영유아에서 철결핍빈혈의 평가 및 관리
김 순 기
인하대학교 의과대학 인하대학교병원 소아과학교실
Iron Deficiency Anemia in Infants and Young Children:
Evaluation and Management
Soon Ki Kim, M.D.
Department of Pediatrics, Inha University Hospital, College of Medicine, Inha University, Incheon, Korea
Despite a sharp decline in the prevalence of iron deficiency anemia (IDA) during the past several decades owing to better nutrition and iron-fortified foods, IDA continues to remain the most common disorder in the world. From about 4 months of age, iron stores are insufficient to maintain the rapidly expanding blood volume associated with normal growth. If there is no steady dietary supply, iron stores become depleted and IDA develops. It is known that iron deficiency (ID) may impair not only physical activity but also mental functions such as learning. Children with ID are found to have more psychomotor deficits and achieve lower scores in aptitude tests than those with normal iron status. Therefore, the detection and treatment, or preferably prevention of ID and IDA is imperative during late infancy, when increased vulnerability to ID coincides with the rapid growth and differentiation of the brain. The diagnosis of IDA is confirmed by the findings of a hemoglobin level <11 g/dL and low iron stores (serum ferritin level <12 μg/L, transferrin saturation <16%). Iron status should be evaluated in children who have risk factors for IDA such as low birth weight, premature baby, exclusive breastfeeding beyond 6 months of life, and weaning to whole milk and complementary foods without iron-fortified foods. With the management of underlying cause, oral iron therapy should be given to replenish iron stores. Parenteral therapy may be used in children who cannot tolerate or absorb oral preparations.
pISSN 2233-5250 / eISSN 2233-4580 Clin Pediatr Hematol Oncol 2013;20:1∼7
Received on March 23, 2013 Revised on April 5, 2013 Accepted on April 11, 2013
Corresponding author: Soon Ki Kim
Department of Pediatrics, College of Medicine, Inha University Hospital, 7-206, Shinheung-dong, Jung-gu, Incheon 400-103, Korea Tel: +82-32-890-2843 Fax: +82--32-890-2844 E-mail: [email protected]
Key Words: Iron deficiency anemia, Infants, Children, Complementary foods, Iron prepa- ration
서 론
경제성장과 식생활 개선에 따른 영양 상태의 개선, 모유 영 양의 지속, 철분 강화 분유 및 곡분의 사용 등으로 철결핍빈혈 (iron deficiency anemia. IDA)의 빈도는 많이 감소하였지만, IDA는 여전히 가장 흔한 영유아기 영양결핍증 중의 하나이다
[1-4]. 최근 모유 영양의 증가가 괄목할만하게 증가하였다[5].
모유 영양의 수많은 장점을 고려하건대, 이는 매우 바람직한 현상일 것이다. 그러나 이러한 장점의 극단에 대한 그림자인 가? 장기간 모유 수유로 인한 부작용을 종종 목격하곤 한다.
가장 극명한 예가 IDA 및 비타민 D 부족이 아닌가 한다.
