963
The Association of Metabolic Syndrome and Prostate-Specific Antigen
Young Eun Yoon, Jae Won Lee, Seok Young Lee, Kyoung Taek Lim, Sung Yul Park, Yong Tae Kim, Tchun Yong Lee, Hae Young Park From the Department of Urology, Hanyang University College of Medicine, Seoul, Korea
Purpose: Recent studies have reported the association between metabolic syndrome and benign prostatic hyperplasia. This study was conducted to evaluate the relation between metabolic syndrome and prostate-specific antigen (PSA).
Materials and Methods: From January 2004 to December 2007, a total of 4,115 male outpatients (aged 40 to 79 years) who visited the health care center at our medical center were examined. Eligible men were classified according to the presence or absence of metabolic syndrome and the number of components of the metabolic syndrome. The association between the sum of metabolic syndrome components and PSA level was evaluated. The association between each metabolic syndrome component and PSA level was also evaluated.
Results: The PSA level of metabolic syndrome patients was lower than that of the control group (p=0.022). An increased number of metabolic syndrome components was significantly associated with a linear, decreas- ing trend in PSA levels (p-trend=0.040). When a Pearson's correlation was performed, only obesity was inversely associated with PSA level in the metabolic syndrome group. There was no significant factor that was related to having a PSA level greater than or equal to 2.5 ng/ml.
Conclusions: Metabolic syndrome should be considered as a factor associated with reduced PSA levels. If the patient with metabolic synd- rome is obese, the PSA cutoff value should be lower than 4 ng/ml. (Korean J Urol 2009;50:963-968)
Key Words: Prostate-specific antigen, Metabolic syndrome X, Obesity
Korean Journal of Urology Vol. 50 No. 10: 963-968, October 2009
DOI: 10.4111/kju.2009.50.10.963
한양대학교 의과대학 비뇨기과학교실 윤영은ㆍ이재원ㆍ이석영
임경택ㆍ박성열ㆍ김용태 이춘용ㆍ박해영
Received:March 30, 2009 Accepted:September 10, 2009 Correspondence to: Hae Young Park
Department of Urology, Hanyang University College of Medicine, 17, Hangdang-dong, Seongdong-gu, Seoul 133-792, Korea
TEL: 02-2290-8598 FAX: 02-2299-2186
E-mail: haeypark@hanyang.ac.kr
Ⓒ The Korean Urological Association, 2009
서 론
혈중 전립샘특이항원 (prostate-specific antigen; PSA)은 전 립샘암 선별검사에 쓰이는 종양표지자이다. PSA의 세계적 인 활용은 전립샘암의 조기 발견 및 치료에 막대한 영향을 가져왔다. 그러나 PSA 수치가 높은 환자에서도 전립샘암이 발견되지 않을 가능성이 있어 PSA 검사의 특이도를 높이기 위한 많은 연구들이 진행 중이다. PSA 수치는 전립샘 질환 뿐만 아니라 인종, 나이 등을 포함하여 많은 인자의 영향을 받는 것으로 알려져 있다 [1]. PSA 수치에 영향을 주는 인자
에 대한 연구는 PSA 검사의 활용성을 좀 더 높여줄 것으로 기대된다.
인슐린 저항성과 고인슐린혈증이 특징인 대사증후군은 제2형 당뇨, 고혈압, 비만, 이상지혈증으로 정의한다. 인슐 린 매개성 포도당 흡수장애로 인한 인슐린 저항성에 따른 2차적 고인슐린혈증 및 교감신경계의 과활성이 대사증후 군의 기본 병태생리이다. 최근 식습관 및 생활 방식이 서구 화 되어 대사증후군 환자가 늘어나면서 대사증후군이 사회 적 문제로 떠오르고 있다.
