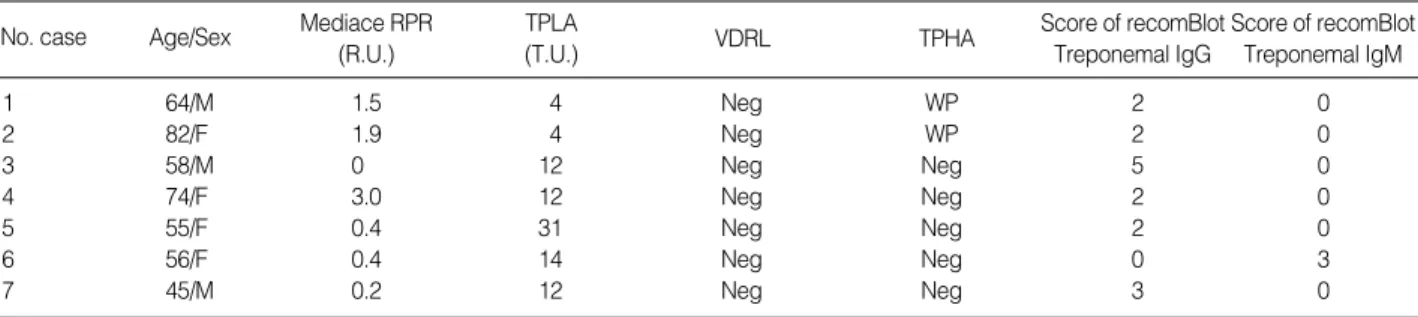
TPLA와 TPHA 검사 결과의 차이를 보인 7예 중 매독의 임 상적 증거와 과거력이 있는 예는 없었다. Mediace RPR 양성, TPLA 음성이고 TPHA 양성인 2예는 recomBlot Treponemal IgG/IgM 음성이었다(Table 5). TPLA 양성이고 TPHA 음성 인 5예에서 2예는 recomBlot Treponemal IgG 결과 양성이었고, 한 예는 recomBlot Treponemal IgM 양성이었다.
고 찰
국내 매독 양성률은 연구 대상에 따라 다른 결과를 보이고 있는 데, 1997년에서 1998년 사이 헌혈자의 매독항체 양성률은 0.08%
이고, 2000년에 헌혈자와 임산부, 건강검진 환자를 대상으로 한 매독검사 양성률은 0.2%로 보고되고 있다[1, 6]. VDRL, card RPR 등의 시약에 이용되는 항원의 정제기술이 발전하였지만, 비 트레포네마검사는 여러 만성감염과 자가면역 질환 등에서 5-30%
의 생물학적 위양성을 보인다[7]. Mediace RPR 검사의 생물학 적 위양성률은 보고된 위양성률 보다 높은 39.6% (19/48)였다.
이번 연구에서 매독의 유병률이 낮은 건강검진과 수술 전 매독검 사에서 양성을 보인 예가 주로 연구 대상에 포함되었고, 이처럼
유병률이 낮은 대상군에서는 양성 예측률이 낮기 때문에 생물학적 위양성률이 높게 산출된 것으로 생각된다[9]. 건강검진 환자 전 체를 대상으로 한 생물학적 위양성률은 0.18% (7/3897)로 이는 VDRL의 생물학적 위양성률인 0.24%와 크게 차이가 없었다[8].
건강검진 환자에서의 Mediace RPR 위양성률은 최초 양성의 67.9%인데 반해 전체 양성 환자에서의 위양성률은 40.9%였다.
건강검진환자의 Mediace RPR과 TPLA 동시 양성률이 0.05%
로 낮아, 유병률이 낮은 대상군에서는 양성예측률이 낮아지는 것 과 같은 의미로 해석된다[9]. 그러므로, 특히 유병률이 낮은 군을 대상으로 Mediace RPR 검사로 선별검사를 시행할 때에는 라텍 스에 반응하는 비특이적 항체에 의한 검사 양성을 감소 시키기 위해 lipid antigen free latex 시약을 이용한 검사가 필요하다.
