증 례
ISSN 2093-9272 일산병원학술지 2017;16(2):230-232230 Korean Journal of National Health Insurance Service Ilsan Hospital
후복막강 혈종 및 혈흉을 동반한 후천성 혈우병에서의 인터벤션 치료
연세대학교 의과대학 영상의학과1, 국민건강보험 일산병원 영상의학과2, 외과3
김동규
1, 김태환
2, 이형순
3Acquired Hemophilia with Bizarre Bleeding Presented as Concomitant Retroperitoneal Hematoma and Hemothorax
Dong Kyu Kim
1, Taehwan Kim
2, Hyung Soon Lee
31Department of Radiology, Yonsei University College of Medicine, Seoul,
Department of 2Radiology and 3Surgery, National Health Insurance Service Ilsan Hospital, Goyang, Korea
This report introduces a patient with acquired hemophilia who showed sudden onset spontaneous retroperitoneal hematoma initially, then followed by concomitant hemothorax and treated with endovascular radiologic intervention at first and hematologic replacement therapy with conservative management afterwards. Concomitant retroperitoneal hematoma and hemothorax is very rare, but is life-threatening. Therefore, a diagnosis of acquired hemophilia should be considered when sudden hemorrhagic event like this bizarre bleeding was developed in elderly patients. Also, if there is a possibility of acquired hemophilia, appropriate treatment is required not only immunosuppressive therapy to suppress production of the FVIII inhibitor, but also hemostasis to address hemorrhage. In conclusion, if we meet the patients with bizarre bleeding who had no prior history of coagulation disorder, a diagnosis of acquired hemophilia should be considered. And in these patients such as our case, the interventional embolization should be considered first to control active bleeding.
Key Words: Acquired Hemophilia, Retroperitoneal Hematoma, Hemothorax
책임저자: 김태환
10444 경기도 고양시 일산동구 일산로 100 국민건강보험 일산병원 영상의학과 전화 : (031)900-6965, 팩스 : (031)900-6967 E-mail: [email protected]
INTRODUCTION
Acquired hemophilia, caused by the development of auto- antibodies for the factor VIII, is a rare disease occurring in app- roximately one in 1 million people. Spontaneous unexpe cted bleeding is a most serious complication in these patients with acquired hemophilia, which is clinically distinct from inheri- ted hemophilia, being characterized by frequent skin and other soft tissue hematomas or rarely hemarthrosis.1 Also, spontane- ous retroperitoneal hemorrhage is unusual disease, most com- monly associated with patients in anticoagulation therapy, blee- ding abnormalities and hemodialysis. Therefore, it can be deve- loped in patients with hemophilia, von Willebrand disease, or antiphospholipid syndrome.2 Some people claimed that hemo
philia-associated hemorrhage could be preventable if clotting factor replacement therapy was infused to achieve and main- tain normal physiologic levels of factor VIII or factor IX, but such dosing was achieved rarely.
If the retroperitoneal hemorrhage is treated inappropria- tely, it could be associated with high morbidity and mortality, so the treatment choice is important. The treatment of retrope- ritoneal hematoma remains controversial. There was a study that compared the conservative management, endovascular in- tervention, open surgery and it concluded, if hemodynami- cally unstable, interventional radiology with endovascular em- bolization or stent-grafting is the primary treatment of choice.2
This report introduces a patient with acquired hemophilia who showed sudden onset spontaneous retroperitoneal hema- toma initially, then followed by concomitant hemothorax and treated with endovascular radiologic intervention at first and hematologic replacement therapy with conservative manage- ment afterwards.
김동규 외. 후복막강 혈종 및 혈흉을 동반한 후천성 혈우병에서의 인터벤션 치료
Volume 16 Number 2 December 2017
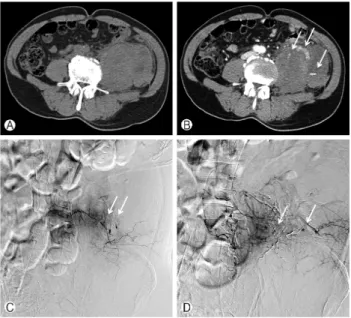
231 Fig. 2. Each APCT was done 1 day (A) and 10 days (B) after the embolization. Despite of successful embolization, aggravation of retroperitoneal hematoma was noted. But, there was no active blee- ding focus on follow up angiographies (not shown here). The possi- bility of hemophilia was considered after confirmation of sponta- neous hemothorax in both sides (C). Liquefaction of hematoma was noted on 2 months follow up CT scan (D).
