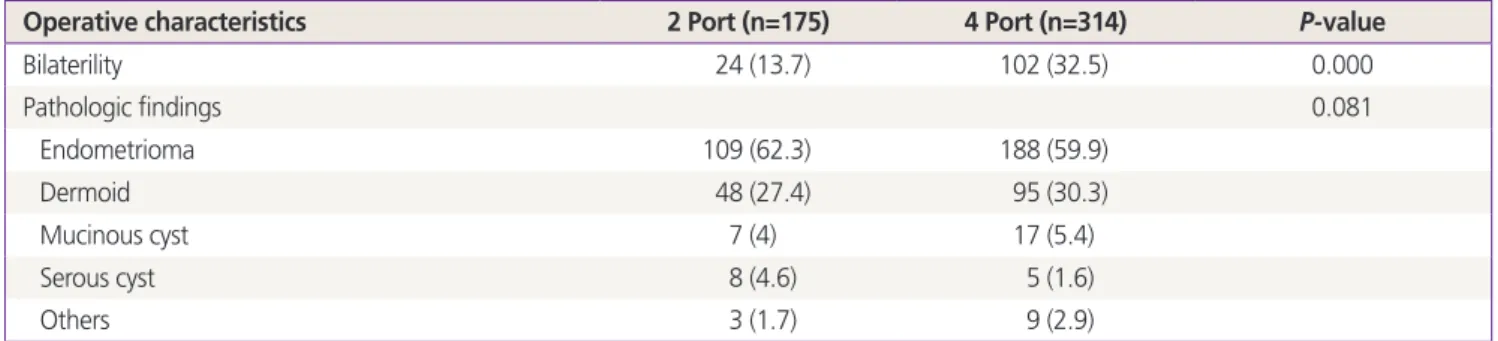
Two-port access versus four-port access laparoscopic ovarian cystectomy
7
0
0
전체 글
(2)
(3)
(4)
(5)
(6)
(7)
수치

관련 문서
Notably, Ser729 phosphorylation on PKCε, an indicator of active PKCε, decreases following overnight treatment with ETO or with PKCε-i (Figure 3D), suggesting that the effect of
In addition, to investigate whether the difference in differentiation patterns between wild-type and Dab1 −/− cells was due to a loss of Reelin- Dab1 signaling, we
To determine whether LAG3 mediates the pathology induced by human α-syn PFF, we assessed P-α-syn immunoreactivity in cortical cultures from mouse prion promoter
In this study, primary activity is defined as input (seed, fertilizer, pesticide, agricultural machinery, etc.), production (land access, production base,
In this study, primary activity is defined as input (seed, fertilizer, pesticide, agricultural machinery, etc.), production (land access, production base,
Fig. Security Threats in Cloud Environments.. completely removed when the user leaves the existing cloud environment [4-12]. A user who has left creates a problem if he /
Postoperative adhesion formation and reproductive outcome using interceed ® after ovarian surgery: a randomized trial in the rabbit model.. Adhesion reformation
Patient had laparoscopic surgery on the adnexal tumor and excised tissue was removed through Douglas pouch incision by single surgeon.. Results: The mean age