활성된 교감신경은 하부요로증상을 유발하여 [2], 최근 전립샘비대증과 대사증후군의 상관성에 관한 연구가 활발
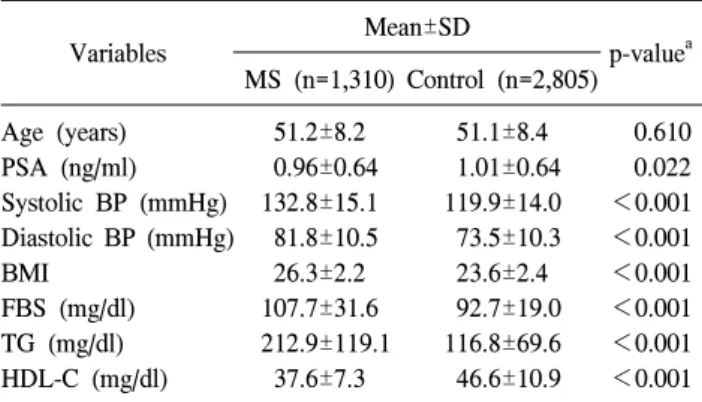
Table 1. Comparison of PSA levels and metabolic syndrome components between those who had the metabolic syndrome and those who did not
Variables Mean±SD
p-valuea MS (n=1,310) Control (n=2,805) Age (years)
PSA (ng/ml) Systolic BP (mmHg) Diastolic BP (mmHg) BMI
FBS (mg/dl) TG (mg/dl) HDL-C (mg/dl)
51.2±8.2 0.96±0.64 132.8±15.1 81.8±10.5 26.3±2.2 107.7±31.6 212.9±119.1
37.6±7.3
51.1±8.4 1.01±0.64 119.9±14.0 73.5±10.3 23.6±2.4 92.7±19.0 116.8±69.6 46.6±10.9
0.610 0.022
<0.001
<0.001
<0.001
<0.001
<0.001
<0.001 PSA: prostate- specific antigen, SD: standard deviation, MS:
metabolic syndrome, BP: blood pressure, BMI: body mass index, FBS: fasting blood sugar, TG: triglyceride, HDL-C: high-density lipoprotein cholesterol, a: Student's t-test
히 진행되고 있다. 국내 연구 결과로 대사증후군이 전립샘 용적을 증가시키고, 전립샘비대증 환자들의 하부요로 증상 을 악화시킨다는 보고가 있었다 [3,4]. 최근 대사증후군과 PSA 수치와의 연관성에 대한 보고들이 있었으나 [5,6], 이 들 논문의 대부분이 연구 대상을 선정하는데 있어 대사성 인자에 영향을 줄 수 있는 심혈관계 약물 복용력이나, 고지 혈증, 당뇨 등의 치료 여부를 고려하지 않았다는 지적을 받 고 있다. 또한 대사증후군인 환자와 그렇지 않은 환자에서 대사성 인자가 PSA에 미치는 영향의 차이점에 대한 연구는 발표된 바 없다. 이에 건강검진센터를 방문한 성인 남성에 서 대사증후군의 구성 요소들과 PSA 수치가 어떤 상관관계 가 있는지 알아보았다.
대상 및 방법 1. 대상
2004년 1월부터 2007년 12월까지 본원 건강검진센터를 방문한 40세 이상의 성인 남성 6,329명을 대상으로 하였다.
그 중 대사증후군의 판단에 영향을 줄 수 있는 당뇨, 고혈 압, 고지혈증 및 심혈관계질환의 병력으로 치료받았던 경 우 대상에서 제외하였고, PSA 검사에 영향을 줄 수 있는 전립샘 관련 수술이나 치료를 받은 경력이 있는 경우를 제 외하였다. 또 PSA 수치가 4 ng/ml 이상인 경우 조사 대상에 서 제외하였다. 총 연구 대상은 4,115명이었으며, 평균연령 은 51.1±8.3세였다.