Fig. 1. Initial APCT scan showed extensive left psoas hemorrha- gic muscular swelling with adjacent retroperitoneal hematoma (A) and multifocal bizarre bleeding foci (B, arrows). Emergent endo- vascular embolization of left lower lumbar arteries using NBCA glue and microcoils. As the initial CT scan, multifocal tiny blee- ding foci was confirmed (C and D, arrows).
CASE REPORT
A 60-year-old man who presented with acutely onset left side abdominal and back pain came to our emergency center.
He had no unusual medical history including bleeding ten- dency and coagulopathy except for seizure that controlled with medication. At the initial abdomen-pelvis computed tomogra- phy (APCT) scan, extensive left psoas muscular swelling with multifocal bizarre intramuscular bleeding foci and associated retroperitoneal hematoma was noted. Due to the getting wor- sened patient vital sign and multifocal retroperitoneal blee- ding with extensive hematoma, primary endovascular radiolo- gic intervention was attempted rather than surgical approach such as exploratory laparotomy. As the initial APCT scan, mul- tifocal active bleeding foci having somewhat bizarre feature was confirmed at left lower lumbar angiographies. By using N-butyl cyanoacrylate (NBCA) glue and microcoils, successful embolization was done to multiple peripheral bleeding foci of left lower lumbar arteries. But despite of successful emboli- zation treatment, the patient’s vital sign showed a pattern of improvement and deterioration. So we performed one day fol- low up APCT scan to looking for another bleeding focus. At the follow up CT scan, left psoas muscle hemorrhagic swelling was aggravated and the size of hematoma was increased (7
13 cm). But, the active contrast extravasation was not remar-
kable and hemodynamically, vital was stable after then. Until that time, physicians did not consider the possibility of acqui- red hemophilia, so only conservative management with fresh frozen plasma (FFP) transfusion was performed.
10 days after the embolization, the level of hemoglobin was rapidly downed (9.8 ->6.3 g/dL) and the patient’s vital sign deteriorated again. On follow up APCT, 22 cm sized hema- toma was noted in left retroperitoneal space with suspected active contrast extravasation. However, on angiogram of left lumbar artery and left internal iliac artery, there was no defi- nite active bleeding.
Follow up with conservative management was continued but the hemoglobin level was fallen to 5.9 g/dL, so the Chest CT was performed to check bleeding focus somewhere else.
On that study, hematoma with active contrast extravasation is found at right pleural cavity.
At that time, physicians considered the possibility of hemo- philia and on follow up laboratory tests, prolongation of acti- vated partial thromboplastin time (aPTT), reduced factor VIII level and positive of factor VIII inhibitor were found, which is compatible with acquired hemophilia. Due to the high risk of bleeding in patients with acquired hemophilia, open surgery was held off.
The patient underwent a recombinant activated factor VII (FVIIa) transfusion treatment and was on keeping hemoglobin level more than 10.0 g/dL. However, about 2 months later, the hemoglobin level decreased to 8.0 g/dL and the CT was per- formed. On CT images, the retroperitoneal hematoma extent was slightly increased in left iliopsoas area and the active blee-
DK Kim, et al. Acquired Hemophilia with Bizarre Bleeding Presented as CRH and Hemothorax
232 Korean Journal of National Health Insurance Service Ilsan Hospital ding focus was newly seen. But again, on angiogram, there was no definite active bleeding in left internal/external iliac and left lumbar artery.
The patient has undergone conservative management with FVIIa transfusion, and on the last follow up APCT, which was taken on 2017-02-28, the retroperitoneal hematoma was still noted, but the size was reduced without active contrast extra- vasation. In addition, the hemoglobin level has keep above 10.0 g/dL, and on the last laboratory tests, which was taken on 2017-05-19, the hemoglobin level was 13.7 g/dL.
