https://doi.org/10.35827/cp.2020.19.1.8
접수일: 2020년 3월 20일, 게재승인일: 2020년 6월 5일 책임저자: 김상준, 서울시 서초구 남부순환로 2606
06737, 서울준재활의학과
Tel: 02-576-0100, Fax: 02-577-0035 E-mail: [email protected]
골수 흡인-혈소판 풍부 혈장과 히알루론산의 관절강내 주사의 효과 비교
성균관대학교 의과대학 삼성서울병원 재활의학교실1, 가톨릭대학교 의과대학 내과학교실 내분비내과2,
이엔셀 바이오, R&D 센터3, 서울준재활의학과4
이병찬1ㆍ김아란1ㆍ김은경2ㆍ김선정3ㆍ김상준4
Effects of Bone Marrow Aspirate Concentrate-Platelet-rich Plasma Versus Hyaluronic Acid on Patients with Knee Osteoarthritis: A Randomized Controlled Trial
Byung Chan Lee, M.D.1, Ah Ran Kim, M.D.1, Eun Kyung Kim, M.S.2, Sun Jeong Kim, M.S.3 and Sang Jun Kim, M.D., Ph.D.4
1Department of Physical and Rehabilitation Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, 2Division of Endocrinology and Metabolism, Department of Internal Medicine, College of Medicine, The Catholic University of Korea, 3R&D Center, ENCell Co. Ltd, 4Seoul Jun Rehabilitation Clinic, Seoul, Korea
Objective: To compare the therapeutic efficacy of the bone marrow aspirate concentrate (BMAC)- platelet-rich plasma (PRP) complex with hyaluronic acid in patients with knee osteoarthritis. Method: Thirty-four patients with knee osteoarthritis participated in this study. Seventeen patients in the study group underwent BMAC and PRP extraction followed by intra-articular injection of BMAC-PRP complex within affected knee. Seventeen patients in the control group underwent intra-articular injection of hyaluronic acid. Knee injury, osteoarthritic outcome score (KOOS), and EuroQol-5D (EQ-5D) questionnaire were evaluated before, one month, three months, and six months after the injection. Results: There were statistically significant temporal differences in total KOOS scores in both BMAC-PRP and HA groups. However, there were no significant group difference in the study period. In the Sports and Recreational Function Scale, there was statistically significant improvement in the BMAC-PRP group compared to the HA group at three months (p=0.041). There were no side effects or complications in both groups. Conclusion: Intra-articular injection of BMAC-PRP showed better functional recovery in the OA at three months and this can be an alternative treatment in terms of functional recovery in the OA in addition to the decrease of pain. (Clinical Pain 2020;19:8-15)
Key Words: Bone marrow aspiration concentrates, Platelet rich plasma, Hyaluronic acid, Osteoarthritis, Knee
INTRODUCTION
Knee osteoarthritis (OA) is the most common joint dis- ease that causes pain and disability. Cartilage loss, sub- chondral bone changes, synovial inflammation, and me- niscus degeneration is common pathologic changes of OA.1 According to worldwide prevalence estimates, 9.6% of males and 18.0% of females over 60 years have sympto- matic OA.2 The prevalence rate is increasing with the aging
society, and recent studies predict that it will constitute one-fourth of the causes of disability by 2020.3 OA symp- toms are mostly controlled with symptomatic management, including oral medication for relieving pain and intra-artic- ular (IA) injection with steroid or hyaluronic acid (HA).
Total joint arthroplasty of the knee can be considered when conservative symptomatic management fails.4
However, most of these treatments focus on relief of symptoms of OA to increase function and mobility, not on delay or prevention of disease progression to avoid disability. In recent years, new biological treatments using for several orthopedic conditions including focal cartilage injuries, OA, and soft tissue injuries have recently grown in popularity to delay or prevent OA progression. In partic- ular, previous studies demonstrated effects of growth fac-
tors in cartilage repair both in vitro and in vivo.5-8 Platelet-rich plasma (PRP), one biological treatment, is concentrated autologous growth factors from a patient's blood. Clinical improvements such as reducing pain and improving quality of life have been reported by intra-artic- ular PRP injections for treatment of focal chondral defects and OA patients.9-12 In addition, previous studies reported that the effect of IA injection of PRP is equivalent or even superior to IA injection of HA.11,12 The mechanism of PRP is based on growth factors, including transforming growth factor β (TGF-β), insulin-like growth factor 1 (IGF-1), bone morphogenetic proteins (BMPs), and platelet-derived growth factor (PDGF). These factors inhibit inflammation and pain while enhancing biosynthesis of cartilage and bone matrix.11
The use of IA injection of bone marrow aspirate concen- trate (BMAC) in various orthopedic conditions has recently become popular. Centrifuged materials from bone marrow aspirates composed of isolated cellular components in dis- tinct layers is called BMAC, which is considered mini- mally manipulated. White blood cells, mesenchymal stem cells (MSCs), hematopoietic stem cells, and platelets are concentrated into one layer and red blood cells into another layer.13 IA injection of MSCs contained in BMAC has been reported to treat joint pain. MSCs has tri-lineage potential to hold promise for tissue regeneration, most notably for chondrogenic potential.14 However, Shapiro et al.14 demon- strated negative and inconclusive results of IA injection of BMAC in patients with knee osteoarthritis.