2. 방법
대사증후군의 진단 기준은 2001년 5월 발표된 National Cholesterol Education Programme Adult Treatment Panel III (NCEP-ATP III)의 기준 인자에 따라 1) 고혈압 (수축기 혈압 이 130 mmHg 이상 혹은 이완기 혈압 85 mmHg 이상), 2) 비만 (허리둘레가 90 cm 이상이거나 신체질량지수 (body mass index; BMI)가 25 kg/m2 이상), 3) 내당능 장애 (공복 시 혈당이 110 mg/dl 이상), 4) 고중성지방혈증 (150 mg/dl 이상), 5) 저HDL 콜레스테롤혈증 (45 mg/dl 미만)인 경우 중 세 가지 이상의 인자가 양성인 경우 대사증후군으로 진단 하였다 [7]. 본 연구에서는 측정의 편의를 위하여 허리둘레 대신 BMI를 이용하였다.
모든 조사 대상의 PSA 검사는 monoclonal immunora- diometric assay (Tandem-R PSA assay, Hybritech, Inc. San Diego, USA)로 측정하였고, 대사증후군 관련 지표로 신장, 체중, 혈압, 공복 혈당, 중성지방, HDL-C를 측정하였다. 각 군의 PSA 평균을 비교하였고, PSA 수치와 각각의 인자들 간의 상관관계에 대하여 조사하였다. 대사성 인자의 합에
따른 PSA 수치의 변화를 살펴보았으며, PSA 수치가 2.5 ng/ml 이상인 군을 따로 분류하여 대사성 인자들과의 상관 관계를 분석하였다.
3. 통계분석
모든 데이터는 평균±표준편차로 표시하였으며 통계 분 석은 WindowsⓇ용 Stastical Package for Social Science 15.0 (SPSS 15.0)을 사용하였다. 각 군의 대사성 인자와 PSA 수 치의 평균을 비교하기 위해 Student's t-test를 시행하였으며, 대사성 인자들의 합에 따른 PSA 수치의 차이를 보기위해 ANOVA를 시행하였다. PSA 수치와 각각의 대사성 인자들 간의 상관관계를 비교하기 위하여 Pearson's correlation을 사 용하였다. 각 군에서 PSA 수치가 2.5 ng/ml 이상인 군의 비 율은 chi-square test를 이용하여 비교하였으며, PSA 수치가 2.5 ng/ml 이상일 가능성에 대한 인자들의 분석은 단변량 로지스틱 회귀분석을 시행하였다. 모든 통계값은 p값이 0.05 미만인 경우 통계학적으로 유의한 것으로 판단하였다.
결 과
1. 대사증후군과 대조군의 평균 혈중 PSA 수치
전체 4,115명 중 대사증후군은 1,310명, 정상 대조군은 2,805명이었다. 대사증후군과 정상대조군의 평균 연령은 각 각 51.2±8.2세와 51.1±8.4세로 큰 차이가 없었다 (p=0.610).
전체 평균 PSA 수치는 0.99±0.64 ng/ml였고, 대사증후군은 0.96±0.64 ng/ml, 정상 대조군이 1.01±0.64 ng/ml로 대조군에 서 유의하게 낮았다 (p=0.022) (Table 1).