건강한 아이는 출생 시에 체중 kg 당 75 mg의 철을 갖고
태어나는데, 대부분 마지막 3분기 동안에 축적된다. 정상분만
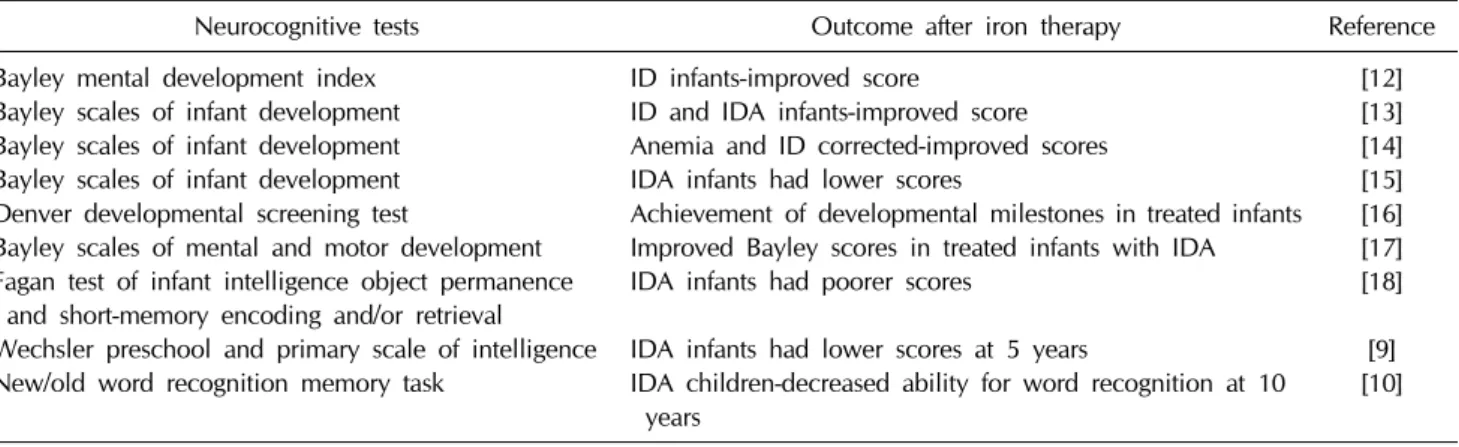
Table 1. Association between iron deficiency and neurocognitive development
Neurocognitive tests Outcome after iron therapy Reference
Bayley mental development index Bayley scales of infant development Bayley scales of infant development Bayley scales of infant development Denver developmental screening test
Bayley scales of mental and motor development Fagan test of infant intelligence object permanence
and short-memory encoding and/or retrieval
Wechsler preschool and primary scale of intelligence New/old word recognition memory task
ID infants-improved score
ID and IDA infants-improved score Anemia and ID corrected-improved scores IDA infants had lower scores
Achievement of developmental milestones in treated infants Improved Bayley scores in treated infants with IDA IDA infants had poorer scores
IDA infants had lower scores at 5 years
IDA children-decreased ability for word recognition at 10 years
[12]
[13]
[14]
[15]
[16]
[17]
[18]
[9]
[10]
ID, iron deficiency; IDA, iron deficiency anemia.
아의 철분상태는 모체가 심한 빈혈이 아니라면 모체의 철분 상태와 연관성이 없지만, 미숙아는 철분 저장량이 불충분하기 때문에 철분제 보충이 더욱 중요하다(뒤에 설명). 보통 만삭 아에서는 생후 3-6개월까지는 출생 시부터 갖고 있는 철분으 로 충당이 되지만, 출생 체중의 3배가 되면 저장된 철분은 거 의 소진된다. 이후에는 체외로부터 섭취하지 못하면 철결핍이 초래된다.
모유에 함유된 철은 생체이용율(bioavailability)이 높아 섭 취한 철분의 약 50%가 흡수된다. 그러나 모유에는 철이 소량 존재한다(0.3-0.5 mg/L). 모유에 약 0.4 mg/L의 철이 함유되 어 있고, 하루 1 L의 모유를 먹는다고 가정할 때, 영아가 흡수 하는 철분은 하루 0.2 mg에 불과하며, 이 시기의 왕성한 성장 에 필요한 0.55 mg에는 훨씬 못 미친다[6,7]. 따라서 장기간 모유 수유만으로는 섭취할 철분 자체가 부족하기 쉽다. 더구 나 모유 영양이 높은 흡수율로 인하여 철결핍을 예방하지만, 이유식 과정에서 반드시 거쳐야 하는 고형식의 첨가가 모유로 부터의 철분흡수를 방해한다. 특히 고형식이 모유 수유와 같 이 주어질 경우, 모유의 생체이용율이 감소한다. 이처럼 영유 아에 있어 철결핍의 주원인은 낮은 함량뿐만 아니라 흡수율도 낮기 때문이다.
생우유(cow’s milk)를 돌 전에 줄 경우, 철분이 적게 함유 되어 있고(0.5 mg/L), 흡수율도 모유에 비해 10% 정도로 작 고, 다른 음식내의 철분 섭취를 방해한다. 일부 영유아에 있어 생우유 내에 있는 열민감단백(heat labile protein)이 장출혈을 일으킬 수 있다. 생우유는 9-12개월 이후에 주기 시작하는 것 이 일반적으로 용인된 방법이다[8].
