679
목 적: Tubular retractor와 현미경을 이용한 최소 침습적 요추간판 제거술의 소개와 함께 이 수술법의 단기적 임상 결과와 장점을 알아보고자 하였다.
대상 및 방법: 2003년 4월부터 2004년 4월까지, 45명의 요추간판 탈출증 환자를 대상으로 tubular retractor (METRx-MD System, Medtronic Sofamor Danek, Memphis, TN)와 현미경을 사용하여 요추간판 제거술을 실시하였다. 모든 환자에 서 1인치 크기의 정중방(para-median) 피부 절개를 통해 tubular retractor를 삽입하고 이를 통하여 후방 감압술을 시행하 였다. 수술 후 임상 결과, 수술 시간, 실혈량, 수혈 유무, 보행 시기, 입원 기간 및 합병증에 관한 결과를 수집, 분석하였고, 수술 후 임상 결과는 MacNab 분류를 사용하여 평가하였다.
결 과: Tubular retractor를 이용하여 최소 침습적 요추 후방 감압술을 시행 받은 45명의 환자 중, MacNab 분류에 따른 임 상 결과는 최우수 33명(73%), 우수 10명(22%)이었다. 평균 수술 시간이 63분(35-95분) 소요되었고, 평균 실혈량은 62 mL (50-110 mL)로 측정되었고, 수혈이 필요한 경우는 없었다. 또한 2명을 제외한 43명의 환자가 수술 당일 자발적인 보행을 할 수 있었으며, 평균 입원 기간은 2.3일이었다. 경막 손상, 수술 후 감염, 수술 후 재발 및 다른 합병증은 관찰되지 않았다.
결 론: Tubular retractor와 현미경을 이용한 요추간판 제거술은 요추간판 탈출증 치료의 유용한 술기이며, 기존 고식적인 수술의 장점을 그대로 유지시키면서도, 최소 침습적 접근법을 통하여 만족할 만한 임상 결과를 가져올 것으로 사료된다.
색인 단어: 최소 침습적, 요추간판 제거술, Tubular retractor, 현미경
Department of Orthopedic Surgery, National Health Insurance Corporation Ilsan Hospital, Goyang; Department of Orthopedic Surgery, Yonsei University College of Medicine*, Seoul, Korea
Yung Park, M.D., Joong Won Ha, M.D., Hyun Cheol Oh, M.D., Ju Hyung Yoo, M.D., Yun Tae Lee, M.D., Doo Hyung Lee, M.D.*, and Chul Jun Choi, M.D.*
Minimally Invasive Lumbar Microdiscectomy using Tubular Retractor
- A Preliminary Report -
679
Tubular Retractor와 현미경을 이용한 최소 침습적 요추간판 제거술
- 예비 보고 -
박 융ㆍ하중원ㆍ오현철ㆍ유주형ㆍ이윤태ㆍ이두형*ㆍ최철준*
국민건강보험공단 일산병원, 연세대학교 의과대학 정형외과학교실*
679 679 통신저자 : 하 중 원
경기도 고양시 일산구 백석동 1232 국민건강보험공단 일산병원 정형외과학교실 TEL: 031-900-0270∙FAX: 031-900-0049
E-mail: [email protected]
*본 논문의 요지는 2004년도 대한정형외과학회 추계학술대회에서 발표되었음.
*본 논문은 2004년도 국민건강보험공단 일산병원의 임상연구비의 지원을 받 아 이루어졌음.
Address reprint requests to Joong Won Ha, M.D.
Department of Orthopaedic Surgery, National Health Insurance Corporation Ilsan Hospital, 1232 Baekseok-dong, Ilsan-gu, Goyang 411-719, Korea
Tel: +82.31-900-0270, Fax: +82.31-900-0049 E-mail: [email protected]
Purpose:To evaluate the early clinical results of lumbar microdiscectomy using minimally invasive tubu- lar retractor (METRx-MD system, Medtronic Sofamor Danek, Memphis, TN), and to validate the merits of minimally invasive spinal surgery.
Materials and Methods:From April, 2003 to April 2004 we retrospectively studied a consecutive series of 45 patients who underwent lumbar microdiscectomy using minimally invasive tubular retractor. In all cases, minimally invasive approach using the tubular retractor were performed with a 2 cm sized para- median incision. The following data were collected: clinical outcomes, operative time, intraoperative blood loss, need for blood replacement, time needed before ambulation, length of hospital stay, and complica- tions. The clinical outcomes were assessed by the modified MacNab criteria.