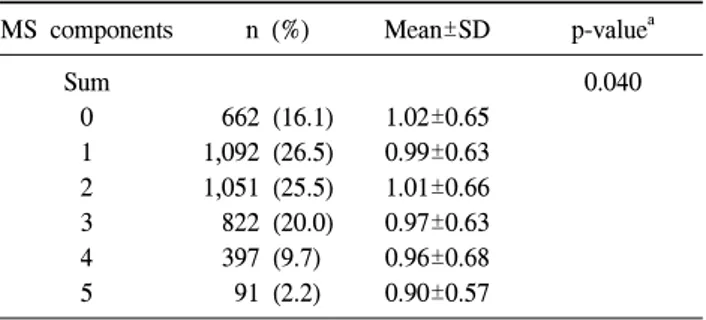
Table 2. PSA levels with sum of metabolic syndrome components MS components n (%) Mean±SD p-valuea
Sum 0 1 2 3 4 5
662 (16.1) 1,092 (26.5) 1,051 (25.5) 822 (20.0) 397 (9.7) 91 (2.2)
1.02±0.65 0.99±0.63 1.01±0.66 0.97±0.63 0.96±0.68 0.90±0.57
0.040
PSA: prostate-specific antigen, MS: metabolic syndrome, SD:
standard deviation, a: ANOVA
Table 3. Correlation between metabolic syndrome components and PSA level
Variables MS (n=1,310) Control (n=2,805) ra p-value ra p-value Hypertension
Obesity Hyperglycemia Hypertriglyceridemia Reduced levels of HDL-C
0.021
−0.078 0.006
−0.008 0.026
0.449 0.005 0.827 0.773 0.344
0.034
−0.036
−0.005
−0.012 0.018
0.071 0.059 0.798 0.519 0.346 PSA: prostate-specific antigen, MS: metabolic syndrome, HDL-C:
high-density lipoprotein cholesterol, a: Pearson's correlation co- efficient
Table 4. Univariate logistic regression analysis of metabolic syndrome components predicting a PSA level greater than or equal to 2.5 ng/ml
Variablesa
MS Control
Odds ratio
(95% CI) p-value Odds ratio (95% CI) p-value
Hypertension 1.522
(0.802-2.887) 0.199 1.289
(0.829-2.002) 0.259
Obesity 0.505
(0.278-0.919) 0.025 0.879
(0.553-1.396) 0.584
Hyperglycemia 1.050
(0.580-1.903) 0.871 0.872
(0.377-2.017) 0.750 Hypertriglyceridemia 0.930
(0.480-1.799) 0.828 0.701
(0.396-1.240) 0.222 Reduced levels of
HDL-C
3.189
(0.767-13.252) 0.111 1.186
(0.805-1.746) 0.388 PSA: prostate-specific antigen, MS: metabolic syndrome, CI:
confidence interval, HDL-C: high-density lipoprotein cholesterol, a: absent or present
2. 대사성 인자와 PSA 수치의 상관성
1) 대사성 인자의 합과 PSA 수치: 전체를 대상으로 대사성 인자들의 합과 PSA 수치의 상관관계를 분석한 결과 대사성 인자의 합이 1인 경우보다 2인 경우의 PSA 수치가 조금 높 았다 (0.99±0.63 vs. 1.01±0.66). 그러나 대사성 인자의 합이 0인 군의 평균 PSA가 1.02±0.65, 5인 군의 PSA가 0.90±0.57 로 전체적으로는 대사성 인자의 합이 증가함에 따라 PSA 수치가 낮아지는 경향을 보였다 (p=0.040) (Table 2).
2) 각각의 대사성 인자와 PSA 수치: 각각의 대사성 인자와 PSA 수치의 상관관계를 분석한 결과 대사증후군에서 비만과 PSA 수치가 통계적으로 유의한 상관관계가 있었고 (p=0.005), 이들의 상관계수 (r)은 −0.078로 음의 상관관계였다 (Table 3).
고중성지방혈증도 음의 상관관계였지만, 상관계수가 상대 적으로 작았으며 (r=−0.008), 통계적으로 유의하지 않았다 (p=0.773). 대조군에서는 비만과 PSA의 상관계수가 음이었 지만 (r=−0.036), 통계적으로 유의하지 않았다 (p=0.059).
3) PSA 수치가 2.5 ng/ml 이상인 군과 대사성 인자의 상관성:
대사증후군과 대조군에서 PSA 수치가 2.5 ng/ml 이상인 군 의 비율은 각각 3.9% (51명)와 3.8% (107명)로 두 군 간에
차이가 없었다 (p=0.931). 각 군에서 PSA 수치가 2.5 ng/ml 이상일 경우를 대사성 인자들과 단변량 로지스틱 선형회귀 모형으로 분석한 결과 대사증후군에서 비만만이 odds ratio 가 0.505 (0.278-0.919, p=0.025)로 유의하였다 (Table 4).