IDA는 영유아의 신경학적 발달, 운동, 행동발달에도 나쁜 영향을 미친다. 철분이 부족한 아이들은 영유아 발달검사에서 불량한 점수를 보였고, 철분 치료 후에 점수가 향상되었다
(Table 1). 철분 부족의 영향이 비가역적인가에 관해서는 논 란이 있는데, 나중에 지속적인 철분 보충을 하더라도 영속적 인 발달 장애의 위험이 있다는 보고들이 있다[9,10]. 이에 대해 서는 IDA로 진단된 영아의 사회적 배경이 불량하기 때문이라 는 주장도 있는 만큼[11], 이중 맹검법에 의한 좀더 큰 규모의 연구가 이루어져야 할 것이다. 어쨌든 두뇌발달의 대부분이 이 루어지는 영유아기에 있어서 철분부족에 의한 뇌의 인지기능 저하를 막기 위해서는 충분한 철분 공급이 있어야 할 것이다.
영유아기는 골격계의 빠른 성장으로 비타민 D가 상대적으
로 더 많이 필요하므로 비타민 D 결핍이 일어날 수 있는 시기
이다. 모유의 비타민 D 함량은 26-78 IU/L로 1일 권장량 400
IU에 비하여 현저히 적기 때문에 모유 수유를 주로 하는 영아
는 비타민 D 결핍의 위험도가 높고, 이러한 영아가 햇빛 노출
도 적다면 위험도는 더 높아진다[19,20]. 중국, 파키스탄, 방글
라데시, 아랍 에미리트에서도 모유수유를 주로 하는 영아에서
비타민 D 결핍증이 20-85%나 되었다[21-23]. 국내에서 비열성
경련으로 입원한 모유수유아에서 IDA와 함께 저칼슘혈증 및
비타민 D 결핍증이 동반되었다는 보고가 있고[24], IDA 가진
영유아에서 vitamin D 혈중 농도가 낮은 경우가 훨씬 많았다
[25]. 비타민 D 결핍증은 늦은 시기까지 모유수유만 주로 하는
영아에서 나타날 수 있는 영양 질환이고, 비타민 D를 공급하
는 것이 필요하다. Fig. 1의 사진은 필자 병원의 증례로서, 2
년 1개월 남아가 걸음이 늦고 심한 내반슬(genu varum)이 있
어 본원 정형외과를 통하여 소아과에 내원하였다. 환아는 13
개월 동안 모유수유하였고, 이유식을 5개월부터 먹였는데, 간
간이 분유를 시도하였으나 잘 안먹었다고 한다. 방문 시 검사
소견은 IDA (Hb 11 g/dL, MCV 72 fL, ferritin 6.12 ng/mL
이었는데, 이때는 아마도 2세가 넘었으므로, IDA가 상당히 개
선된 후의 검사결과로 해석됨)와 함께 혈청 25-hydroxychole-
Fig. 1. Radiographs of a rickets
patient at diagnosis, showing wid- ening of growth plate; cupping of distal radius, ulna and distal tibia;metaphyseal fraying; irregularity of metaphyseal border; underminerali- zation.
Fig. 2. Radiographs of a rickets
patient after treatment.calciferol이 17.2 ng/mL로 감소하였고, alkaline phosphatase 2,986 IU/L, parathyroid hormone 117.77 pg/mL로 증가되었 다. 치료 후, 6개월 후의 X-선 사진에서 골의 헤어짐(fraying) 이 개선된 것을 알 수 있다(Fig. 2).
