https://doi.org/10.5763/kjsm.2016.34.2.169 pISSN 1226-3729 eISSN 2288-6028
Received: October 4, 2016 Revised: November 2, 2016 Accepted: November 9, 2016 Correspondence: Young-Joo Kim
Department of Rehabilitation Medicine, Inje University Sanggye Paik Hospital, 1342 Dongil-ro, Nowon-gu, Seoul 01757, Korea Tel: +82-2-950-1383, Fax: +82-2-938-4109
E-mail: [email protected]
This study was supported by the sports promotion fund from Korea Institute of Sport Science, Seoul Olympic Sports Promotion Foundation (KISS-15-A04004).
Copyright ©2016 The Korean Society of Sports Medicine
CC
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/
licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
운동유발성 고혈압 주자의 울트라 마라톤 달리기가 전구염증과 항염증 사이토카인 및 혈관내피세포
기능인자에 미치는 영향
순천향대학교 스포츠의학과
1, 인제대학교 상계백병원 재활의학과
2김철현
1
ㆍ강덕호1
ㆍ김영주2
Effects of Ultra-Marathon Running on Pro-inflammatory, Anti-inflammatory and Endothelial Function Factors in Athletes with Exercise-induced Hypertension
Chul-Hyun Kim 1 , Duk-Ho Kang 1 , Young-Joo Kim 2
1
Department of Sports Medicine, Soonchunhyang University, Asan,
2
Department of Rehabilitation Medicine, Inje University Sanggye Paik Hospital, Seoul, Korea
Running for a long distance in runners with exercise-induced hypertension (EIH) increases high blood pressure (BP) which causes myocardial burden, inducing elevation of cardiac markers. It is assumed to be associated with end- othelial dysfunction, but has not been studied so far. The purpose of this study is to exam the responses of anti-inflammatory, inflammatory, and endothelial regulation factors to 100 km ultra-marathon of athletes who have EIH. For this study, we obtain and analysis interleukin-6, tumor necrosis factor-α, interleukin-10 (IL-10), monocyte chemoattractant protein-1, creatine kinase and nitric oxide (NO) from 100 km ultra-marathoners before and right after the 100 km race. There were 40 volunteers who had ever won the 100 km marathon race before more than one time. They had the graded exercise test with measurement of BP for assessing EIH. Among them, eight athletes were categorized to normal control group (NCG) and 10 athletes were assessed by EIH group (EIHG). The graded exercise test with treadmill was performed for the maximal strenuous exercise and BP. EIH was diagnosed as
<140/90 mm Hg in normal and ≥210 mm Hg in maximal exercise. Marathoners including EIHG (n=10) and NCG
(n=8) participated in the race and blood extracted from them before the race and right after the race. As results,
EIHG had lower IL-10 than NCG during resting states and after the 100 km race EIHG had significantly lower NO
concentration than NCG. Therefore, the NO in the endothelial is inhibited during strenuous endurance exercise,
resulting in vasoconstriction with increasing the BP.
Keywords: Cardiovascular disease, Cytokines, Exercise-induced hypertension, Nitric oxide
서 론
규칙적인 운동은 심혈관 위험요인들을 개선시키고 심혈관질 환의 발병률과 사망률을 감소시킨다 1,2) . 또한 적당한 운동수행 은 항염증 기전으로 심장보호 효과를 주는 것으로 알려져 있다 3) . 반면 극심한 운동은 급성심근경색을 촉발하며 급사 및 동맥경 직도를 증가시킬 수 있다 4,5) . 마라톤이나 울트라 마라톤 같은 극심한 운동에서도 심혈관에 부정적 요인이 발생할 수 있는 상황에서 운동유발성 고혈압을 갖고 있는 주자들은 심혈관계에 더 높은 부담을 갖고 달릴 수 있다 . 운동유발성 고혈압은 안정 시에는 < 140/90 mm Hg로 정상이나 최대운동부하 검사에서 수축기 혈압이 ≥ 210 mm Hg 과도하게 상승하는 것을 말한다 6) . 운동유발성 고혈압은 향후 고혈압으로 이환될 비율이 높으며 , 뇌졸중과 심혈관 사망률의 위험예측 인자이다 7,8) .