고 찰
고혈압, 당뇨, 이상지방혈증, 비만 등 관상동맥질환의 위 험요인이 되는 질환들이 함께 나타나는 것을 대사증후군이 라 정의한다 [8]. 2005년 미국에서 발표된 자료에 의하면 NCEP-ATP III 기준에 따른 대사증후군의 유병률이 34.6%
였고 [9], 우리나라는 같은 기준에서 28%로 보고하고 있다 [10]. 본 연구에서도 대사증후군이 전체 조사 대상의 31.8%
로 이와 유사하였다. 그러나 우리나라에서도 식습관 및 생 활 습관의 서구화와 고령화 현상으로 인해 대사증후군 유 병률이 증가하는 추세이다 [10].
전립샘의 성장과 전립샘비대증 그리고 전립샘암은 현재 까지의 연구에서 비만을 비롯한 대사증후군의 요소들과 어 느 정도 관련성이 있는 것으로 보인다. Hammarsten 등은 대 사증후군의 구성요소들이 전립샘비대증의 위험 인자라고 처음 보고하였으며 [11], Parsons 등은 BMI 및 상승된 공복 혈당과 당뇨병의 유무가 전립샘 용적과 상관이 있다고 보 고하였다 [12]. 또 Kim 등은 전립샘의 용적이 나이, 체표면 적 (body surface area; BSA), PSA 수치와 양의 상관관계를 보이며, HDL-C와는 음의 상관관계가 있다고 하였다 [13].
PSA 검사는 전립샘암을 진단하거나, 진단된 전립샘암의
치료 효과를 판정하기 위해 널리 사용하고 있다. 그러나 PSA 수치는 전립샘 질환 이외에 여러 가지 요인들에 의해 영향을 받을 수 있어 PSA 검사의 정확성에 대한 논의가 끊 이지 않고 있다. 당뇨나 대사증후군이 있는 남성은 혈중 테 스토스테론이 낮으며 [14], 혈중 테스토스테론이 낮은 남성 은 당뇨나 대사증후군의 발병률이 높다고 한다 [15]. 낮은 혈중 테스토스테론은 PSA 수치를 낮출 것으로 여겨지나, 반면에 대사증후군이 대조군에 비해 전립샘용적만이 크며 두 군 간의 PSA 수치는 차이가 없다는 연구 결과도 있다 [3,13]. 본 연구에서는 대사성 인자가 많을수록 PSA 수치가 낮아지고, 대조군보다 대사증후군의 PSA 수치가 낮았다.
이 결과는 Kim 등의 연구 결과와 일치하였다 [5].
고혈압은 혈중 테스토스테론을 감소시킨다 [16]. 낮은 혈 중 테스토스테론은 전립샘의 성장을 억제하여 혈중 PSA 수 치를 감소시킬 수 있다. 그러나 Han 등은 고혈압 환자의 낮 은 성호르몬은 동맥강직을 유발하므로 PSA 수치와 이완기 혈압이 양의 상관관계를 갖는다고 하였다 [6]. 그러나, 고혈 압은 PSA 수치와 아무 관계가 없다는 보고도 있다 [5]. 본 연구에서도 고혈압은 대사증후군과 대조군 모두에서 PSA 와 상관성이 없었다. Zmuda 등은 고중성지방혈증과 저HDL 콜레스테롤혈증이 낮은 혈중 테스토스테론과 연관이 있다 고 하였고 [17], Duell과 Biermon은 혈중 HDL 콜레스테롤이 혈중 테스토스테론과 양의 상관관계가 있다고 하였지만 [18], PSA 수치와 HDL 콜레스테롤이 음의 상관관계가 있다 는 보고도 있다 [6]. 본 연구에서 이상지혈증의 여부는 PSA 수치와 관계가 없었는데, 전립샘에 대한 이상지혈증의 영 향은 제한적일 것으로 생각한다. Werny 등은 당뇨 환자에 서 PSA 수치가 21.6% 낮으며 이 차이는 이환 기간과 비례 하여, 당뇨로 진단받은 후 10년이 지난 환자에서는 27.5%의 감소가 있음을 보고하였다 [19]. 이는 당뇨 환자에서 성호 르몬결합글로블린 (sex hormone-binding globulin; SHBG)이 낮기 때문으로 [20], 몇몇의 연구에서도 공복 혈당이 PSA 수치와 음의 상관관계가 있다고 발표된 바 있다 [6,21]. 본 연구의 분석 결과 내당능장애는 유의한 상관성을 보이지 않아 추후 이에 대한 연구가 필요할 것으로 생각한다.