이렇게 모유만의 영양이 강조된 이유의 하나가 아토피 피 부염과 음식 알레르기에 대한 우려 때문이었다. 아토피 피부 염의 위험인자를 가진 영아는 6개월 이전에 이유식을 시작하 는 경우 아토피 피부염의 발생률이 증가할 수 있으므로 6개월 이 지난 후에 이유식을 시작할 것을 권유하고 있지만, 6개월 까지 이유식을 안하는 것이 아토피피부염의 발생을 낮추는지 에 대해서는 논란이 있다[26,27]. 대규모의 연구에서 첫 4개월 만의 모유 영양만으로 충분할 것 같다는 결론을 내렸고[28], 최근 생후 4개월까지의 모유 수유는 아토피 피부염 발생을 낮 추는데 이롭지만, 2011년 전문가에 의한 안내서에 의하면, 고 형식 시작을 4-6개월 이후로 늦추지 말도록 권장하고 있다 [29]. 이유식을 6개월이 되어서 시작할 경우, 많은 아이들이 이유식을 제대로 필요한 만큼 먹지 않는다는 것이다[30]. 그러 므로 4-6개월 사이에 이유식을 시작하는 적응기간이 필요할
것으로 사료된다.
철결핍 및 IDA의 진단
우리나라 소아과학 교과서에는 12개월에 Hb 측정을 시행 하도록 하고 있고[31], 위험요소가 있을 경우에는 다른 기간에 도 시행하도록 권유하고 있다. 위험요소로는 미숙아, 저체중 출생, 납에 노출, 영아기에 생우유의 과다 섭취, 철분보충 없 이 장기간 모유만을 수유했을 때, 또는 식사문제가 있거나 성 장이 불량한 경우가 포함된다[32]. 그러나 Hb가 정상수치이더 라도 철결핍이나 부족은 알 수 없기 때문에 검사에 한계가 있다. 그러므로 가능한 기회가 있다면 철분영양을 평가하는 것이 확실한 방법일 것이다. Table 2에는 검사종목에 관하여 기술해 놓았다.
철분공급이 부족하면, 우선 철고갈(iron depletion)이 일어나
저장철이 감소한다. 철저장의 상태는 골수검사하여 Prussian
blue 염색을 하여 골수내의 hemosiderin을 관찰하는 것이 정
확하지만, 상용으로 수행하기에는 너무 침습적 방법이므로 보
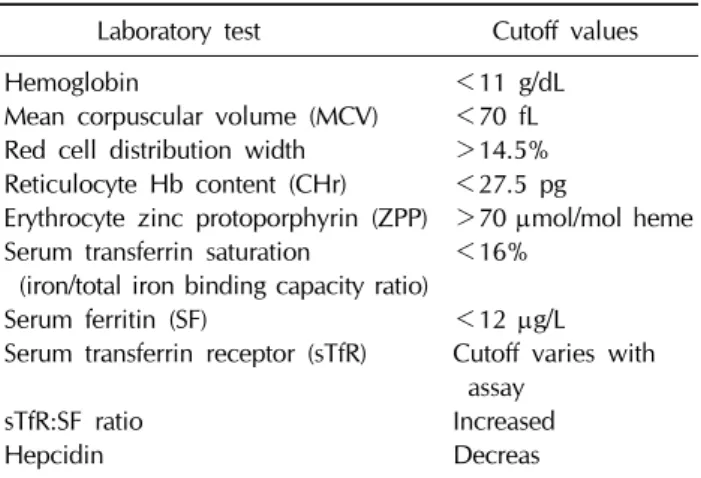
Table 2. Laboratory parameters of iron deficiency anemia in
toddlersLaboratory test Cutoff values
Hemoglobin
Mean corpuscular volume (MCV) Red cell distribution width Reticulocyte Hb content (CHr) Erythrocyte zinc protoporphyrin (ZPP) Serum transferrin saturation
(iron/total iron binding capacity ratio) Serum ferritin (SF)
Serum transferrin receptor (sTfR) sTfR:SF ratio
Hepcidin
<11 g/dL
<70 fL
>14.5%
<27.5 pg
>70 μmol/mol heme
<16%
<12 μg/L
Cutoff varies with assay
Increased Decreas
통 철저장 단백인 ferritin 검사로 대신하고, 12 ng/mL 미만인 경우 철결핍에 해당한다[33,34]. 혈청 ferritin은 감염이 없으면 비교적 정확한 상태를 반영하지만, 감염이나 염증성 질환(특 히 간질환), 결핵, 골수염, 만성 신장질환이나 신경모세포종 같은 종양에서 증가할 수 있다.