이제까지 안정 시 고혈압에 대한 연구는 오랫동안 활발하게 연구되어 왔지만 운동 중 높은 혈압에 대한 연구는 안정 시 혈압만큼 그 중요성이 배제되어 왔다. 특히 급사율이 높은 극심 한 장거리 달리기 주자들 중 운동유발성 고혈압을 가지고 있는 경우 대한 연구들은 잘 이루어져 있지 않다 . 일반적으로 35세 이하의 젊은 선수들에게서의 급사는 비후성 심근증이 가장 높은 비율을 차지하며 35세 이상의 선수들은 70%가 관상동맥의 죽상경화에 의한 폐색이 주 원인으로 알려져 있다 9) . 죽상경화는 고혈압, 당뇨, 흡연, 산화된 저밀도 단백, 유전적 요인 같은 위험요인들이며 10) , 이 모든 과정은 염증성 반응으로 시작된다 11) . 죽상경화 내 위험요인들에 의한 염증 반응이 진행되면 경화 반 내에 활성화된 interleukin-2 (IL-2), interferon-γ, tumor necrosis factor-α (TNF-α) 등이 분비되고, 대식세포와 내피세 포에서 IL-1과 같은 사이토카인(cytokine)이 분비된다 12) . 혈관 내피세포 내의 활성화된 단핵구와 혈관 평활근 세포에서의 IL-6, IL-12, IL-18과 같은 사이토카인이 분비되며 13) 생성된 사이토카인은 다시 간에서 전신성 염증반응물질인 C-reactive protein (CRP)를 발현시킨다 14) . CRP는 죽상경화가 진행되면 혈중에 증가하게 되어 관상동맥질환의 위험을 증가시킨다 15) . 반면 염증의 정도를 완화시켜주는 항염증 사이토카인으로 IL-4, IL-10, monocyte chemoattractant protein-1 (MCP-1), soluble TNF receptors, IL-1 receptor antagonist 등이 있다 16) . 이들 사이토 카인은 심혈관외 근육과 혈액세포에서도 기원하는 것으로 알려져 있다 17) . 전구염증 사이토카인은 손상과 치료가 필요한
항염증 사이토카인은 운동유발 염증반응의 정도를 제한하는 기능을 한다 18) . 한편 혈관내피세포 기능인자로 산화질소인 nitric oxide (NO)는 강력한 혈관확장물질로 혈관의 이완 및 확장에 매우 중요한 역할을 하며 산화질소 활성이 저하될 경우 심혈관계 질환의 위험을 높이는 것으로 알려져 있다 19) . 최근 연구에 따르면 운동유발성 고혈압을 가지고 있는 마라톤 주자들은 경기 중 말초혈관의 후부하의 증가로 혈관수축 물질 의 증가와 함께 심근손상 지표와 심근스트레스 지표가 증가했 으며 20) , 울트라 마라톤에서는 운동유발성 고혈압 주자에게서 장시간 달리기가 말초동맥 혈관확장 장애로 인한 활동근의 혈류제한으로 근손상 지표인 creatine kinase (CK)와 염증 지표 인 high sensitive C reactive protein (hsCRP)이 증가한 것으로 보고했다 21) . 이러한 보고들은 운동유발성 고혈압 주자가 운동 중 높은 혈압을 보이는 것이 말초혈관확장 장애로 추측할 수 있지만 혈관확장과 관련된 중요한 NO의 발현에 대해서는 아직까지 연구된 바가 없다. 따라서 본 연구는 운동유발성 고혈압을 가지고 있는 주자의 장거리 달리기에서 염증 사이토 카인인 전구염증물질(IL-6, TNF-α)과 항염증물질(IL-10, MCP-1) 및 혈관내피세포 기능인자(NO)들을 통해 혈관의 생리 학적 반응을 연구하고자 하였다.
연구 방법
1. 연구 대상
본 연구는 100 km 울트라 마라톤을 1회 이상 완주한 경험이 있는 중년 남성들을 대상자로 하였다. 총 지원자는 40명으로 대회 2개월 전부터 운동부하 검사를 시행하였다. 운동부하 검사 전 안정 시 혈압은 편안한 자세로 앉아서 5분 간격을 두고 2번 측정하여 평균을 구하였으며 안정 시 혈압이 <140/90 mm Hg이면서 최대운동부하 검사 시 수축기 혈압이 ≥210 mm Hg 상승하는 자를 운동유발성 고혈압군(exercise-induced hypertension group, EIHG) 주자로 선정하였다 7) . 지원자 40명 중 대회당일 불참 10명, 중도 포기자 12명으로 최종 완주자는 18명이었다. 이 중 통제집단은 안정 시 혈압이 <140/90 mm Hg이면서 최대운동 시 수축기 혈압이 <210 mm Hg인 정상 혈압군(normal control group, NCG) 8명이 선정되었으며 운동유 발성 고혈압은 10명으로 분류되었다. 두 집단은 모두 비슷한
(NCG vs. EIHG,
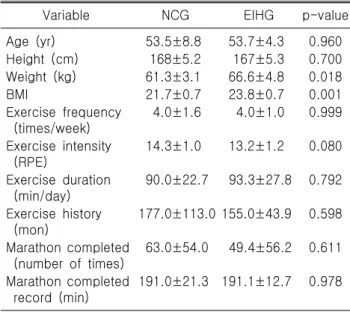
Table 1. Demographic characteristics of the subjects
Variable NCG EIHG p-value
Age (yr) 53.5±8.8 53.7±4.3 0.960 Height (cm) 168±5.2 167±5.3 0.700 Weight (kg) 61.3±3.1 66.6±4.8 0.018
BMI 21.7±0.7 23.8±0.7 0.001
Exercise frequency (times/week)
4.0±1.6 4.0±1.0 0.999
Exercise intensity (RPE)
14.3±1.0 13.2±1.2 0.080
Exercise duration (min/day)
90.0±22.7 93.3±27.8 0.792
Exercise history (mon)
177.0±113.0 155.0±43.9 0.598
Marathon completed (number of times)
63.0±54.0 49.4±56.2 0.611
Marathon completed record (min)
191.0±21.3 191.1±12.7 0.978
Values are presented as mean±standard deviation.