PSA 검사의 정확성을 증대하기 위해 많은 인자들이 거론 되고 있는데, 최근에는 PSA 수치와 비만이 음의 상관관계 가 있다고 보고하는 연구들이 있다. Sohn 등은 건강증진센 터를 방문한 26,193명의 hospital based study에서 나이에 상 관없이 BMI와 PSA 수치는 음의 상관성을 갖는다고 하였고 [22], Han 등은 대사성 인자와 PSA 수치의 관계에 대한 연 구에서 이완기 혈압, 혈중 HDL 콜레스테롤 수치, 공복 혈당 과 함께 BMI가 PSA 수치와 음의 관계를 갖는다고 하였다 [6]. Baillargeon 등은 역학연구에서 전립샘암이 없는 2,770
명을 대상으로 인종, 연령을 보정하였을 때 BMI와 PSA 수 치간의 유의한 음의 관계가 있다고 하였고 [23], Werny 등 은 높은 체중과 BMI, 허리둘레, 삼두근의 피부 두께, 총 신 체 수분량과 PSA 수치의 음의 관계가 있다고 하였다 [24].
비만 환자에서 SHBG의 감소는 혈중 테스토스테론의 감 소를 유발한다 [25]. 또 지방세포는 테스토스테론을 에스트 라디올로 변환시키는 주요 물질이기도 하다 [26]. 비만 환 자의 감소된 테스토스테론이 PSA 수치와 음의 상관성을 시 사하며, 더불어 비만 환자의 증가된 혈장량이 PSA 수치를 희석시킨다는 이론도 있다. Banez 등은 전립샘암으로 근치 적 전립샘적출술을 시행 받은 환자를 대상으로 한 연구에 서 BMI가 클수록 PSA 수치가 낮게 측정됨을 발견하고 이 를 총 혈장량 증가에 의한 PSA 수치의 상대적인 희석으로 추정하였다 [27]. 본 연구에서는 대조군과 달리 대사증후군 에서만 비만이 PSA 수치와 음의 상관관계를 보였다. 불행 히도 아직까지 대사증후군과 대조군에서 각각 비만의 존재 가 어떠한 영향을 주는지에 대해서는 알려진 바가 없다. 비 만은 대사증후군의 가장 중요한 인자이고, 대사증후군의 다른 인자들이 모두 비만과 연관이 있으므로, 비만과 다른 인자들 간의 협력 작용이 있는 것으로 생각되나, 이에 대한 정확한 연구가 필요하다. 또 통계적으로 유의하긴 하였지 만, 상관계수가 −0.078로 매우 미미하게 측정되어, 이에 대 한 대단위적 연구가 필요할 것이다. 또한 통계적으로 유의 하지는 않았으나 대조군에서도 비만이 PSA 수치와 음의 상 관관계를 보이므로 대단위적 연구가 시행된다면 다른 결과 를 얻을 수도 있을 것이다.