철저장이 다 소모되면, 2단계로, 철분이 고갈되어 Hb 합성 이 장애를 받기 시작하고, 효소내 철분 역시 감소하므로 정신 신체 및 면역에 관여하는 효소의 활성도가 감소한다. 혈청철 이 감소하고(<30 μg/dL), 혈청 transferrin은 증가하며(TIB C>350 μg/dL), 따라서 transferrin 포화도(iron/TIBC)가 16%
미만(어떤 이는 10% 미만을 주장)으로 떨어진다. Hb 합성을 위한 철의 이용이 제한되어 있으므로 free erythyrocyte pro- toporphyrin이 축적된다. 혈청철은 여러 가지 인자(식사로부 터 흡수, 감염, 염증, 하루 중 변동)에 의해 영향을 받기 때문 에 철저장을 정확하게 반영하지 않을지도 모른다. 철의 농도 는 아침에 높고 밤에 낮다. 그러므로 아침이나 이른 오후에 채혈하는 것이 더 좋다. TIBC 역시 영양부족, 염증, 만성감염 이나 암 질환에서 감소한다.
더 진행하면, 제3단계가 되는데, Hb를 생산하기에 필요한 철분을 갖고 있지 않은 상태가 된다. 그러므로 저구성, 저색소 성 빈혈은 심하게 철결핍의 영향을 받은 상태를 말한다. 빈혈 뿐 아니라, 평균적혈구용적(mean corpuscular volume, MCV), 평균적혈구혈색소량(mean corpuscular hemoglobin, MCH) 이 감소하고, 적혈구크기분포폭(red cell distribution width, RDW)은 상승한다. 그리고 heme precursor 인 free eryth- rocyte protoporphyrins (FEP) 증가한다(1-2세 영유아에서>
70 μg/dL RBC or >1.24 mmol/L RBC).
혈청 transferrin 수용체(transferrin receptor, TfR)는 조직의 TfR에서 떨어져나온 것이다. 조직 TfR는 인체내 모든 세포에
존재하는 transmembrane glycoprotein 인데 철을 가장 많이 필요로 하는 조직에 가장 높은 농도로 존재한다. 혈청 TfR는 조직내 철결핍 시 증가하므로, 철결핍의 초기 표지자(marker) 로서 유용하다. 혈청 TfR는 IDA에서 증가하고, 급성 감염 시 에 증가하지 않는다. 혈청 TfR/log of ferritin (sTfR-F index) 값이 증가하면 철결핍을 의미하고, 그렇지 않은 경우이면 만 성질환 빈혈을 의미한다.
Zinc protoporphyrin (ZPP)은 heme 합성의 최종 단계에서 철 대신 아연(zinc)이 protoporphyrin에 통합되어 형성된다.
철의 공급이 부족한 경우 ZPP는 증가하여 ZPP/heme 비가 증가한다. ZPP/heme 비는 Hb 합성 동안 철의 상태를 반영하 여 빈혈이 없더라도 철결핍을 탐지할 수 있다. ZPP와 EPP (erythrocyte protoporphyrin은 보통 ZPP로서 측정된다)는 철 결핍, 납중독이나 만성 감염시 증가하며, 최근의 철제복용에 영향받지 않는다.
망상적혈구 Hb 양(reticulocyte hemoglobin content, CHr) 은 망상적혈구 내의 철함유 단백의 농도를 flow cytometry로 측정한 것으로, MCV, MCH 감소에 비하여 먼저 감소한다. 즉, IDA가 발생하기 전인 iron deficiency erythropoiesis를 탐지 가능하다.
Hepcidin은 간에서 생성되는 호르몬으로 철 생체이용률을 조정함으로써 철의 필요량에 책임을 지는 역할을 한다.
Hepcidin은 장세포 및 대식세포의 세포표면의 ferroportin에 결합하여 세포에서 혈장으로의 철 이동을 차단하여, 혈청철을 감소시킨다. IDA 같은 적혈구생성이 가속화될 필요가 있을 경우에는 hepcidin 표현이 감소하여 철의 이용도가 증가하고 반면, 염증이나 이어지는 격리(sequestration)시에는 hepcidin 이 유도, 증가되어 침범한 병원체에 대한 면역반응을 증강시 킨다. 국내에서 소아를 대상으로 한 연구에서도 IDA에서 hepcidin이 감소하였다[35].