Previous studies demonstrated that conjunction with scaffold and BMAC can enhance the viability and differ- entiation of stem cells.15 Scaffold materials include HA, collagen, fibrin glue, adipose tissues, and PRP. In partic- ular, PRP may improve the environment for MSC develop- ment and differentiation.16 PRP can also stimulate MSC proliferation, preserve MSC multipotency, and does not in- terfere with any lineage differentiation.17 Recent studies re- ported good regenerative potential in BMAC-PRP complex in diabetic ulcers,16 osteochondral defects,18 and spinal cord injury.19
To the best of our knowledge, the efficacy of IA in- jection of BMAC-PRP in the knees of patients with OA has not been established. This study compares the clinical outcomes of IA injection of BMAC-PRP and HA in knees of patients with OA.
MATERIALS AND METHODS
This study was conducted as a prospective, open-label, randomized controlled, comparative study in Samsung Medical Center. Patients were enrolled from the outpatient clinic and treated with BMAC-PRP or hyaluronic acid in- tra-articular knee injections. The following inclusion cri- teria were used for patient selection: adult older than 19 years, suffered from chronic (at least three months) knee pain or swelling, and radiologically confirmed degenerative changes in the knee joint (simple radiography or MRI).
Exclusion criteria were history of knee arthroplasty or in- tra-articular steroid injection within three months, suspi- cious for systematic infection or inflammation (ESR over 40 mm/hr, CRP over 10 mg/dl), hematologic disorder (coagulopathies), anticoagulant therapy, immunosuppressant medication, and undergoing chemotherapy for cancer.
After recruitment, patients were randomly assigned to BMAC-PRP and hyaluronic acid (HA) groups. Demographic data including age, sex, involved side, and Kellgren and Lawrence (K-L) grade were collected. The K-L grade de- scribes knee OA on plain radiographs as 0 (no radiologic features of OA), 1 (possible joint space narrowing and os- teophyte), 2 (definite osteophyte formation and possible joint space narrowing on weight bearing radiograph), 3 (multiple osteophytes, definite joint space narrowing, scle- rosis, and possible bony deformity), and 4 (large osteo- phytes, marked joint space narrowing, severe sclerosis and definite bony deformity). Knee injury and osteoarthritic outcome score (KOOS) and EuroQol-5D (EQ-5D) ques- tionnaires were administered by one experienced physician who was blinded to group assignment of each patient to evaluate pain and disability. These outcome instruments were recorded before the procedure and at 1 month after, 3 months after, and 6 months after the procedure in both groups. Knee plain radiography was obtained before and 6 months after the procedure.
BMAC extraction was taken from Patients in the BMAC-PRP group. Patients laid on a table in the prone position. Skin sterilization was performed by povidone io- dine and skin and periosteum anesthetic procedure by 1%
lidocaine was followed. The iliac bone was penetrated by a bone marrow aspiration needle and aspiration of bone marrow was performed. To isolate concentrated BMACs, bone marrow aspirates were centrifuged with a BIOMET
Fig. 1. BIOMET MarrowStimTM Mini kit was used to acquire bone marrow aspirates. Acquired bone marrow aspirates were centrifuged to isolate the concentrated BMACs. BMAC: bone marrow aspirate concentration.
MarrowStimTM Mini kit (Biomet Biologics, Inc., Warsaw, IN, USA) (Fig. 1).
To extract PRP, 60 ml autologous whole blood was re- trieved from a patient’s median cubital vein. The whole blood was centrifuged with a BIOMET GPSTM III kit (Biomet Biologics, Inc.). 6 ml of citrate anticoagulant and 54 ml of autologous whole blood were mixed and then cen- trifuged at 3,200 RPM for 15 minutes. The platelet-poor plasma (PPP) was then separated. Extraction of remaining PRP contents followed.
After procedure, 2 ml of BMACs and 1 ml of PRP were mixed in a 5 ml syringe. IA injection BMAC-PRP to osteo- arthritis knee joint was performed by one experienced physiatrist. IA injection of HA to osteoarthritic knee joint was performed in HA group.