NCG: normal control group, EIHG: exercise-induced hyper- tension group, BMI: body mass index, RPE: rating of perceived exertion.
61.3±3.1 vs. 66.6±4.8 kg; p<0.05)과 BMI (NCG vs. EIHG, 21.7±0.7 vs. 23.8±0.7 kg/m 2 ; p<0.01)에서 EIHG가 NCG보다 유의하게 높았다 (Table 1). 채혈은 출발 2시간 전과 100 km 완주 직후에 실행하였다. 대상자 중 안정 시 혈압이 ≥140/90 mm Hg인 자, 심혈관질환자 , 신장, 간질환자 및 고혈압 약물 복용자, 12시간 (100 km 완주제한시간) 이내로 완주하지 못한 자는 연구에서 제외하였다 . 모든 대상자들의 개인정보는 설문지를 통해 얻어졌 으며 모든 연구를 실행하기 전 인제대학교 상계백병원 연구윤리 위원회에 윤리심의를 거쳐 연구를 실행하였다.
2. 운동부하 검사
운동부하 검사는 트레드밀(Medtrack ST 55; Quinton Instru- ment, Boston, MA, USA)을 이용하여 Bruce protocol에 따라 시행하였다. 호흡가스분석은 Quinton metabolic cart (Quinton Instrument)를 이용하였고, 15초 간격으로 시행하여 최대산소 섭취량(VO 2max ), 호흡교환율을 측정하였으며, 실시간 심전도 감시를 위하여 12채널 Quinton stress test system (Q4500, Quinton Instrument)을 이용하였다. 안정 시 혈압은 자동 혈압 측정기 (Me-del 412, Quinton Instrument)를 이용하여 3분 간격으로 두 번 측정하여 평균값으로 얻어진 혈압을 사용하였다. 운동 중 혈압은 각 운동 단계 2분에 측정하였으며 운동 중 혈압측정은 고성능 마이크폰을 상완 동맥에 위치시켜 헤드폰으로 수축기와
이완기음을 직접 듣고 측정하였다. 검사 중 세부적인 운동중단 요건은 American College of Cardiology/American Heart Associa- tion (AHA)의 지침에 근거하여 검사를 종료하였다 22) .
3. 혈액채혈 및 생리표적물질 분석
혈액채혈은 간호사에 의해 시행되었으며 채혈 장소는 대회 장소 오전 4–5시에 채혈 하였다. 실험대상자들은 울트라 마라 톤 출발 전 , 100 Km 완주 직후 주전정맥(antecubital vein)에서 Clinical and Laboratory Standards Institute guidelines 기준에 따라 채혈(1회 채혈양은 8 cc)하였다. 채혈된 표본은 염증과 항 염증 및 혈관조절인자에 대한 생리표적물질인 TNF-α, IL-6, IL-10, MCP-1, CK를 젤과 혈액응고 촉진제가 들어있는 진공상태의 SST 채혈관(BD vacutainer serum separator tube;
BD, Franklin Lakes, NJ, USA)에 담아 혈청분리하여 –70 o C 냉동고에 보관하였다가 측정하였다. TNF-α는 Quantikine HS human TNF-α kit (R&D, Minneapolis, MN, USA)를 이용하여 분석절차에 따라 분석액을 조제하여 microplate reader (Versa Max Corp., Sunnyvale, CA, USA)로 enzyme-linked immun- osorbent assay (ELISA) 법에 의해 정량 분석하였다. IL-6는 Quantikine HS human IL-6 immunoassay kit (R&D)를 이용하여 샘플을 조제하여 ELISA방식으로 정량하였으며, IL-10, MCP-1 은 human IL-10 Quantikine HS ELISA kit (R&D)와 Quantikine human MCP-1 kit로 시료를 준비하여 ELISA 방식으로 정량 분석하였다. CK는 Vacutainer SST Tubes (BD)를 이용하여 시료 를 조제하여 UV-assay (IFCC Granulat)법으로 분석하여 정량값 을 얻었다. 혈액 내 NO의 분석은 Griess methods의 절차로 분석하였다 23) . 채혈로 얻어진 혈액은 상온에서 30분 이상 응고 후 3,000 rpm에 10분 동안 원심분리한 후 분리된 상층액을 튜브에 옮겨 분석 때까지 혈청을 –70 o C에서 냉동 보관하였다.