IDA의 치료 및 예방
1) 경구용 철분제
철결핍이나 IDA가 발견되면 철분 치료와 함께 영양상담이
필요하다. 혹자는 IDA가 있을 경우에 소고기를 추천하는데,
이것은 치료제가 아니고, 단지 철분이 약간 많은 음식일 뿐이
다. 치료는 철분제로 해야 한다. 보통 2가 철을 함유한 경구용
ferrous 염(sulfate, gluconate, fumarate)이 선택제이며 경제
적이다. 용량은 원소 철(elemental iron) 3-6 mg/kg/day를 공
복이나 식전 30분에 하루 3회로 나누어 주는데, 정상적인 십
이지장은 원소 철 25 mg으로 포화되기 때문이다. 음식이나
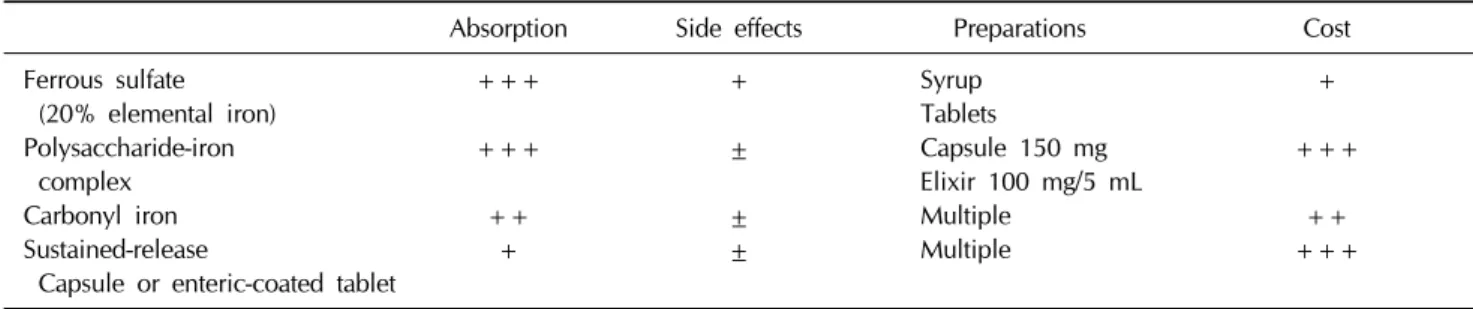
Table 3. Treatment of iron deficiency
Absorption Side effects Preparations Cost
Ferrous sulfate (20% elemental iron) Polysaccharide-iron
complex Carbonyl iron Sustained-release
Capsule or enteric-coated tablet
+++
+++
++
+
+
±
±
±
Syrup Tablets
Capsule 150 mg Elixir 100 mg/5 mL Multiple
Multiple
+ +++
++
+++
제산제가 철분 흡수를 감소시킬 수 있으므로 공복이나 식전 30분에 먹이는 것도 좋다. Hb가 정상화된 후에도 2-3개월 계 속 철분제를 공급하고, 약을 끊고 6개월 후에 Hb를 다시 측정 하는 것이 필요할 수도 있다. Ferrous sulfate는 원소철이 20%
로서, 식사 사이에 주스와 함께 주면 무난한 약이다. Ferrous sulfate로 Ferrimond
R시럽(보완)이 있고, 정제로는 훼로바-유
R(원소 철 80 mg/T), Hemocontin
R(원소 철 100 mg으로, 비타 민 B공유), 헤모스쿨
R등이 있다.
부작용으로, 위장 불쾌감(복통, 구역질), 설사, 변비, 더부 룩함 같은 증세가 있기 때문에 약을 잘 먹지 않으려는 아이도 있다. 변이 검게 나오고, 치아 착색이나 변비를 보일 수 있으 며, 과량 섭취에 의한 중독의 위험이 있다. Ferrous gluconate (50 mg의 원소 철 함유)는 부작용이 약간 적어서 초기 치료에 좋다.
