대 한 류 마 티 스 학 회 지
□
증 례
□ Vol. 12, No. 3, September, 2005― 231 ― 서 론
Sulfasalazine은 염증성 장 질환(inflammatory bowel
disease)의 치료에 흔히 쓰이는 약제이며 그 밖에 류 마티스 관절염, 척추관절병증 등에 사용되고 있다.
베체트병에서 위장관 병변이 발생한 경우에도 sul- fasalazine은 주요 약제로 사용된다1). Sulfasalazine의
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
<접수일:2005년 6월 20일, 심사통과일:2005년 8월 9일>
※통신저자:백 한 주
인천광역시 남동구 구월동 1198번지 가천의대 길병원 내과 류마티스분과
Tel:032) 460-3350, Fax:032) 469-4320, E-mail:[email protected]
정상 혈청 엽산 농도에서 발생한 Sulfasalazine에 의한 거대적아구성 빈혈
가천의과대학교 길병원 류마티스내과, 진단검사의학과*
김정곤․김태경․안정열*․최효진․방수미․백한주
= Abstract =
Sulfasalazine-induced Megaloblastic Anemia in Normal Serum Folate Level
Jung Gon Kim, M.D., Tae Kyung Kim, M.D., Jeong Yeal Ahn, M.D.*, Hyo Jin Choi, M.D., Soo Mee Bang, M.D., Han Joo Baek, M.D.
Departments of Internal Medicine and Laboratory Medicine*, Gachon Medical School Gil Medical Center, Incheon, Korea
Sulfasalazine produces a varied spectrum of adverse reactions on the hematopoietic system.
Sulfasalazine-induced megaloblastic anemia is very rare and a few cases have been reported in patients with inflammatory bowel disease. Most of them show a low serum folate level. The pathogenesis is known as folate deficiency by intestinal folate malabsorption, inhibition of folate enzyme, or hemolysis. We experienced a 43-year old female with Behcet’s disease, who presented with megaloblastic anemia having normal serum folate level after treatement of sulfasalazine (2 g/day for 3 months). Megaloblastic anemia recovered after withdrawal of the drug only.
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ Key Words: Sulfasalazine, Megaloblastic anemia, Serum folate level
― 대한류마티스학회지 제 12 권 제 3 호 2005 ―
― 232 ― 부작용 중 거대적아구성 빈혈이 염증성 장질환 환자 에서 드물게 보고되어 있으며, 엽산 결핍이 주요 기 전으로 알려져 있다2-4). 염증성 장질환이 아닌 베체 트병 환자에서 정상 혈청 엽산 수치를 보이며 sul- fasalazine 복용에 의해 생긴 거대적아구성 빈혈의 보 고는 없었다.
저자들은 베체트병으로 진단된 환자에서 혈청 엽 산 농도의 감소 없이 생긴 sulfasalazine에 의한 거대 적아구성 빈혈을 경험하여 보고한다.
증 례
환 자: 43세, 여자 주 소: 혈액 검사 이상
현병력: 환자는 5년 전 근위부, 원위부 지간 관절, 주관절, 슬관절 통증과 함께 재발성 구강내 궤양, 생 식기계 궤양, 여드름과 같은 피부병변, 홍반성 결절 로 베체트병을 진단받았다. 당시 시행한 pathergy 검 사는 음성이었다. 이후 colchicine 1.2 mg/day과 비스 테로이성 항 염증제를 투여하였고 입원 2년 전부터 는 구강 내 궤양이 악화되어 경구용 스테로이드를 추가 투여하였다. 입원 3개월 전 설사와 우하복부 통증을 호소하여 대장 내시경을 시행하였고 회맹판 부위에 두 개의 궤양이 있어 조직검사와 함께 항산 균 도말 검사를 시행하였으나 염증 외에 이상이 없
었다. 이후 sulfasalazine 2 g/day을 추가하고 경구용 스테로이드를 증량 투여하여 증상 호전을 보였다.
외래 추적 관찰 중 정기 혈액 검사에서 발견된 빈혈 로 입원하였다. 환자의 식습관은 정상이었으며 현재 복용 중인 약제 외에 다른 약제 복용력은 없었다.
사회력: 음주나 흡연의 병력은 없었다.
가족력과 과거력: 특이 사항은 없었다.