Results:Minimally invasive tubular microdiscectomy was performed in 45 patients over a 12-month peri-
Minimally invasive approaches to the lumbar spine have been attempted with success over the past 25 years. The minimally invasive spinal surgery was developed as a poten- tial solution to iatrogenic soft tissue injury while still accom- plishing the traditional goals of the open procedure. Microen- doscopic discectomy was developed by Foley and Smith4-6), and represents the first microendoscopic technique enabling the surgeon to efficiently explore the canal and foramen, and perform bony decompression3). With the evolution of expanded applications of the tubular retractor, a more des- criptive name has been given to the system. Microdiscecto- my endoscopic tubular prescriptions (METRx, Medtronic Sofamor Danek, Memphis, TN) describes a tubular retractor system that allows a muscle-splitting approach to the spine.
This system has been termed METRx-MD to encompass its microdiscectomy option.
Satisfactory results have been reported from clinical stud- ies showing that this system offers many advantages over other minimally invasive lumbar discectomy techniques
2,3,5-8,12,13)by reducing soft tissue trauma, allowing direct visu-
alization of the nerve root and disc pathology, and allowing bony decompression. However, the experiences about lum- bar discectomy with tubular retractor are limited, especially for the technique using operative microscope instead of en- doscopy.
We conducted a study retrospectively to evaluate the early clinical results of minimally invasive lumbar microdiscec- tomy using tubular retractor and to validate the merits of this procedure.
MATERIALS AND METHODS
A consecutive series of 45 patients underwent minimally invasive lumbar microdiscectomy using tubular retractor from April 2003 to April 2004. All of them were failed to relieve their symptoms despite of appropriate conservative treatments. All patients had unilateral lumbar disc hernia- tions as demonstrated by CT and/or MRI. All of disc hernia- tions were shown to compress the symptomatic nerve root.
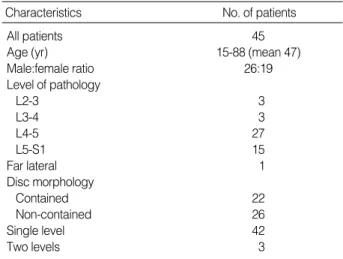
Using the METRx-MD spinal access systems (Medtronic Sofamor Danek, Memphis, TN), minimally invasive lum- bar microdiscectomy was performed through a 2 cm sized skin incision after induction of general endotracheal anes- thesia. The patients demographic characteristics of this study were listed on the Table 1. We excluded the patients who performed previous spinal surgery, concomitant spinal steno- sis, and spinal instability.
The data collected for analysis were age, gender, preoper-
Characteristics No. of patients
All patients 45
Age (yr) 15-88 (mean 47)
Male:female ratio 26:19
Level of pathology
L2-3 3
L3-4 3
L4-5 27
L5-S1 15
Far lateral 1
Disc morphology
Contained 22
Non-contained 26
Single level 42
Two levels 3
Table 1.Clinical characteristics and procedure data
ative diagnosis, operative time, intraoperative estimated blood loss, need for blood replacement, time needed before ambulation, length of hospital stay, and complications. We reviewed all of the charts including progress note, discharge summary, and anesthesia records to determine the above data.
Operation time was checked from the beginning of skin incision to the end of skin closure. Intraoperative blood loss and need for blood replacement were obtained from the records of anesthesia. For the evaluation of clinical outcomes after surgery, the modified MacNab criteria (Table 2) were used at the last follow-up. An average follow-up period of all patients was approximately 8 months (range, 3 to 18 months) over a 12 month period.
Operative technique
Patients were prepared and positioned as in standard lum- bar decompression. We used minimally invasive tubular retractor system (METRx-MD System, Medtronic Sofamor Danek, Memphis, TN) (Fig. 1). Under fluoroscopic guid- ance with guide wire held laterally to the patient, the approxi- mate level of the incision was marked approximately 1 inch off the midline. A small stab incision was then made in the midline of the marking line through which the guide wire was passed to the medial bony facet margin. The skin incision was extended above and below the guide wire total length of approximately 2 cm. The sequential dilators were then passed over the guide wire to dilate the lumbar musculature gently and to expand the lumbodorsal fascia (Fig. 2). The final working channel of the tubular retractor was then passed over the dilators and secured to the flexible-arm retractor mounted to the table side rail (Fig. 3). After proper tissue
Results Criteria
Excellent No pain: no restriction of mobility: return to normal work & level of a activity
Good Occasional nonradicular pain; relief of presenting symptoms; return to modified work
Fair Some improved functional capacity; still handica- pped & unemployed
Poor Continued objective symptoms of root involvement;
additional operative intervention needed at the index level, irrespective of repeat or length of postoperative follow up
Table 2.Modified MacNab criteria for characterizing outcome after spinal surgery
Fig. 1.Minimally invasive tubular retractor system.
Fig. 2.Sequential dilators were passed over the guide wire to dilate lumbar musculature gently and to expand the lumbodorsal fascia.
moved with a pituitary forcep in a standard fashion. Intradis- cal and extradiscal work was preformed as one would nor- mally do during a standard open microdiscectomy. At this
sterile adhesive dressing (Fig. 5).