Oral medication including non-steroidal anti-inflammatory drugs and other pain killers was prohibited during the study period. Only acetaminophen was allowed.
Initially, to address clinical improvement, total score, score of subscales of KOOS and EQ-5D from baseline to the final follow-up and between-group differences were evaluated with dependent and independent t tests, respec- tively. Repeated measures analysis of variance models for total KOOS and all five KOOS subscale, EQ-5D in each group were performed to evaluate within-group changes over time for each follow-up interval. Post-hoc analysis was performed by the Scheffé test to evaluate significant differences between each follow-up time points. SPSS 20.0 software (IBM Corp, Chicago, IL, USA) was used for anal- ysis, and p less than 0.05 were considered statistically significant.
Sample size was calculated based on the literature com- paring KOOS between surgical and non-surgical treatment
groups.20 A difference of at least 16.5 in KOOS was con- sidered statistically meaningful. Standard deviation was es- tablished as 12.5 based on standard deviation observed be- tween the two groups. Considering a 0.05 two-sided sig- nificance level, power of 90%, and an allocation ratio of 1:1, at least 15 patients were required in each group.
Because the approximate dropout rate was estimated as 10%, 17 patients in each group was the recruitment goal.
The study protocol was approved by the Institutional Review Board of Samsung Medical Center, and patients were registered in the institutional board registry (registry number: SMC 2016-12-061). Written informed consent was acquired from all patients.
RESULTS
A total of 34 knees of 34 patients participated in the study from November 2017 to October 2018. Patients were randomly assigned to two groups: 17 patients (7 men and 10 women) were assigned to the BMAC-PRP group, and 17 patients (7 men and 10 women) were assigned to the HA group. Average age was 66.88 ± 7.39 years in the BMAC PRP group and 69.41 ± 6.54 years in the HA group (p=0.844). Of 34 knees in the BMAC PRP group, 8 were radiographically graded as K-L grade 2 (2 in the BMAC- PRP group, 6 in the HA group), 17 were graded as K-L grade 3 (8 in the BMAC-PRP group, 9 in the HA group), and 9 were graded as K-L grade 4 (7 in the BMAC-PRP group, 2 in the HA group). Initial KOOS score was 241.71
± 93.87 in the BMAC-PRP group and 243.68 ± 83.3 in the HA group (p=0.949). There were no significant differences in initial KOOS score between the two groups (Table 1).
In both groups, mean total KOOS score improved after
Table 3. Within-Group Difference in Patient-Reported Outcome Scores Across All Time Points Among the BMAC-PRP Group
Measurement: subscale Initial assessment One month Three months Six months KOOS: Total 241.71 ± 93.87†,‡,§ 283.75 ± 73.99* 321.03 ± 101.48* 320.99 ± 83.35*
KOOS: Pain 56.37 ± 15.92†,‡,§ 65.66 ± 13.96* 71.21 ± 17.80* 71.97 ± 13.40*
KOOS: Symptom 59.45 ± 17.67†,‡,§ 66.24 ± 14.41* 72.73 ± 16.54* 75.00 ± 15.32*
KOOS: ADL 58.82 ± 24.90†,‡,§ 67.51 ± 15.17* 73.80 ± 18.27* 76.07 ± 15.97*
KOOS: Sports 28.82 ± 23.62§ 35.45 ± 19.81 43.64 ± 32.57 42.27 ± 28.14*
KOOS: QOL 38.24 ± 21.52†,‡,§ 48.86 ± 20.69* 59.66 ± 23.78* 55.68 ± 21.19*
EQ-5D 8.65 ± 1.69 7.70 ± 0.95 7.80 ± 1.69 7.4 ± 1.84
BMAC: bone marrow aspirate concentration, PRP: platelet rich plasma, HA: hyaluronic acid, KOOS: Knee injury and osteoarthritic outcome score, ADL: Activities of Daily Living, QOL: Quality of Life, EQ-5D: EuroQol-5D.
*Significantly different from the initial assessment. †Significantly different from one month follow-up. ‡Significantly different from three month follow up. §Significantly different from six month follow up.