보충 철의 흡수는 약의 형태에 따라 다르다(Table 3).
Multivitamin의 형태, 특히 칼슘이 사용될 경우 흡수가 저하된 다. 종합비타민과 미네랄은 식사나 차와 커피와 함께 복용 시, 철의 흡수는 감소한다. 비타민 C는 철 흡수를 증가시킨다.
Polysaccharide/iron complex는 앞에 말한 약제와는 달리, 넓은 pH에서 용해성이며 원소 철 150 mg처럼 많은 양을 주어 도 먹기 쉽다. 훼럼메이트
R, 훼럼키드
R, 훼럼포라
R, 훼로맥스
R등이 있다. Iron (III) hydroxide polymaltose complex 제제인 Ferrummate
R는 철(III) 100 mg/5 mL 비율로 함유되어 있고, 같은 성분으로 농축된 Ferrumkid
Rsyrup (45 mL/bottle)은 Fe3+로서 50 mg/mL 원소 철을 함유하고 있다.
철분치료 시, 가장 먼저 나타나는 반응으로 기분이 좋아지 고, 보챔이 감소하며 식욕이 증가하는데, 이는 세포내 철분 관련 효소의 회복 때문이다. 이어서 골수반응이 일어나고 4-5 일이 되어서 망상구가 최고로 증가하고, 철분 저장은 Hb가 증가된 후에야 비로소 일어난다.
치료 1개월 후에 Hb 측정을 반복하여 1 g/dL 이상 증가하 면 IDA를 확인할 수 있다. 혈색소 수치가 상승하지 않으면
다른 원인을 찾아보아야 한다. 약을 지시대로 안먹었거나 (noncompliance), 계속적으로 혈액이 어딘가로 새나가거나, 치료기간이나 용량이 부족할 때, 위 pH가 높을 때, 철흡수나 이용을 방해할 경우 또는 진단이 잘못될 경우가 있다. 하루 50 mg 이상의 철분을 보충하는 경우 흔한 불평 중 하나가 변비와 위장장애인데, 이로 인해 처방을 따르지 않는 것이 문 제이다.
2) 비경구용 철분제
경구용 철을 허용할 수 없거나 흡수할 수 없는 경우나 경구 복용을 지키지 않을 때, 철저장을 급격히 올리기 원할 때, 위 장관 흡수가 방해받을 때, 신장 투석 환자에서 erythropoietin 치료가 필요할 때, 정맥을 통하여 공급한다. 과거에는 high- molecular weight (HMW) iron dextran이 사용되었으나, 호 흡억제나 저혈압을 포함한 아나필락시스 반응이 종종 보고되 었다. 최근에는 low molecular weight (LMW) iron dextran이 나 iron gluconate가 도입되면서 급성기 부작용이 줄어들었으 나, 드물게 아나필락시스 반응을 보였다. 안전성 때문에 최근 에는 ferric gluconate나 iron sucrose가 널리 사용되고 있다.
Iron sucrose (예: Venoferrum
R, 100 mg Fe/5 mL)는 소아의
사용례가 제한되어 있긴 하지만, 소아와 청소년의 IDA에서도
안전하게 사용할 수 있다고 보고되었다[36,37]. 시험용량으로
소아의 경우 1일 사용량의 1/2 앰플을 투여한 후 15분 이상
부작용이 관찰되지 않으면 나머지를 투여한다. 시험용량의 투
여는 투여시마다 실시한다. 정맥철분제제 투여시 철 부족량에
따라 총 투여량을 정해야 하는데 일반적으로 총 투여량을 1주
일에 2-3회, 1회에 1-2 ample (100-200 mg)로 나누어 투여하
며 정맥 직접 주입하는 경우 10분 이상에 걸쳐 서서히 투여하
여야 한다. 필자의 경우, 근래 경구용 제제에 반응하지 않거나
장절제술을 받은 3명의 환자(방문 시 Hb 각각 4.5 g/dL, 5.3
g/dL 및 6.1 g/dL)에서 사용한 바, 효과적이었고, 특별한 부작
용은 없었다.