RESULTS
Minimally invasive lumbar microdiscectomy was per-
Fig. 4.Decompression was completed through tubular retractor.
Fig. 5.One inch sized postoperative wound.
Fig. 3.The final working channel of tubular retractor was passed over the dilators and secured to the flexible-arm mounted to table side rail.
L5
formed on the 45 patients over a 12-month period with an average follow-up of approximately 8 months (range, 3 to 18 months). Of the 45 patients, 26 were males and 19 were females with a average age of 47 years (range, 15 to 88 years).
None of operations was converted to a standard open pro- cedure for better visualization. Twenty seven of the proce- dures were performed at the L4-5 level, 15 at the L5-S1, 3 at the L2-3, and 3 at the L3-4. And 42 procedures were per- formed at the single level and 3 at the two levels. Twenty six cases had non-contained sequestered discs and 22 cases were contained discs.
The clinical outcomes assessed by MacNab criteria were excellent in 33 patients (73%), good in 10 patients (22%), fair in 2 patients (4%), and poor in none of patients. The average operative time was 63 minutes (range, 35 to 95 min- utes). The average intraoperative blood loss was 62 mL (range, 50 to 110 mL) derived from the operative records of anes- thesia. It should be stated that for most cases the blood loss was negligible (less than 50 mL). And these cases considered the blood loss to be calculated with 50 mL. All procedures were completed without blood replacement. Almost all pa- tients could walk at the day of surgery, except 2 patients who could ambulate at the next day of surgery. Patients stayed an average of 2.3 days (range, 2 to 7 days) in the hospital.
And none of patients had a dural tear, wound problem, recur- rent herniated disc, and other complications.
DISCUSSION
Numerous percutaneous and minimally invasive techniques have been developed for lumbar discectomy, including per- cutaneous nucleotomy, percutaneous laser disc decompres- sion, percutaneous endoscopic laser discectomy and endo- scopic discectomy1,2,8,17).
Outcome studies are necessary to validate the clinical effi- cacy of these new techniques and to show that they are at least or better than traditional methods. Percutaneous app- roaches to the lumbar spine for the treatment of disc disease have limited indications, primarily because the technique is restricted to those patients with contained lumbar disc herniation15,16). The Cochrane methodology used for meta-
analysis of randomized controlled trials showed that microdis- cectomy produced better results than percutaneous discec- tomy9). A recent review of randomized trials of the surgical management of lumbar disc prolapse identified three trials of percutaneous discectomy revealing moderate evidence that it produces poorer clinical outcomes than standard dis- cectomy or chymopapain10). In this same review, three trials showed no difference in clinical outcomes for microdiscec- tomy and standard discectomy.
In 1997, the introduction of microendoscopic discectomy (MED) system allowed spinal surgeons to reliably decom- press a symptomatic lumbar nerve root reliably via an endo- scopic minimally invasive surgical approach5-7). This system offers many advantages over other minimally invasive lum- bar discectomy techniques2,8,12,13)by reducing soft tissue trau- ma, allowing direct visualization of the nerve root and disc pathology, and allowing bony decompression.
However, there were limitations to the initial MED sys- tem. The endoscope was not reusable, image quality was inconsistent, and the working space within the tubular ret- ractor was limited. The next generation system called the METRx was developed to address these limitations. Com- pared with the MED system, the METRx system has addi- tional advantages, including increased image quality, dec- reased endoscopic diameter, variable tubular retractor size, increased available working room within the tubular retrac- tor, and decreased per case cost. Unlike percutaneous app- roaches, the METRx system allows surgeons to address not only contained lumbar disc herniations, but also sequestered disc fragments and lateral recess stenosis. Microdiscectomy with METRx-MD is a muscle-splitting approach that per- mits three-dimensional visualization. A operating micro- scope provides the optics and a series of tubular retractors provide the exposure. The minimally invasive tubular retrac- tor offers versatility in both tube diameter (14, 16, and 18 mm) and in length (3 to 10 cm), enabling the surgeon to individualize both of these parameters for each patient.
Currently, the majority of spine surgeons have not been trained to perform minimally invasive approaches during their formal training period, so they have to learn these pro-
rating scales, surgical approaches, selection criteria, and out- come interpretation. Success rates vary significantly (60%
to 97%) depending on the methodology of the study as well as criteria used to select the surgical candidate11,14). Long-term retrospective analysis of inpatient lumbar microdiscectomy has shown successful outcomes in 91% at 6 months, which declined to an 83% success rating at 10 years7). Clinical out- comes of our study assessed by MacNab criteria showed app- roximately 95% success rate of microdiscectomy using tubular retractor at the average follow-up period of 8 months, which was a similiar result with the above report.