비트레포네마 검사 양성환자의 확진검사로 이용되는 트레포네마 검사인 TPLA 위양성률도 건강검진환자 양성 중 9.8%이므로 TPLA 중화시험도 필요한 것으로 생각된다.
VDRL 검사의 일차매독 민감도는 89-87%, 말기매독에서는 37-94%이고 특이도는 98.7-99.5%로 보고되고 있다[10, 11]. 본 연구에서 Mediace RPR 검사의 민감도와 특이도를 산출하지는 못했지만, TPLA를 기준으로 두 검사를 비교했을 때 Mediace RPR 양성이고 VDRL 음성인 31예 중 13예는 TPLA 양성이었 고 18예는 음성이었다. 연구 대상을 선택한 기준이 Mediace RPR 양성 검체였기 때문에 Mediace RPR 양성이고 VDRL 음 성인 예가 많은 것으로 추측된다. 결과에 제시하지는 않았지만, VDRL 양성인 검체를 대상으로 Mediace RPR 검사를 시행했을 때 VDRL 양성인 21예 중 15예가 Mediace RPR 음성 이었으므 로 선별검사로 이용되는 비트레포네마검사인 두 검사 중 어떤 검 사가 우수하다고 결론내기는 어렵고, 양성 결과를 보였을 때 트 레포네마검사로 확진검사를 시행하는 것이 필요하다.
FTA-ABS 검사가 확진검사의 gold standard로 여겨지지만, 위양성의 위험이 있고 IgG 검사의 경우 초기 매독에서 20%의 위음성 가능성이 보고되고 있어, 또 다른 확인검사로 western blot법이 제시되고 있다[12-15]. 본 연구에서는 TPLA와 TPHA 결과의 차이를 보이는 7예의 확인을 위해 recomBlot Trepone- mal IgG/IgM를 이용하였다. RecomBlot Treponemal IgG/IgM We interpretive as positive for Mediace RPR and TPLA when the values above the cutoff, 1.0 R.U. and 10 T.U., respectively.
Abbreviations: RPR, Rapid Plasma Reagin; TPLA, Treponema pallidum Latex Agglutination; VDRL, Venereal Disease Research Laboratory; TPHA, Treponema pallidum hemmagglutination assay; Pos, positive; Neg, negative; WP, weakly positive.
No. case Age/Sex Mediace RPR (R.U.)
Score of recomBlot Treponemal IgG
Score of recomBlot Treponemal IgM TPLA
(T.U.) VDRL TPHA
1 64/M 1.5 4 Neg WP 2 0
2 82/F 1.9 4 Neg WP 2 0
3 58/M 0 12 Neg Neg 5 0
4 74/F 3.0 12 Neg Neg 2 0
5 55/F 0.4 31 Neg Neg 2 0
6 56/F 0.4 14 Neg Neg 0 3
7 45/M 0.2 12 Neg Neg 3 0
Table 5.Detailed results of discrepant samples on TPLA and TPHA
법의 시약은T. pallidum의 항원들 중 항원성이 강해 매독 진단 에 있어 중요한 역할을 하는 47, 17, 15 kDa의 분자량을 갖는 지 단백인 TP 47, TP 17, TP 15와[10], TmpA, Tp 37 항원들로 구성되어 있다. Western blot 법의 민감도는 93.8%, 특이도는 100%로 보고되고 있다[10, 14]. TPLA 양성이면서 TPHA 음 성인 5예 중 한 예는 Tp 47 IgG 항체 양성이었고, 한 예는 IgM 항체 양성이었다. Tp 47에 대한 항체는 초기매독에서 양성을 보 이고 치료 후 음성으로 전환될 가능성이 높은 항체로, TPLA 검 사는 주로 Tp 47을 주 항원으로 이용하고 있으므로 TPLA 양성, TPHA 음성의 결과를 보인 2예의 설명이 가능하다[16]. TPLA 와 TPHA 결과 차이를 보인 7예 모두 매독의 임상적 증거와 과 거력은 없었기 때문에 임상 진단을 기준으로 판단하기는 어려웠지 만, recomBlot Treponemal IgG/IgM 검사 결과와 비교해 보았 을 때(Table 5), 5예에서 TPLA와 recomBlot Treponemal IgG/
IgM는 일치하는 결과를 보였으므로 TPLA는 TPHA에 비해 확 진검사로써의 우수성을 갖는 것으로 생각된다.