진찰 소견: 입원 시 만성 병색을 보였고, 활력 징후 는 혈압 110/70 mmHg, 맥박 76회/분, 호흡수 20회/분,
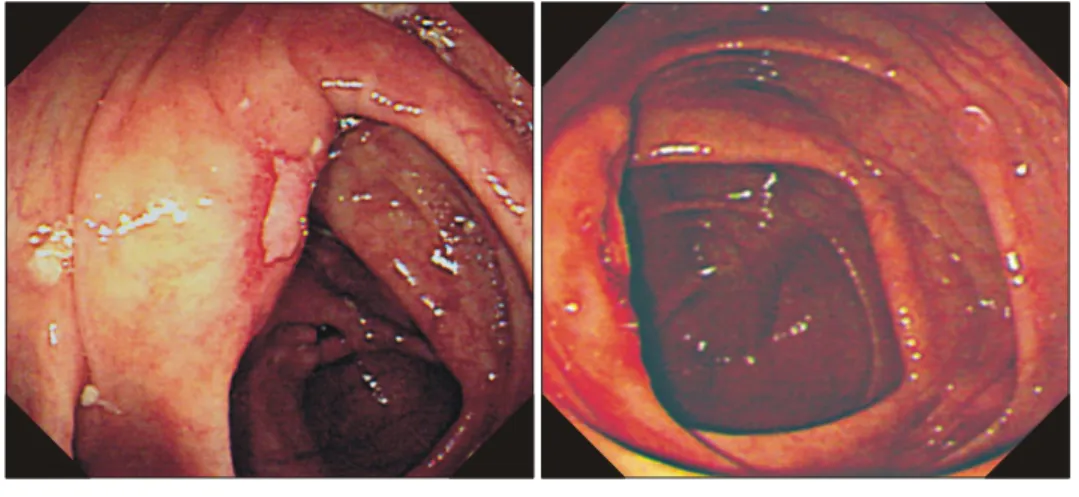
Fig. 2. Colonoscopic findings show that the previous ileocecal ulcer is disappeared.
3 months ago At admission
Fig. 1. Peripheral blood smear shows that macrocytic red blood cells are admixed with normocytic ones.
― 김정곤 외 : Sulfasalazine에 의한 거대적아구성 빈혈 ―
― 233 ― 체온 36.5oC였다. 결막이 창백하였으나 구강 내 궤 양, 피부 발진과 피하 결절은 없었다. 흉부 진찰 소 견은 정상이었으며 복부 진찰에서 장음은 정상이었 고 압통이나 반발 압통도 없었다. 흑색변이나 혈변 은 관찰되지 않았다.
검사 소견: 3개월 전 대장 궤양 발견 당시 혈색소 수치는 12.0 g/dL였다. 입원 시 말초 혈액 검사에서 혈색소 8.3 g/dL, 헤마토크리트 24.8%, MCV 112.6 fL, RDW 18.2% (참고치 11.5∼14.5%), 백혈구 4,290/
mm3, 혈소판 301,000/mm3, ESR 2 mm/hr, reticulocyte production index 0.85이었다. 혈청 LDH 446 U/L, hap- toglobin 22.2 mg/dL (참고치 30∼178 mg/dL), iron/
TIBC 216/ 306μg/dL, ferritin 94.03 ng/mL, cobalamin 781.6 pg/mL (참고치 200∼900 pg/mL), 엽산 6.36 ng/
mL (참고치 3∼20 ng/mL), uric acid 4.9 mg/dL이었고 간기능은 정상이었다. 직, 간접 Coombs 검사와 대변 잠혈 검사는 음성이었다. 말초 혈액 도말에서 대타 원적혈구(macroovalocyte), 적혈구부동증(anisocytosis), 변형적혈구증가증(poikilocytosis)을 보였고 과분엽 호중 구는 관찰되지 않았다(그림 1). 하부 위장관 출혈을 확인하기 위해 대장 내시경을 시행하였으나 정상이 었다(그림 2).
임상 경과: 약제에 의해 발생한 거대적아구성 빈 혈으로 진단한 후, sulfasalazine을 중지하고 경구용 스테로이드 10 mg/day와 colchicine 1.2 mg/day을 투 약하였다. Sulfasalazine 중단 10일 후 혈색소는 10 g/dL로 증가하였고, 1개월 후 12.9 g/dL이었으며 혈 청 엽산은 6.65 ng/mL로 큰 변화가 없었다. 약제 중 단 2개월 후 MCV는 97.2 fL로 정상화되었고 현재 외래에서 추적관찰 중이다.