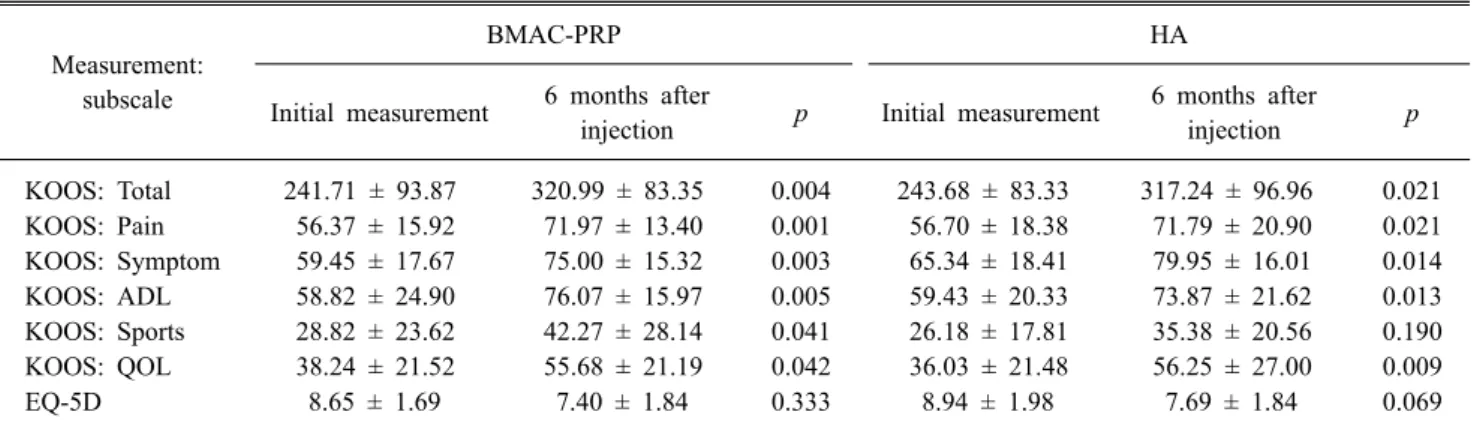
Table 2. Within-Group Difference in Patient-Reported Outcome Scores from BMAC-PRP Group and HA Group
Measurement:
subscale
BMAC-PRP HA
Initial measurement 6 months after
injection p Initial measurement 6 months after
injection p
KOOS: Total 241.71 ± 93.87 320.99 ± 83.35 0.004 243.68 ± 83.33 317.24 ± 96.96 0.021 KOOS: Pain 56.37 ± 15.92 71.97 ± 13.40 0.001 56.70 ± 18.38 71.79 ± 20.90 0.021 KOOS: Symptom 59.45 ± 17.67 75.00 ± 15.32 0.003 65.34 ± 18.41 79.95 ± 16.01 0.014 KOOS: ADL 58.82 ± 24.90 76.07 ± 15.97 0.005 59.43 ± 20.33 73.87 ± 21.62 0.013 KOOS: Sports 28.82 ± 23.62 42.27 ± 28.14 0.041 26.18 ± 17.81 35.38 ± 20.56 0.190 KOOS: QOL 38.24 ± 21.52 55.68 ± 21.19 0.042 36.03 ± 21.48 56.25 ± 27.00 0.009
EQ-5D 8.65 ± 1.69 7.40 ± 1.84 0.333 8.94 ± 1.98 7.69 ± 1.84 0.069
BMAC: bone marrow aspirate concentration, PRP: platelet rich plasma, HA: hyaluronic acid, KOOS: Knee injury and osteoarthritic outcome score, ADL: Activities of Daily Living, QOL: Quality of Life, EQ-5D: EuroQol-5D.
Table 1. Age, Initial KOOS, Kellgren-Lawrence Grade between BMAC-PRP and HA Groups
BMAC-PRP HA p
Age 66.88 ± 7.39 69.41 ± 6.54 0.84
Initial KOOS 235.86 ± 68.91 234.97 ± 82.67 0.95
K-L grade 0.10
K-L grade 2 2 6
K-L grade 3 8 9
K-L grade 4 7 2
Values are mean ± standard deviation.
BMAC: bone marrow aspirate concentration, PRP: platelet rich plasma, HA: Hyaluronic Acid, KOOS: Knee injury and osteo- arthritic outcome score, K-L grade: Kellgren and Lawrence grade.
treatment (Table 2). Follow up KOOS score at one month was 283.75 ± 73.99 in the BMAC-PRP group and 281.74
± 67.59 in the HA group. Follow up KOOS score at 3 months and 6 months was 321.03 ± 101.48 and 320.99 ± 83.35 in the BMAC-PRP group, and 318.92 ± 84.98 and 317.24 ± 96.96 in the HA group, respectively (Table 3, 4).
However, there is no group difference noted at final 6 month follow up (Table 5).