Mediace RPR, TPLA 검사의 결과값들을 이용하여 위양성과 생물학적 위양성을 구분할 수 있을지 확인하였다. Mediace RPR 과 TPLA의 양성군과 위양성군의 값 차이는 없었다. Mediace RPR 양성이고 TPLA 양성인 예의 중앙값은 1.8 R.U. (1-1,177.6), 생물학적 위양성을 보인 예의 중앙값은 1.3 R.U. (1-2.3)로 생물 학적 위양성일 때 의미 있게 낮은 값을 보였다(P=0.03). 그러므 로 위양성이 배제된다면 Mediace RPR 결과치가 높은 환자는 TPLA 양성 매독의 가능성이 높음을 시사한다.
결론적으로, Mediace RPR의 생물학적 위양성률은 보고된 VDRL의 생물학적 위양성률과 큰 차이가 없었지만, Mediace RPR은 라텍스에 대한 비특이 결합에 의해 발생하는 위양성의 가 능성이 있으므로 Mediace RPR 양성 결과를 보이는 검체에 대 해서는 lipid antigen free latex 시약을 이용해 위양성 유무를 확 인하고, TPLA 양성 결과를 보이는 검체에 대해서는 TPLA 중 화시험을 시행해야 할 것으로 생각된다. TPLA와 TPHA 결과 차이를 보이는 예들의 확인검사에서 새로운 자동화 검사법이 TP- HA보다 recomBlot Treponemal IgG/IgM과 일치도가 높았다.
또한, Mediace RPR과 TPLA는 선별검사 목적의 대량검사 수 행이 가능하고, 정량적 측정이 가능하고, 감염의 위험이 적고, 검 사자간 결과 판독의 차이를 보이지 않는 장점을 가지고 있는 유 용한 검사로 생각된다.
요 약
배경 : 최근 자동화장비로 검사 가능한 Mediace Rapid plas- ma reagin (RPR), Treponema pallidum latex agglutination (TPLA) (Sekisui, Japan)법이 소개되었다. Mediace RPR과 TPLA의 양성률과 생물학적 위양성률을 알아보고, Mediace RPR 또는 TPLA 양성 검체를 대상으로 VDRL과 TPHA 결과와 비
교 평가하였다.
방법 : 2005년 12월부터 2006년 11월까지 건강검진 검사로 Mediace RPR과 TPLA 검사를 시행한 3,896예를 대상으로 Me- diace RPR의 생물학적 위양성률, 양성률과 TPLA의 양성률을 구하였다. 같은 기간 Mediace RPR 또는 TPLA 양성인 134예 를 대상으로 VDRL 및 TPHA 검사를 시행하였다. TPLA와 TPHA 검사결과의 차이가 있는 경우 recomBlot Treponemal IgG/IgM (Mikrogen GmbH, Germany)를 시행하였다. Medi- ace RPR과 TPLA는 Hitachi 7600 chemistry autoanalyzer (Hitachi, Japan)로 검사하였다. Mediace RPR 양성이고 TPLA 음성이 경우 생물학적 위양성으로 정의하였다.
결과 : Mediace RPR 양성률은 0.23% (9/3,896)이고, 생물학 적 위양성률은 0.18% (7/3,896)이었다. TPLA 양성률은 1.62%
(37/2,284)이었다. Mediace RPR 또는 TPLA 양성 134예 중 33예(24.6%)는 VDRL과 Mediace RPR 결과의 차이를 보였다.
이 중 Mediace RPR(+)/VDRL(-)인 31예 중 13예는 TPLA 양성이었고, 18예는 TPLA 음성이었다. TPLA와 TPHA 결과의 차이를 보였던 7예 중 TPLA(-)/TPHA(+)인 2예는 recomBlot Treponemal IgG/IgM 음성이었고, TPLA(+)/TPHA(-)인 5 예 중 3예는 recomBlot Treponemal IgG/IgM 양성이었다.