고 찰
거대적아구성 빈혈의 원인은 cobalamin 결핍, 엽산 결핍, DNA 대사를 방해하는 약물, 대사성 질환 등 이다. Sulfasalazine은 아조 결합에 의해 5-aminosali- cylic acid와 sulfapyridine으로 구성된 물질로 대장에 서 박테리아에 의해 분리되어 주로 5-aminosalicylic acid가 치료 효과를 나타내며, 대부분의 부작용은 높 은 혈중 sulfapyridine 농도와 관련되어 있다5,6). Sulfa- salazine의 혈액학적 주요 부작용은 무과립증, 백혈구
감소증, 범혈구 감소증, 혈소판 감소증, 용혈성 빈혈, 혈색소혈증(sulfhemoglobinemia), 메트헤모글로빈혈증 (methemoglobinemia) 등이 있다7-9). 그 외 염증성 장 질환 환자에서 발생한 거대적아구성 빈혈의 증례들 이 소수에서 보고되었다2-4). Sulfasalazine이 거대적아 구성 빈혈을 일으키는 기전은 엽산 결핍에 의한 것 으로 이해되고 있으며, 엽산의 흡수장애, 음식물 엽 산인 pteroylpolyglutamate의 가수분해 억제, 간에서의 엽산 대사 억제, 그리고 경증의 용혈이 기전으로 알 려져 있다10,11). Swinson 등은 sulfasalazine 치료를 받 은 궤양성 대장염 환자의 2.5% (2/80)에서 엽산 결핍 과 거대적아구성 빈혈이 발생함을 보고하였다12). 베체트병에서 위장관 병변이 발생한 경우 sulfa- salazine과 스테로이드가 주요 치료 약제로 사용되고 있다. 하지만 광범위한 장질환을 동반하지 않은 베 체트병 환자에서 sulfasalazine에 의한 거대적아구성 빈혈의 예는 없었다. 본 증례에서 환자는 5년 전부 터 정기적으로 혈액 검사를 받아 왔으며 빈혈의 병 력이 없었고 그동안 생활 습관의 변화나 식습관의 변화가 없었다. 내원 3개월 전에 있었던 회맹판부 궤양에 의한 하부 위장관 출혈을 의심하여 시행한 대장 내시경은 정상이었고 잠혈 반응 검사에서 음성 이 나와 위장관 출혈에 의한 빈혈은 배제할 수 있었 으며 reticulocyte production index는 0.85로 저형성 빈 혈을 시사하였다. Pounder 등에 의하면 sulfasalazine (mean daily dose 2.5 g)을 투여 받은 궤양성 대장염 환자 50명 중 23명에서 용혈이 발생하였고 sulfasala- zine 1.5 g/day를 안전한 유지용량으로 제안하였다7). 본 증례에서 환자는 sulfasalazine 2.0 g/day를 복용하 고 있었으나 말초 혈액 도말에서 구상 적혈구, 헬멧 양 적혈구 등이 보이지 않고 정상 LDH 및 직/간접 Coombs 검사 음성을 보여 용혈에 의한 거대적아구 성 빈혈을 배제할 수 있었다.
거대적아구성 빈혈의 원인 약물로는 alcohol, cyclo- phosphamide, methotrexate, hydroxyurea, zidovudine, tri- methoprim, sulfasalazine, colchicine, neomycin 등이 있 다13). 환자가 복용 중이던 약물들 중에 원인이 될 수 있는 약물은 sulfasalazine과 colchicine이 있었다.