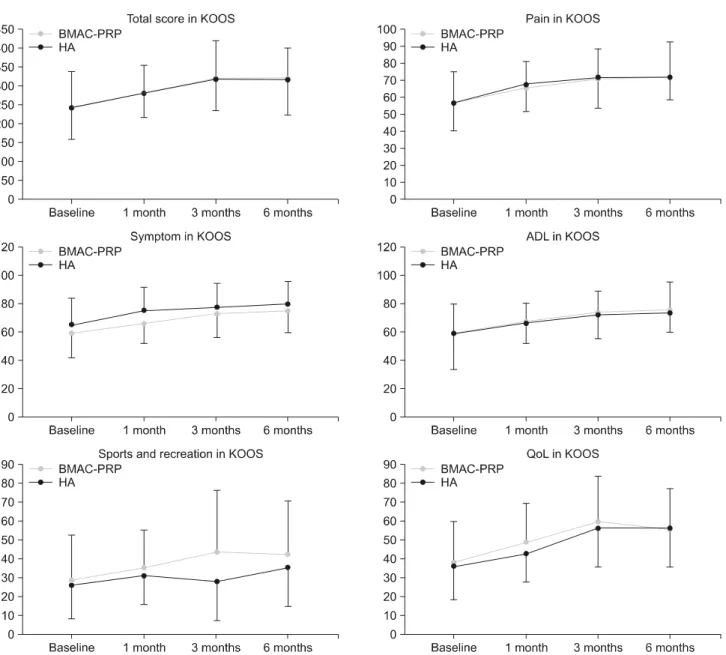
In five KOOS subscales (Pain, Symptoms, Activities of Daily Living, Sports and Recreational Function, and Knee-Related Quality of Life), there were no statistically significant differences between groups (Fig. 2). However, only in Sports and Recreational Function Scale, Initial Score was 28.82 ± 23.62, and follow up score at 6 months was 42.27 ± 28.14 which was statistically significant in BMAC-PRP group (p=0.041). Initial Score was 26.18 ± 17.81 and follow up score at 6 months was 35.38 ± 20.56 in HA group (p=0.190) (Table 2).
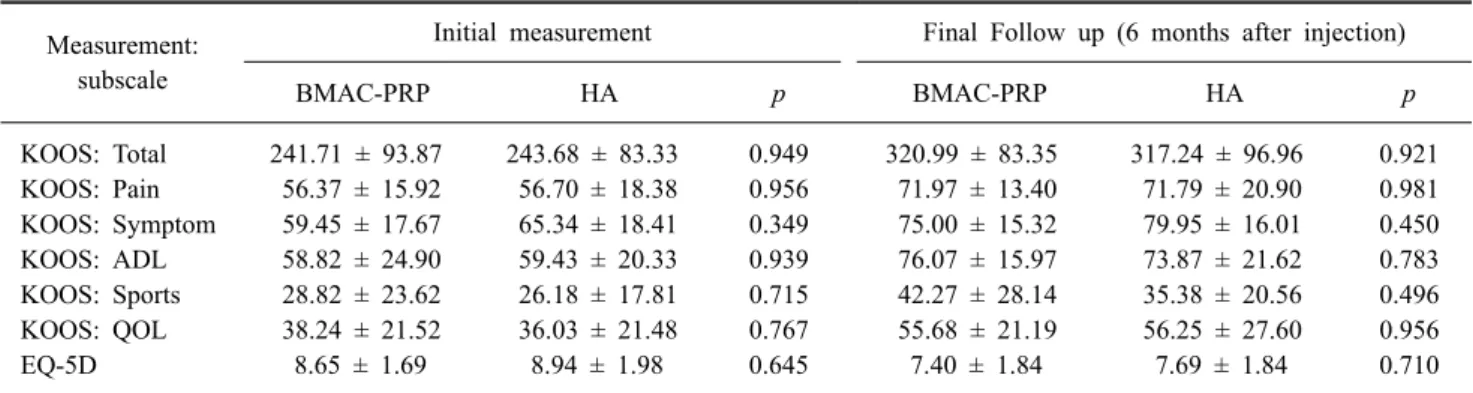
Table 5. Between-Group Difference in Patient-Reported Outcome Scores from BMAC-PRP Group and HA Group Measurement:
subscale
Initial measurement Final Follow up (6 months after injection)
BMAC-PRP HA p BMAC-PRP HA p
KOOS: Total 241.71 ± 93.87 243.68 ± 83.33 0.949 320.99 ± 83.35 317.24 ± 96.96 0.921 KOOS: Pain 56.37 ± 15.92 56.70 ± 18.38 0.956 71.97 ± 13.40 71.79 ± 20.90 0.981 KOOS: Symptom 59.45 ± 17.67 65.34 ± 18.41 0.349 75.00 ± 15.32 79.95 ± 16.01 0.450 KOOS: ADL 58.82 ± 24.90 59.43 ± 20.33 0.939 76.07 ± 15.97 73.87 ± 21.62 0.783 KOOS: Sports 28.82 ± 23.62 26.18 ± 17.81 0.715 42.27 ± 28.14 35.38 ± 20.56 0.496 KOOS: QOL 38.24 ± 21.52 36.03 ± 21.48 0.767 55.68 ± 21.19 56.25 ± 27.60 0.956
EQ-5D 8.65 ± 1.69 8.94 ± 1.98 0.645 7.40 ± 1.84 7.69 ± 1.84 0.710
BMAC: bone marrow aspirate concentration, PRP: platelet rich plasma, HA: hyaluronic acid, KOOS: Knee injury and osteoarthritic outcome score, ADL: Activities of Daily Living, QOL: Quality of Life, EQ-5D: EuroQol-5D.
