대 한 소 아 신 경 학 회 지
Vol. 20, No. 1, March, 2012 □ 증 례 □
- 39 -
Atypical Miller-Fisher Syndrome Presenting as an Isolated Internal Ophthalmoplegia
Following Epstein-Barr Virus Infection
Hye Jin Park, M.D. and Kye Hyang Lee, M.D.
Department of Pediatrics, College of Medicine, Daegu Catholic University, Daegu, Korea
= Abstract =
Acute external ophthalmoplegia, areflexia, and ataxia compose the classic Miller-Fisher syndrome (MFS). Pupillary dysfunction is present in half of patients with MFS. However, isolated internal ophthalmoplegia is rare in children with MFS. We report a case with MFS presenting with isolated internal ophthalmoplegia following an acute Epstein-Barr virus (EBV) infection. An 11-year-old girl with flu-like symptoms was diagnosed with having an acute EBV infection on prior admission. After discharge, she complained of anorexia, poor oral intake and dizziness associated with blurred vision when in the upright position. Physical examination on readmission 10 days later showed anisocoric, mydriatic pupils with an abnormal light reflex.
The patient displayed no external ophthalmoplegia, ataxia or areflexia. Cerebrospinal fluid ana- lysis showed elevated protein with no white blood cells. Serum anti-GQ1b antibody was nega- tive. MFS was diagnosed under clinical findings and CSF albuminocytologic dissociation. Isolated internal ophthalmoplegia can be the sole manifestation of MFS. Therefore, MFS must be con- sidered in the differential diagnosis for children presenting with unexplained acute internal ophthalmoplegia.
Key Words : Miller Fisher syndrome, Ophthalmoplegia, Anisocoria, Mydriasis
1)
Introduction
Miller-Fisher syndrome (MFS) has the clinical triads of variable ophthalmoplegia, tendon are- flexia, and ataxia. Pupillary dysfunction is pre- sent in 35-42% in MFS patients
1, 2). There have been some MFS case reports showing internal ophthalmoplegia as the main clinical features
3-7)
. So far there were several cases reported as having isolated external ophthalmoplegia only
8,9)
or internal ophthalmoplegia together without
접수 : 2012년 2월 14일, 수정 : 2012년 3월 20일 승인 : 2011년 3월 30일
책임저자 : 이계향, 대구가톨릭대학교 의과대학 소아과학교실 Tel : 053)650-4242, Fax : 053)622-4240 E-mail: [email protected]
typical features of MFS in Korea
10). However, there have been no case reports presenting with pupillary dysfunction as the only manifestation of MFS as yet. Here, we report a MFS patient with isolated internal ophthalmoplegia following acute Epstein-Barr virus (EBV) infection.
Case Report
An 11-year-old girl was admitted for gene-
ralized weakness and postural dizziness with
visual dimness. She suffered from acute EBV
infection 10 days prior to readmission. During
her first hospitalization, she presented with a 1-
week history of sore throat, bilateral retroauri-
― Hye Jin Park and Kye Hyang Lee : MFS Presenting with Isolated Internal Ophthalmoplegia ―
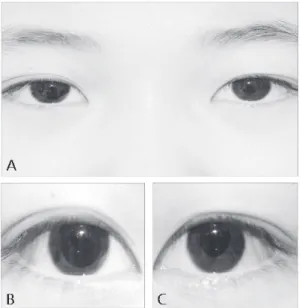
- 40 - Fig. 1. The patient showed anisocoric pupil at admission (A). Right pupil was dilated to 8 mm in diameter and nonreactive to light stimulus (B).
Left pupil was 5 mm in diameter and poorly reactive to light stimulus (C).
Fig. 2. Cholinergic denervation supersensitivity was positive. Right pupil constricted after in- stillation of 0.125% pilocarpine.
cular pain, whole body pain with paresthesia, malaise, and a 5-day history of fever, diarrhea, and epigastric discomfort with anorexia. Her serologic testing was compatible with acute EBV infection: positive for viral capsid antigen (VCA)- IgM, negative for VCA-IgG, EBV early antigen (EA)-IgG, and EBV nuclear antigen (EBNA)- IgG. She was discharged after improvement of her general condition. However, she complained of persistent generalized weakness and poor oral intake. In addition, dizziness with visual dimness developed while in the upright position. Past medical history and family history were unremar- kable. Vital signs were as follows: body tempe- rature of 37℃, blood pressure of 110/70 mmHg, heart rate of 94/min, respiratory rate of 20/min.