colchicine은 cobalamin 흡수 장애를 통해 거대적아구 성 빈혈을 일으키나 환자의 혈청 cobalamin은 781.6 pg/mL (200∼900 pg/mL)로 정상이었으며 5년 전부터
― 대한류마티스학회지 제 12 권 제 3 호 2005 ―
― 234 ― 지속적으로 복용했기 때문에 원인 약물일 가능성은 낮았다. 환자는 sulfasalazine 투여 후 3개월만에 거대 적아구성 빈혈이 발생하였으며 약제 중단과 함께 검 사실 소견이 정상으로 급격히 회복된 점으로 보아 저자들은 이 약제가 거대적아구성 빈혈의 원인이라 고 생각하였다. 기존의 증례들은 확연히 낮은 엽산 농도(0.8∼1.0 ng/mL)를 보고하였고 약제 투여 중지 나 엽산 보충 후에 혈청 엽산은 정상 수치로 빠르게 회복되었으나2-4), 본 증례에서는 혈청 엽산과 cobala- mine 농도가 정상이었고 약제 투여 중지 후에도 혈 청 엽산 수치는 6.65 ng/mL로 변화가 없어 기존 보 고와 차이점을 보였다. 최근 sulfasalazine은 세포막의 엽산 수송기(reduced folate carrier)를 억제하는 것으 로 알려졌다14). 저자들은 본 증례에서 sulfasalazine 에 의한 거대적아구성 빈혈의 발생 기전으로 혈청 엽산 농도는 정상이면서 세포내 엽산 농도의 결핍이 일어났을 것으로 생각하였다.
요 약
염증성 장질환, 류마티스 관절염, 척추관절병증 등 에 흔히 사용되는 sulfasalazine에 의한 거대적아구성 빈혈은 매우 드물며, 이 약제에 의한 엽산 결핍이 주요 기전으로 알려져 왔다. Sulfasalazine으로 치료 중 거대적아구성 빈혈이 의심되면 약제 투약을 중단 해야 하고 말초 혈액 도말검사나 혈청 엽산 농도, 혈청 cobalamin 측정 등의 검사를 실시하여 거대적 아구성 빈혈이 발생한 원인에 대해 관심을 가져야 한다.
저자들은 베체트병 환자에서 회맹판부 궤양이 있어 sulfasalazine 2 g/day로 3개월간 치료하던 중 엽산 결핍 을 동반하지 않은 거대적아구성 빈혈이 발생한 1예를 경험하였기에 문헌 고찰과 함께 보고한다.
REFERENCES
1) Kaklamani VG, Variopoulos G, Kaklamanis PG.
Behcet's disease. Semin Arthritis Rheum 1998;27:
197-217.
2) Kane SP, Boots MA. Megaloblastic anaemia asso- ciated with sulphasalazine treatment. Br Med J 1977;2:1287-8.
3) Schneider RE, Beeley L. Megaloblastic anaemia associated with sulphasalazine treatment. Br Med J 1977;1:1638-9.
4) Grieco A, Caputo S, Bertoli A, Caradonna P, Greco AV. Megaloblastic anaemia due to sulpha- salazine responding to drug withdrawal alone.
Postgrad Med J 1986;62:307-8.
5) Schröder H, Campbell DES. Absorption, metabo- lism and excretion of salicylazosulphapyridine in man. Clin Pharmacol Ther 1972;13:539-51.
6) DAS KM, Eastwood MA, MeManus JPA, Sireus W. Adverse reaction during salicylazosulfapyridine therapy and the relation with drug metabolism and acetylator phenotype. N Engl J Med 1973;289:
491-5.
7) Pounder RE, Craven ER, Henthorn JS, Banatyne JM. Red cell abnormalities associated with sulpha- salazine maintenance therapy for ulcerative colitis.
Gut 1975;16:181-5.
8) Taffet SL, Das KM. Sulfasalazine. Adverse effect and desensitization. Dig Dis Sci 1983;28:833-42.
9) Das KM. Pharmacotherapy of inflammatory bowel disease. Part 1. Sulfasalzine. Postgrad Med J 1983;
74:141-51.
10) Selhub J, Dhar GJ, Rosenberg IH. Inhibition of folate enzymes by sulfasalazine. J Clin Invest 1978;
61:221-4.
11) Franklin JL, Rosenberg IH. Impaired folic acid ab- sorption in inflammatory bowel disease: effects of salicylazosulfapyridine (Azulfidine). Gastroentero- logy 1973;64:517-25.
12) Swinson CM, Perry J, Lumb M, Levi AJ. Role of sulphasalazine in the aetiology of folate deficiency in ulcerative colitis. Gut 1983;22:456-61.
13) Colon-Otero G, Menke D, Hook CC. A practical approach to the differential diagnosis and evalu- ation of the adult patient with macrocytic anemia.
Med Clin North Am 1992;76:581-97.
14) Jansen G, Van Der Heijden J, Oerlemans R, Lems WF, Ifergan I, Scheper RJ, et al. Sulfasalazine is a potent inhibitor of the reduced folate carrier.
Arthritis Rheum 2004;50:2130-9.