Table 4. Within-Group Difference in Patient-Reported Outcome Scores Across All Time Points Among the HA Group
Measurement: subscale Initial assessment One month Three months Six months KOOS: Total 243.68 ± 83.33‡,§ 281.74 ± 67.59§ 318.92 ± 84.98* 317.24 ± 96.96*,†
KOOS: Pain 56.70 ± 18.38‡,§ 67.74 ± 13.11 71.79 ± 16.47* 71.79 ± 20.90*
KOOS: Symptom 65.34 ± 18.41‡,§ 75.55 ± 16.23 77.47 ± 16.78* 79.95 ± 16.01*
KOOS: ADL 59.43 ± 20.33‡,§ 66.40 ± 14.18 72.17 ± 16.89* 73.87 ± 21.62*
KOOS: Sports 26.18 ± 17.81 31.15 ± 15.16 28.08 ± 20.47 35.38 ± 20.56
KOOS: QOL 36.03 ± 21.48‡,§ 42.79 ± 20.39 56.25 ± 21.50* 56.25 ± 27.60*
EQ-5D 8.94 ± 1.98 8.92 ± 1.71 8.54 ± 1.61 7.69 ± 1.84
BMAC: bone marrow aspirate concentration, PRP: platelet rich plasma, HA: hyaluronic acid, KOOS: Knee injury and osteoarthritic outcome score, ADL: Activities of Daily Living, QOL: Quality of Life, EQ-5D: EuroQol-5D.
*Significantly different from the initial assessment. †Significantly different from one month follow-up. ‡Significantly different from three month follow up. §Significantly different from six month follow up.
Initial EQ-5D was 8.65 ± 1.69 in the BMAC-PRP group and 8.94 ± 1.98 in the HA group. Final EQ-5D was 7.40
± 1.84 in the BMAC-PRP group and 7.69 ± 1.84 in the HA group. There were no differences between groups (Table 5) and all time point (Table 3, 4). There were no side effects in either group.
DISCUSSION
This study showed that intra-articular BMAC-PRP in- jection improved clinical symptoms in patients with knee OA equivalently to intra-articular HA injection. At 3 months, BMAC-PRP injection group showed statistically significant improvement of scores in sports and recreational function subscales of KOOS which is not demonstrated in HA injection group.
Our study demonstrated that intra-articular BMAC-PRP injection improved KOOS and EQ-5D without any side effects. This might be due to the known regenerative and anti-inflammatory activities of BMAC and PRP, which were demonstrated in previous studies.10,18,21,22
However, radiographic, histologic, and cytokine studies were not con- ducted in this research.
It is difficult to know that the BMAC-PRP complex is more effective than the BMAC or PRP alone in this study because we did not assign any groups to receive BMAC or PRP alone. We had to focus on the optimal protocols to improve the functional recovery in the OA rather than to investigate the therapeutic mechanism of BMAC or PRP because extraction of BMAC was an invasive procedure.
We hypothesized that PRP plays a role as a cell scaffold for BMAC components, and BMAC might play a role as
Fig. 2. Changes in mean total KOOS scales and five subscales (Pain, Symptoms, Activities of Daily Living, Sports and Recreational Function, and Knee-Related Quality of Life) in BMAC-PRP group and HA group are presented. All subscales were significantly increased after the procedure except Sports and Recreational Function scale in HA group (p=0.190). BMAC: bone marrow aspirate concentration, PRP: platelet rich plasma, HA: Hyaluronic Acid, KOOS: Knee injury and osteoarthritic outcome score.