Our study also showed the early recovery and short hos- pital stay of patients who underwent minimally invasive microdiscectomy using tubular retractor, which had simil- iar results of the Foley and Smith’s reports5-7).
It is critically important to understand the three-dimen- sional anatomy, particularly the neural anatomy, to avoid injury to these structures. If, in the minimally invasive tech- nique, a complication occurs intraoperatively, the surround- ing anatomy cannot be assessed and repaired as easily in com- parison to a more traditional open approach. For instance, dural tear tend to be somewhat mere difficult to repair within the confines of minimally invasive approaches compared to traditional open techniques. But we did not yet encounter with these complications in the series of this study.
Minimally invasive approaches to the spine depend sig- nificantly on the surgeon’s knowledge of surgical anatomy, as a smaller portion of that anatomy is directly visible com- pared to a traditional open approach. In order to maintain anatomic orientation during minimally invasive spinal sur- gery, the surgeon must be able to mentally recreate this
surgical technique and other minimally invasive spinal dis- cectomy techniques on clinical outcomes.
Our early clinical experiences would suggest that the mic- rodiscectomy using tubular retractor (METRx-MD system) may offer a useful treatment modality of lumbar herniated disc disease in the aspect of minimally invasive spinal surgery.
CONCLUSIONS
Microdiscectomy using tubular retractors is a useful and effective treatment modality for the treatment of lumbar herniated disc disease with the merits of minimally invasive spinal surgery. Further long-term, prospective, randomized study will be needed to fully evaluate the impact of this new surgical technique and other minimally invasive spinal dis- cectomy techniques on clinical outcomes.
REFERENCES
1. Brayda-Bruno M and Cinnella P: Posterior endoscopic discec- tomy (and other procedures). Eur Spine J, 9 (Suppl 1): S24-S29, 2000.
2. Choy DS: Percutaneous laser disc decompression (PLDD): Twelve years’ experience with 752 procedures in 518 patients. J Clin Laser Med Surg, 16: 325-331, 1998.
3. Dirksmeier PJ, Parsons IM and Kang JD: Microendoscopic and open laminectomy and discectomy in lumbar disc disease. Semin Spine Surg, 11: 138-146, 1999.
4. Findlay GF, Hall BI, Musa BS, et al: A 10-year follow-up of the outcome of lumbar microdiscectomy. Spine, 23: 1168-1171, 1998.
5. Foley KT and Smith MM: Microendoscopic discectomy. Tech Neurosurg, 3: 301-307, 1997.
6. Foley KT, Smith MM and Rampersaud YR: Microendoscopic
approach to far-lateral lumbar disc herniation. Neurosurgical Focus, 7: Article 5, 1999.
7. Foley KT, Smith MM and Rampersaud YR: Microendoscopic discectomy, in Schmidek HH (ed.): Operative Neurosurgical Tech- niques: Indications, Methods, and Results. Philadelphia, W.B. Saun- ders Co., 2000, ed 4.
8. Gangi A, Dietemann JL, Ide C, et al: Percutaneous laser disk decompression under CT and fluoroscopic guidance: Indications, techniques, and clinical experience. Radiographics, 16: 89-96, 1996.
9. Gibson JN, Grant IC and Waddell G: The Cochrane review of surgery for lumbar disc prolapse and degenerative lumbar spondy- losis. Spine, 24: 1820-1832, 1999.
10. Gibson JN, Grant IC and Waddell G: Surgery for lumbar disc prolapse (Cochrane review). Cochrane Database Syst Rev, 3: CD- 001350, 2000.
11. Howe J and Frymoyer JW: The effects of questionnaire design on the determination of end results in lumbar spinal surgery. Spine,
10: 804-805, 1985.
12. Marks RA: Transcutaneous lumbar diskectomy for internal disk derangement: A new indication. South Med J, 93: 885-890, 2000.
13. Maroon JC, Onik G and Vidovich DV: Percuttaneous discec- tomy for lumbar disc herniation. Neurosurg Clin N Am, 4: 125- 134, 1993.
14. McCulloch JA: Focus issue on lumbar disc herniation: Macro- and microdiscectomy. Spine, 21 (Suppl 24): 45S-56S, 1996.
15. Sahlstrand T and Lonnntoft M: A prospective study of preop- erative and postoperative sequential magnetic resonance imaging and early clinical outcome in automated percutaneous lumbar dis- cectomy. J Spinal Disord, 12: 368-374, 1999.
16. Siebert W: Percutaneous nucleotomy procedures in lumbar inter- vertebral disk displacement: Current status. Orthopade, 28: 598- 608, 1999.
17. Yeung AT: The evolution of percutaneous spinal endoscopy and discectomy: State of the art. Mt Sinai J Med, 67: 327-332, 2000.