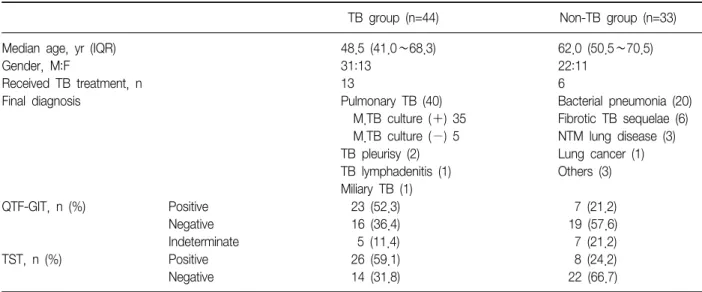
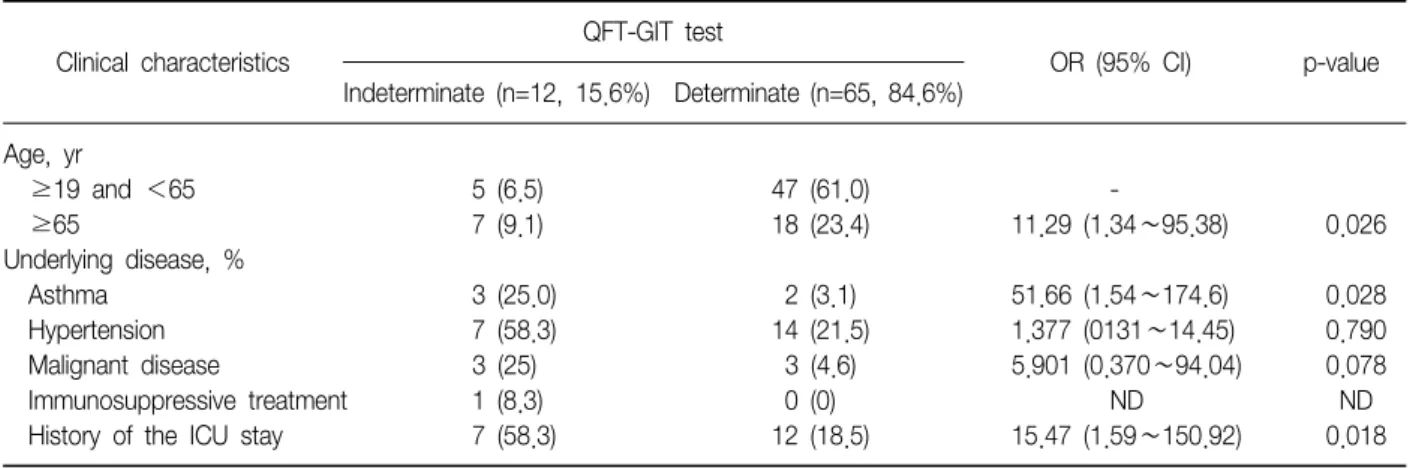
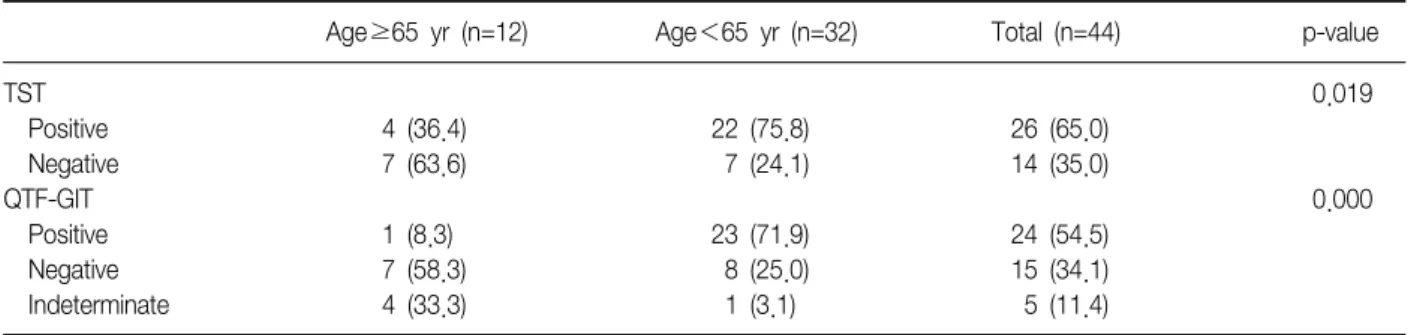
Factors Associated with Indeterminate and False Negative Results of QuantiFERON-TB Gold In-Tube Test in Active Tuberculosis
10
0
0
전체 글
(2)
(3)
(4)
(5)
(6)
(7)
(8)
(9)
(10)
수치

관련 문서
XRD analysis, surface roughness test, FE-SEM imaging, and biaxial flexural strength test were performed... Results: In the result of XRD analysis, an phase change occurred
period was prolonged unavoidably, (3) by explaining the risk factors associated with the failure to patients honestly, and subsequently performing
2. The finite element is calculating using tension test of uni-direction 0° and 90°, compression test of uni-direction 0° and 90° and shear test results and, the results
In the change of functional fitness, muscle strength and endurance, cardiopulmonary endurance, wits, and flexibility showed significantly increased results,
Results: In this research, in the group with fibromyalgia patients group, systemic lupus erythematosus patients group and without systemic autoimmune
The main effect according to the results of the repeated measures ANOVA on physical fitness based on test time showed a significant difference in grip
These results confirm that the 12-week swimming exercise based on the swimming program applied in this study has a positive effect on improvement of
• We can solve the statically indeterminate structure but it is more difficult (but possible!).. : Statically