a regenerative and anti-inflammatory activator by secreting growth factors and cytokines,23 so we determined BMAC- PRP injection as a study group rather than BMAC injection alone. Previous study suggests that BMAC injection with- out PRP would be insufficient because BMAC contains less than 0.001% mononucleated cells, and the regeneration potential of those cells may not be optimal.23 However, several previous studies suggest that un-cultured BMAC causes lesion coverage and tissue repair.22,24
Although we did not find superiority of BMAC-PRP over HA in the total scores of KOOS and EQ-5D, clinical superiority of BMAC-PRP over HA was observed in sports and recreational function subscales of KOOS. These results indicate that BMAC-PRP groups have better performance than HA groups and suggest that BMAC-PRP reduces pain and increases functional recovery more than HA. This would be important in terms of functional recovery in OA because most treatments in the OA have shown decrease
of pain and few treatments showed improvement of func- tional recovery. Our results were similar with a Kim’s study,25 which showed improvement of Lysholm score after BMAC injection with adipose tissue. While the improve- ment of KOOS was similar between one and six months after BMAC-PRP injection in our study, continuous im- provement of Lysholm score was observed in the Kim’s study. We thought that this difference might be due to the difference of characteristics of BMAC scaffold. PRP is flu- id material while adipose tissue is solid one, which could stay longer in the joint cavity than PRP. However, we think that adipose tissue does not play an important role as an enhancing factor for BMAC because Centeno’s study showed there was no significant difference between with and without adipose graft in the efficacy of BMAC.26 During or after injection, there were no side effects or complications.
There are several limitations of this study. One is that the study was designed as an open label study. To perform a double-blind study, BMAC-PRP must be discarded after bone marrow aspiration and blood sampling in the control group. This is ethically challenging because bone marrow aspiration is an invasive procedure. The relatively small sample size for comparative study is also a limitation.
Longer follow up duration is also needed to prove the sus- tained efficacy of BMAC-PRP. The last limitation is that the cell count and number of anti-inflammatory mediators in aspirates was not analyzed. Further studies with a larger sample size and double-blind design are necessary to clar- ify the therapeutic effects of BMAC-PRP on knee OA.
CONCLUSION
This study demonstrated that BMAC-PRP improved pain and function in patients with knee OA. BMAC-PRP has equal effects as HA, which had proven efficacy in previous studies. There was greater improvement on sports activity and recreational sub-scores in BMAC-PRP group than HA group. This indicates that BMAC-PRP is a more appro- priate alternative option in patients with relatively active lifestyles. A double-blind, randomized controlled study with a larger sample size is necessary to clarify the ther- apeutic effects of BMAC-PRP on knee OA.
DECLARATION OF CONFLICTING INTERESTS
There was no commercial conflict of interest in this study.
FUNDING
This work was supported by the National Research Fund (2018R1D1A1B07047084).
REFERENCES
1. Loeser RF, Goldring SR, Scanzello CR, Goldring MB.
Osteoarthritis: a disease of the joint as an organ. Arthritis Rheum 2012; 64: 1697-1707
2. Woolf AD, Pfleger B. Burden of major musculoskeletal conditions. Bull World Health Organ 2003; 81: 646-656 3. Brand C, Hunter D, Hinman R, March L, Osborne R,
Bennell K. Improving care for people with osteoarthritis of the hip and knee: how has national policy for osteoarthritis been translated into service models in Australia? Int J Rheum Dis 2011; 14: 181-190
4. Bruyere O, Cooper C, Pelletier JP, Branco J, Luisa Brandi M, Guillemin F, et al. An algorithm recommendation for the management of knee osteoarthritis in Europe and inter- nationally: a report from a task force of the European Society for Clinical and Economic Aspects of Osteoporosis and Osteoarthritis (ESCEO). Semin Arthritis Rheum 2014;
44: 253-263
5. Hickey DG, Frenkel SR, Di Cesare PE. Clinical applica- tions of growth factors for articular cartilage repair. Am J Orthop (Belle Mead NJ) 2003; 32: 70-76
6. Schmidt MB, Chen EH, Lynch SE. A review of the effects of insulin-like growth factor and platelet derived growth factor on in vivo cartilage healing and repair. Osteoarthritis Cartilage 2006; 14: 403-412
7. Frazer A, Bunning RA, Thavarajah M, Seid JM, Russell RG. Studies on type II collagen and aggrecan production in human articular chondrocytes in vitro and effects of transforming growth factor-beta and interleukin-1beta.
Osteoarthritis Cartilage 1994; 2: 235-245
8. Grimaud E, Heymann D, Redini F. Recent advances in TGF-beta effects on chondrocyte metabolism. Potential therapeutic roles of TGF-beta in cartilage disorders.