Her blood pressure decreased to 90/50 mmHg 1 minute after standing up, which met the diag- nostic definition for orthostatic hypotension. She was chronically ill appearing and in poor general
condition. Her pupils were anisocoric with my- driasis; OD was 8 mm and OS was 5 mm in dia- meter (Fig. 1). Light reflex was absent on the right side, and sluggish on the left side. There was no light-near dissociation, but denervation supersensitivity to a cholinergic agent was po- sitive (Fig. 2). Ophthalmologic examination was normal except for pupillary dysfunction. There were no external ophthalmoplegia or ataxia, and deep tendon reflexes were normal. Brain mag- netic resonance imaging demonstrated no abnor- mal findings. Cerebrospinal fluid (CSF) analysis was as follows: leukocyte 0/μL, protein 102 mg/
dL. CSF polymerase chain reaction for herpes simplex type I, II, EBV and Mycoplasma pneu - moniae were negative. Nerve conduction study showed no abnormalities. Serum anti-GQ1b anti- body was negative. MFS was diagnosed based on clinical findings and CSF albuminocytoloic dissociation. Intravenous immunoglobulin (IVIG) was administered for 5 days. Two month later, her internal ophthalmoplegia persisted but with slightly better reactivity to light stimuli.
Discussion
MFS is defined as an acute monophasic illness
― 대한소아신경학회지 : 제 20 권 제 1 호 2012년 ―
- 41 - featuring the clinical triad of ophthalmoplegia, ataxia, and areflexia. However, on occasion it can present with 2 or even only 1 of these fin- dings. Ophthalmoplegia is the most prevalent and consistent finding in MFS and other related disorders during the acute phase of the illness.
Internal ophthalmoplegia (IO) is quite common in MFS, with pupillary constriction to light and near stimulation ranging from slow to absent.
Light-near dissociation and tonic pupil may be present
1, 2). The tonic pupil develops as a result of damage to the parasympathetic ciliary gang- lion and presents with the following pupillary characteristic: 1) poor light reaction, 2) tonic near response with light-near dissociation, 3) segmental palsy of the sphincter, 4) cholinergic supersensitivity of the denervated muscle
11). Our patient showed bilateral mydriasis with ab- sent or sluggish light reflex, a positive cholinergic supersensitivity, and no light-near dissociation.
As a result, the abnormal pupillary features of our case cannot be termed as a tonic pupil by definition. Though orthostatic hypotension was her main problem responsible for postural dizzi- ness with blurred vision, pupillary dysfunction appeared to be the sole manifestation of the MFS in our patient. Postural hypotension can occur under various conditions, including dysau- tonomia accompanied by peripheral nerve dis- eases such as Guillain-Barré syndrome (GBS).
However, orthostatic hypotension is rarely pre- sent in MFS patients, and no other clinical fin- dings attributable to the autonomic nervous sys- tem (ANS) dysfunction were present in our case.
Also, prolonged poor oral intake and immobility due to generalized weakness can cause ortho- static hypotension more likely than ANS dys- function as in the present case
12). Anti-GQ1b antibody is present in more than 85% of patients
with MFS and it is also found in MFS related diseases such as Bickerstaff’s brainstem ence- phalitis, acute ophthalmoparesis without ataxia (AO), isolated IO, acute ataxia without ophthal- moplegia (ataxic GBS), acute oropharyngeal palsy, acute or chronic sensory neuropathy, and other disorders
1, 2). Nishimoto et al.
13)demonstrated that in the first week after the onset of symp- toms, anti-GQ1b antibodies were almost always present, whereas elevated CSF protein was found in only 25% of cases. They concluded that CSF findings are not as sensitive as the anti-GQ1b antibody assay for the diagnosis of MFS in the early stage of this disorder. CSF protein elevation may be absent at the time of initial symptoms, while becoming more prominent over the next weeks. We presume that our case might have visited after the early stage of the disease, so anti-GQ1b antibody might have been undetec- table whereas positive CSF albuminocytologic dissociation at admission. Based on the current literature, we can categorize patients presenting with IO with positive anti-GQ1b antibody into three groups
3-7). Group I is an AO group having external ophthalmoplegia (EO) together
5, 7), while Group II is an AO without EO or isolated IO group having another symptom of MFS with- out EO
3, 4, 7). Group III is a typical MFS patient
6)