근육주사는 부작용(피부착색, 발진, 발열, 동통, 괴사, 천식, 치명적 anaphylaxis, 발한, 쇼크)이 많아 쓰지 않는다.
3) 수혈
가능하면 안 하는 것이 좋으나, Hb 4-6 g/dL 미만의 심한 빈혈이 있거나 동반된 감염이 치료반응을 저해할 경우에 줄 수 있다. 전혈 1 mL에는 0.5 mg의 철이 함유되어 있다.
4) IDA의 예방
이유식(보충식)의 시작시기는 6개월부터 하자는 의견과 4-6개월 사이에 시작하자는 주장으로 크게 나뉜다. WHO는 2001년에 적어도 첫 6개월 동안 모유만 먹이는 것을 모유 수 유의 일반적인 권장사항으로 채택하였고[38], 이런 원칙이 우 리나라에서도 대세인 듯하다. 미국 소아과학회에서는 완전 모 유 수유를 수유집단의 여건에 따라 달리 적용하고 있었지만, 최근 6개월의 주장이 강하게 되고[39], 유럽에서는 4개월 이전 에 이유식을 주지 말고, 또한 6개월 이후로 늦추지 말도록 주 장한다[40].
그러나 이 원칙에는 아이들에게 철분이 충분한 이유식을 먹이고, 아이들은 이러한 이유식을 충분히 잘 먹어야 한다는 가정이 전제되어야 한다. 우리나라의 경우 철분강화와는 거리 가 있는, 주로 집에서 만든 이유식이 주어지고 있기 때문에 철분 부족의 위험성이 매우 크다. 필자의 경험상 상당수 아이 들이 이유식을 잘 못 먹고, 만들어주는 이유식의 철분 함량은 불충분하였다[30]. 철분 외에도 아연이나 비타민 A, B6, D 영 양 역시 문제가 될 수 있다. IDA를 종종 접하는 우리 현실에 서는 모유만을 먹이는 영아는 6개월 이상 모유수유를 격려하 되, 4-6개월부터 이유식을 시도하고, 이유식에는 철분강화 음 식이 포함되어야 한다는 것이다.
생우유는 9-12개월 이후에 주기 시작하고[8], 돌이 지나서는 양을 늘이되, 하루 섭취를 500-700 mL 이하로 제한하는 것이 IDA를 예방하기 위해서 좋은 방법일 것이다.
2010년 미국 소아과학회 지침에 따르면, 6-12개월 영아는 하루에 11 mg의 철이 필요하고, 1-3세에서는 하루 7 mg이 필요하다. 국내에서는 5개월부터 3세까지 하루 8 mg의 철분 을 권장하고 있다[41]. 현실적으로 용이한 방법의 하나는 6개 월 이후 영아의 경우, 철강화 영아용 시리얼을 하루 두 단위 이상 먹이고, 9-12개월부터 고기를 갈아서 주는 것이다. 1세 이후에는 철분이 풍부한 음식을 격려하며, 생우유는 700 mL 까지만 먹이는 것이 안전할 것이다.
이유식 기간에 철분강화 분유를 하루 두 단위 이상 먹이지 않을 경우에는 1 mg/kg의 철분을 먹여야 할 것이다. 그러나
현실은 대부분의 부모가 철분제를 먹이지 않았다는 것이다 [42].
미숙아나 저체중출생아는 6개월 이전에 하루 2-4 mg/kg의 철을 공급하고 6개월 이전에 빈혈 선별검사를 실시한다. 1 kg 미만인 미숙아의 경우 3-4 mg/kg/day, 1 kg 이상의 미숙아는 2-3 mg/kg/day의 철분을 보충해야 한다.
결론적으로, 철결핍 및 IDA는 여전히 흔히 접하는 질환으 로, 현재의 영양방법으로는 위험성이 존재한다. 보충식 없이 모유영양을 6개월 고수할 것인지에 관해서는 충분한 연구가 진행되어야 할 것이며, 철결핍의 위험성이 있는 그룹은 철분 영양을 포함한 혈액검사가 필요할 것이다. 철분치료는 Hb가 정상화 된 후에도 2-3개월 지속하고, 영양교육 역시 병행하여 제공되어야 할 것이다.
참 고 문 헌