본 연구에서 전립샘암 환자를 제외하기 위하여 통상적인 절단치인 4.0 ng/ml를 기준을 사용하여 그 이상인 경우 연구 대상에서 제외하였다. 그러나 일반적으로 전립샘 생검을 시행하는 PSA의 절단치는 4.0 ng/ml이지만, 전립샘암 환자 의 20% 정도가 2.6-4.0 ng/ml 범위에 있으므로 PSA 절단치 를 2.5 ng/ml로 낮춰야 한다는 주장이 제기되고 있다 [28].
이에 본 연구에서는 PSA 수치가 2.5 ng/ml 이상인 군에 대 하여 따로 분석하였다. 단변량 로지스틱 회귀모형에서 대 사증후군의 비만만이 PSA 수치가 2.5 ng/ml 이상일 가능성 을 낮추는 것으로 나타났다 (OR=0.505, p=0.025). Porter와 Stanford는 비만이 남성호르몬 활성을 감소시켜 전립샘암의 위험도가 낮아진다고 하였다 [29]. 그러나 그 반대의 연구 결과도 있어 [30], 비만과 전립샘암의 관계는 향후 더욱 연 구가 진행되어야 하겠다.
결 론
대사증후군이 대조군에 비해 낮은 혈중 PSA 수치를 보였
으며, 대사성 인자가 증가할수록 PSA 수치는 감소하였다.
또, 대사증후군에서 비만이 PSA 수치를 의미 있게 감소시 키는 것으로 나타났다. 따라서 전립샘암의 선별검사로 PSA 를 측정할 경우 대사증후군이 정상군에 비해 낮게 측정될 수 있으므로 주의를 요하며, 특히 대사증후군 중에서도 비 만 환자는 일반적으로 사용되는 PSA 절단치인 4 ng/ml보다 낮은 절단치가 필요할 것으로 생각한다.
REFERENCES
1. Oesterling JE, Kumamoto Y, Tsukamoto T, Girman CJ, Guess HA, Masumori N, et al. Serum prostate-specific antigen in a community-based population of healthy Japanese men: lower values than for similarly aged white men. Br J Urol 1995;75:
347-53.
2. Hammarsten J, Högstedt B. Hyperinsulinemia as a risk factor for developing benign prostatic hyperplasia. Eur Urol 2001;39:
151-8.
3. Sohn JC, Chang HS, Kim CI. The correlation between metabolic syndrome and the prostate volume. Korean J Urol 2007;48:603-7.
4. Kim JH, Shin BS, Kim JS, Hong YS. Voiding dysfunction of men is associated with metabolic syndrome. Korean J Urol 2006;47:257-62.
5. Kim YJ, Cho YJ, Oh JE, Jeon YS, Lee SC, Kim WJ. The association between metabolic syndrome and prostate-specific antigen levels. Int J Urol 2008;15:905-9.
6. Han JH, Choi NY, Bang SH, Kwon OJ, Jin YW, Myung SC, et al. Relationship between serum prostate-specific antigen levels and components of metabolic syndrome in healthy men.
Urology 2008;72:749-54.
7. Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Executive summary of the third report of the national cholesterol education program (NCEP) expert panel on detection, evaluation, and treatment of high blood cholesterol in adults (adult treatment panel III). JAMA 2001;285:2486-97.
8. Reaven GM. Insulin resistance, cardiovascular disease, and the metabolic syndrome: How well do the emperor's clothes fit?
Diabetes Care 2004;27:1011-2.
9. Ford ES. Prevalence of the metabolic syndrome defined by the International Diabetes Federation among adults in the U.S.
Diabetes Care 2005;28:2745-9.
10. Lim S, Park KS, Lee HK, Cho SI. Changes in the characteristics of metabolic syndrome in Korea over the period 1998-2001 as determined by Korean National Health and Nutrition Examination Surveys. Diabetes Care 2005;28:1810-2.
11. Hammarsten J, Högstedt B, Holthuis N, Mellström D. Components of the metabolic syndrome-risk factors for the development of benign prostatic hyperplasia. Prostate Cancer Prostatic Dis 1998;
1:157-62.