DISCUSSION
There was a few reports about the concomitant retroperi- toneal hematoma with hemothorax in patients receiving war- farin and a non-steroidal anti-inflammatory drug,3 anticoagu- lant agents with or without anticoagulants4,5 or treated with un- fractionated heparin.6 However, to the best of our knowledge, there was no report dealing with spontaneous concomitant retroperitoneal hematoma and hemothorax in patients without any anticoagulant agents.
Patients with acquired hemophilia can present sudden onset of serious bleeding without prior history of coagulation disease.
Severe hemorrhage such as retroperitoneal hemorrhage can also occur, but it is relatively rare.7,8 Furthermore, cases presen- ting as hemothorax are also very rare (1% of casese).7-9
We observed a patient with acquired hemophilia who sho- wed large retroperitoneal hematoma and hemothorax. In this case, interventional angiogram was performed 3 times and only first angiogram showed bleeding focus.
Concomitant retroperitoneal hematoma and hemothorax is very rare, but is life-threatening. Therefore, a diagnosis of acquired hemophilia should be considered when sudden hemo- rrhagic event like this bizarre bleeding was developed in elderly patients. Also, if there is a possibility of acquired hemophilia, appropriate treatment is required not only immunosuppre- ssive therapy to suppress production of the FVIII inhibitor, but also hemostasis to address hemorrhage. For hemostasis, in the long run, therapies that activate other coagulation sys- tems such as recombinant activated FVII (FVIIa) or the active form of prothrombin complex concentrates (aPCC) derived from human plasma are necessary to control bleeding.10 Ho-
wever, prior to that, interventional intra-arterial embolization should be considered to control active bleeding first, because of high bleeding risk on open surgery.
In conclusion, if we meet the patients with bizarre bleeding who had no prior history of coagulation disorder, a diagnosis of acquired hemophilia should be considered. And in these patients such as our case, the interventional embolization should be considered first to control active bleeding.
REFERENCES
1. Lottenberg R, Kentro TB, Kitchens CS. Acquired hemophilia:
A natural history study of 16 patients with factor VIII inhibi- tors receiving little or no therapy. Arch Intern Med 1987;147(6):
1077-81.
2. Chan Y, Morales J, Reidy J, Taylor P. Management of spon- taneous and iatrogenic retroperitoneal haemorrhage: Conser- vative management, endovascular intervention or open surgery?
Int J Clin Pract 2008;62(10):1604-13.
3. Dzielski T, Nowicka D, Pasz P, Wojciechowska J. Hemothorax and retroperitoneal hematoma with the secondary posthemo- rrhagic anemia as a complication of oral anticoagulant and non- steroidal anti-inflammatory drug therapy. Pol Merkur Lekarski.
2000;8(47):335-6.
4. Mrug M, Mishra PV, Lusane HC, Cunningham JM, Alpert MA.
Hemothorax and retroperitoneal hematoma after anticoagula- tion with enoxaparin. South Med J 2002;95(8):936-9.
5. Fan W, Deng Z, Liu F, et al. Spontaneous retroperitoneal hemo- rrhage after hemodialysis involving anticoagulant agents. Journal of Zhejiang University Science B. 2012;13(5):408-12.
6. Moskovitz B, Braner B, Engel A, Kleinhaus U, Levin DR. Mul- tifocal bleeding due to anticoagulant therapy. Urol Int 1988;43 (1):53-5.
7. Franchini M, Gandini G, Di Paolantonio T, Mariani G. Acqui- red hemophilia A: A concise review. Am J Hematol 2005;80 (1):55-63.
8. Shima M. A survey of acquired inhibitors of blood coagulation in japan. Japanese Journal of Thrombosis and Hemostasis. 2003;
14(2):107-21.
9. Fukushima T, Mikane T, Ono D, et al. A case of acquired hemo- philia A with massive hmothorax. Journal of anesthesia. 2012;
26(2):262-264.
10. Huth-Kuhne A, Baudo F, Collins P, et al. International recom- mendations on the diagnosis and treatment of patients with acquired hemophilia A. Haematologica 2009;94(4):566.