Cytokine Growth Factor Rev 2002; 13: 241-257
9. Campbell KA, Saltzman BM, Mascarenhas R, Khair MM, Verma NN, Bach BR, Jr., et al. Does Intra-articular Platelet-Rich Plasma Injection Provide Clinically Superior Outcomes Compared With Other Therapies in the Treatment
of Knee Osteoarthritis? A Systematic Review of Overlapping Meta-analyses. Arthroscopy 2015; 31: 2213-2221
10. Kon E, Buda R, Filardo G, Di Martino A, Timoncini A, Cenacchi A, et al. Platelet-rich plasma: intra-articular knee injections produced favorable results on degenerative carti- lage lesions. Knee Surg Sports Traumatol Arthrosc 2010;
18: 472-479
11. Cole BJ, Karas V, Hussey K, Pilz K, Fortier LA. Hyaluronic Acid Versus Platelet-Rich Plasma: A Prospective, Double- Blind Randomized Controlled Trial Comparing Clinical Outcomes and Effects on Intra-articular Biology for the Treatment of Knee Osteoarthritis. Am J Sports Med 2017;
45: 339-346
12. Say F, Gurler D, Yener K, Bulbul M, Malkoc M. Platelet- rich plasma injection is more effective than hyaluronic acid in the treatment of knee osteoarthritis. Acta Chir Orthop Traumatol Cech 2013; 80: 278-283
13. Moatshe G, Morris ER, Cinque ME, Pascual-Garrido C, Chahla J, Engebretsen L, et al. Biological treatment of the knee with platelet-rich plasma or bone marrow aspirate concentrates. Acta Orthop 2017; 88: 670-674
14. Shapiro SA, Kazmerchak SE, Heckman MG, Zubair AC, O'Connor MI. A Prospective, Single-Blind, Placebo-Controlled Trial of Bone Marrow Aspirate Concentrate for Knee Osteoarthritis. Am J Sports Med 2017; 45: 82-90 15. Willerth SM, Sakiyama-Elbert SE. Combining stem cells
and biomaterial scaffolds for constructing tissues and cell delivery. In: StemBook, Cambridge (MA): Harvard Stem Cell Institute, 2008
16. Lian Z, Yin X, Li H, Jia L, He X, Yan Y, et al. Synergistic effect of bone marrow-derived mesenchymal stem cells and platelet-rich plasma in streptozotocin-induced diabetic rats.
Ann Dermatol 2014; 26: 1-10
17. Rubio-Azpeitia E, Andia I. Partnership between plate- let-rich plasma and mesenchymal stem cells: in vitro experience. Muscles Ligaments Tendons J 2014; 4: 52-62 18. Betsch M, Schneppendahl J, Thuns S, Herten M, Sager M,
Jungbluth P, et al. Bone marrow aspiration concentrate and
platelet rich plasma for osteochondral repair in a porcine osteochondral defect model. PLoS One 2013; 8: e71602 19. Zhao T, Yan W, Xu K, Qi Y, Dai X, Shi Z. Combined treat-
ment with platelet-rich plasma and brain-derived neuro- trophic factor-overexpressing bone marrow stromal cells supports axonal remyelination in a rat spinal cord hemi- section model. Cytotherapy 2013; 15: 792-804
20. Skou ST, Roos EM, Laursen MB, Rathleff MS, Arendt- Nielsen L, Simonsen O, et al. A Randomized, Controlled Trial of Total Knee Replacement. N Engl J Med 2015; 373:
1597-1606
21. Kim SJ, Song DH, Park JW, Park S, Kim SJ. Effect of Bone Marrow Aspirate Concentrate-Platelet-Rich Plasma on Tendon-Derived Stem Cells and Rotator Cuff Tendon Tear. Cell Transplant 2017; 26: 867-878
22. Krych AJ, Nawabi DH, Farshad-Amacker NA, Jones KJ, Maak TG, Potter HG, et al. Bone Marrow Concentrate Improves Early Cartilage Phase Maturation of a Scaffold Plug in the Knee: A Comparative Magnetic Resonance Imaging Analysis to Platelet-Rich Plasma and Control. Am J Sports Med 2016; 44: 91-98
23. Chahla J, Alland JA, Verma NN. Bone Marrow Aspirate Concentrate for Orthopaedic Use. Orthop Nurs 2018; 37:
379-381
24. Gobbi A, Whyte GP. One-Stage Cartilage Repair Using a Hyaluronic Acid-Based Scaffold With Activated Bone Marrow-Derived Mesenchymal Stem Cells Compared With Microfracture: Five-Year Follow-up. Am J Sports Med 2016; 44: 2846-2854
25. Kim JD, Lee GW, Jung GH, Kim CK, Kim T, Park JH, et al. Clinical outcome of autologous bone marrow aspi- rates concentrate (BMAC) injection in degenerative arthri- tis of the knee. Eur J Orthop Surg Traumatol 2014; 24:
1505-1511
26. Centeno C, Pitts J, Al-Sayegh H, Freeman M. Efficacy of autologous bone marrow concentrate for knee osteoarthritis with and without adipose graft. Biomed Res Int 2014; Epub ahead of print.