12. Parsons JK, Carter HB, Partin AW, Windham BG, Metter EJ, Ferrucci L, et al. Metabolic factors associated with benign prostatic hyperplasia. J Clin Endocrinol Metab 2006;91:2562-8.
13. Kim YD, Yang WJ, Song YS, Park YH. Correlation between prostate volume and metabolic or anthropometric factors in male visitors to a health promotion center. Korean J Urol 2008;49:139-44.
14. Laaksonen DE, Niskanen L, Punnonen K, Nyyssönen K, Tuomainen TP, Salonen R, et al. Sex hormones, inflammation and the metabolic syndrome: a population-based study. Eur J Endocrinol 2003;149:601-8.
15. Laaksonen DE, Niskanen L, Punnonen K, Nyyssönen K, Tuomainen TP, Valkonen VP, et al. Testosterone and sex hormone-binding globulin predict the metabolic syndrome and diabetes in middle-aged men. Diabetes Care 2004;27:1036-41.
16. Khaw KT, Barrett-Connor E. Blood pressure and endogenous testosterone in men: an inverse relationship. J Hypertens 1988;
6:329-32.
17. Zmuda JM, Cauley JA, Kriska A, Glynn NW, Gutai JP, Kuller LH. Longitudinal relation between endogenous testosterone and cardiovascular disease risk factors in middle-aged men: A 13-year follow-up of former multiple risk factor intervention trial participants. Am J Epidemiol 1997;146:609-17.
18. Duell PB, Bierman EL. The relationship between sex hormones and high-density lipoprotein cholesterol levels in healthy adult men. Arch Intern Med 1990;150:2317-20.
19. Werny DM, Saraiya M, Gregg EW. Prostate-specific antigen values in diabetic and nondiabetic US men, 2001-2002. Am J Epidemiol 2006;164:978-83.
20. Barrett-Connor E, Khaw KT, Yen SS. Endogenous sex hormone levels in older adult men with diabetes mellitus. Am J Epidemiol 1990;132:895-901.
21. Han JH, Chang IH, Ahn SH, Kwon OJ, Bang SH, Choi NY, et al. Association between serum prostate-specific antigen level, liver function tests and lipid profile in healthy men. BJU Int 2008;102:1097-101.
22. Sohn JC, Lim MS, Chang HS, Park CH, Kim CI. The association of body mass index and prostate-specific antigen.
Korean J Urol 2007;49:1121-4.
23. Baillargeon J, Pollock BH, Kristal AR, Bradshaw P, Hernandez J, Basler J, et al. The association of body mass index and prostate-specific antigen in a population-based study. Cancer 2005;103:1092-5.
24. Werny DM, Thompson T, Saraiya M, Freedman D, Kottiri BJ, German RR, et al. Obesity is negatively associated with prostate- specific antigen in U.S. men, 2001-2004. Cancer Epidemiol Biomarkers Prev 2007;16:70-6.
25. Amatruda JM, Hochstein M, Hsu TH, Lockwood DH.
Hypothalamic and pituitary dysfunction in obese males. Int J Obes 1982;6:183-9.
26. Eldrup E, Lindholm J, Winkel P. Plasma sex hormones and ischemic heart disease. Clin Biochem 1987;20:105-12.
27. Banez LL, Hamilton RJ, Partin AW, Vollmer RT, Sun L, Rodriguez C, et al. Obesity-related plasma hemodilution and PSA concentration among men with prostate cancer. JAMA 2007;298:2275-80.
28. Catalona WJ, Ramos CG, Carvalhal GF, Yan Y. Lowering PSA cutoffs to enhance detection of curable prostate cancer.
Urology 2000;55:791-5.
29. Porter MP, Stanford JL. Obesity and the risk of prostate cancer. Prostate 2005;62:316-21.
30. Freedland SJ, Terris MK, Platz EA, Presti JC Jr. Body mass index as a predictor of prostate cancer: development versus detection on biopsy. Urology 2005;66:108-13.