결론 : TPLA와 TPHA 비교 결과 차이를 보이는 예들의 확 인검사에서 TPLA 결과는 recomBlot Treponemal IgG/IgM 결과와 일치도가 높았다. 또한, Mediace RPR과 TPLA는 대량 검사 수행이 가능한 정량적 측정법이고, 자동화 검사로서 감염의 위험이 적고, 검사자간 결과 판독의 차이를 보이지 않는 장점을 가지고 있는 검사로 생각된다.
참고문헌
1. Cho YH, Kim HO, Lee JB, Lee MG. Syphilis prevalence has rapidly decreased in South Korea. Sex Transm Infect 2003;79:323-4.
2. Clyne B and Jerrard DA. Syphilis testing. J Emerg Med 2000;18:361-7.
3. Egglestone SI and Turner AJ. Serological diagnosis of syphilis. PHLS Syphilis Serology Working Group. Commun Dis Public Health 2000;
3:158-62.
4. Larsen SA, Steiner BM, Rudolph AH. Laboratory diagnosis and interpretation of tests for syphilis. Clin Microbiol Rev 1995;8:1-21.
5. Wheeler HL, Agarwal S, Goh BT. Dark ground microscopy and treponemal serological tests in the diagnosis of early syphilis. Sex Transm Infect 2004;80:411-4.
6. Seo DH, Lee YR, Oh YC, Kim DJ. Study on serologic test for syphilis as a surrogate marker for human immunodeficiency virus infection among Korean blood donors. Korean J Blood Transfus 2001;12:231- 6.(서동희, 이용래, 오영철, 김동집. 국내헌혈자에서매독검사의 HIV 감 염대리표지자에관한연구. 대한수혈학회지 2001;12:231-6.)
7. Kirchner JT. Syphilis--an STD on the increase. Am Fam Physician 1991;44:843-54.
8. Geusau A, Kittler H, Hein U, Dangl-Erlach E, Stingl G, Tschachler E. Biological false-positive tests comprise a high proportion of Vene- real Disease Research Laboratory reactions in an analysis of 300,000 sera. Int J STD AIDS 2005;16:722-6.
9. Diaz T, Almeida MG, Georg I, Maia SC, De Souza RV, Markowitz LE. Evaluation of the Determine Rapid Syphilis TP assay using sera.
Clin Diagn Lab Immunol 2004;11:98-101.
10. Byrne RE, Laska S, Bell M, Larson D, Phillips J, Todd J. Evaluation of a Treponema pallidum western immunoblot assay as a confirma- tory test for syphilis. J Clin Microbiol 1992;30:115-22.
11. Larsen SA, Hambie EA, Pettit DE, Perryman MW, Kraus SJ. Speci- ficity, sensitivity, and reproducibility among the fluorescent trepo- nemal antibody-absorption test, the microhemagglutination assay for Treponema pallidum antibodies, and the hemagglutination tre-
ponemal test for syphilis. J Clin Microbiol 1981;14:441-5.
12. Calonge N, U.S. Preventive Services Task Force Screening for sy- philis infection: recommendation statement. Ann Fam Med 2004;
2:362-5.
13. Johnson PC and Farnie MA. Testing for syphilis. Dermatol Clin 1994;12:9-17.
14. Backhouse JL and Nesteroff SI. Treponema pallidum western blot:
comparison with the FTA-ABS test as a confirmatory test for syphilis.
Diagn Microbiol Infect Dis 2001;39:9-14.
15. Hagedorn HJ, Kraminer-Hagedorn A, De Bosschere K, Hulstaert F, Pottel H, Zrein M. Evaluation of INNO-LIA syphilis assay as a con- firmatory test for syphilis. J Clin Microbiol 2002;40:973-8.
16. Dang Q, Feng J, Lu X, Zhang X, Xu H, Liu C, et al. Evaluation of specific antibodies for early diagnosis and management of syphilis.
Int J Dermatol 2006;45:1169-71.