얻어진 혈청은 total NO와 nitrate/nitrite assay (R&D)로 반응을 시킨 후 분광광도계(ELISA reader, 540 nm optical density; Versa Max Corp.)의 파장에서 값을 측정하였다. 혈액 분석은 녹십자 랩셀(Yongin, Korea)에 의뢰하여 분석하였으며 탈수에 의한 혈장용적변화는 적혈구용적(hematocrit)과 혈색소(hemoglobin) 로 계산했으며 적용은 혈장용적변화에 따라 계산하였다 24) .
4. 자료 분석
본 연구에서 얻어진 자료는 운동유발성 고혈압 주자와 정상
혈압 대조군을 대상으로 한 운동부하 검사 , 혈액분석, 일반적
인 사항들이었다. 이들 자료는 모두 기술통계인 평균과 표준편
차를 산출하였다. 산출된 자료는 생리표적물질별 집단과 전후
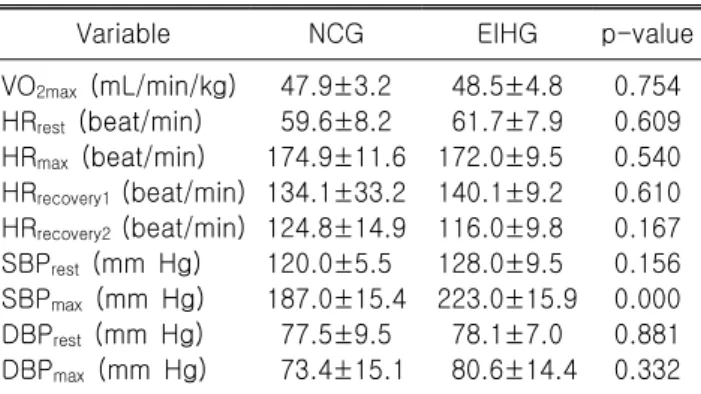
Table 2. Comparison on the graded exercise test between the groups
Variable NCG EIHG p-value
VO
2max(mL/min/kg) 47.9±3.2 48.5±4.8 0.754 HR
rest(beat/min) 59.6±8.2 61.7±7.9 0.609 HR
max(beat/min) 174.9±11.6 172.0±9.5 0.540
HR
recovery1(beat/min) 134.1±33.2 140.1±9.2 0.610
HR
recovery2(beat/min) 124.8±14.9 116.0±9.8 0.167
SBP
rest(mm Hg) 120.0±5.5 128.0±9.5 0.156 SBP
max(mm Hg) 187.0±15.4 223.0±15.9 0.000 DBP
rest(mm Hg) 77.5±9.5 78.1±7.0 0.881 DBP
max(mm Hg) 73.4±15.1 80.6±14.4 0.332 Values are presented as mean±standard deviation.
NCG: normal control group, EIHG: exercise-induced hyper- tension group, HR: heart rate, SBP: systolic blood pressure, DBP: diastolic blood pressure.
에 대한 차이와 상호작용효과를 확인하기 위해서 반복측정 이원변량 분석(repeated-measure two-way analysis of variance) 을 실시하였다 . 상호작용효과가 있는 생리표적물질은 사후개 별 검증을 위해서는 비모수적 방법을 이용하여 운동성 고혈압 군과 정상대조군 간에 평균 차 비교를 Mann-Whitney test로 분석하였고, 운동성 고혈압군과 정상대조군의 마라톤전과 직 후의 평균 차 검증은 Wilcoxon signed-rank test로 하였다. 모든 평균차 검증은 일방검증으로 유의수준을 p<0.05로 하였으며, 통계분석은 SPSS ver. 17.0 프로그램(SPSS Inc., Chicago, IL, USA)을 사용하였다.
결 과
1. 집단 간 운동부하 검사
운동부하 검사상에서 나타난 EIHG과 NCG의 결과는 Table 2에 나타난 바와 같다. 두 집단 간 VO 2max , heart rate (HR) rest , HR recovery1 , HR recovery2 , systolic blood pressure (SBP) rest , diastolic blood pressure (DBP) max 에서는 유의한 차이가 없었지만 SBP max
에서 EIHG (223±15.9)가 NCG (187±15.4)보다 유의하게 높았 다.
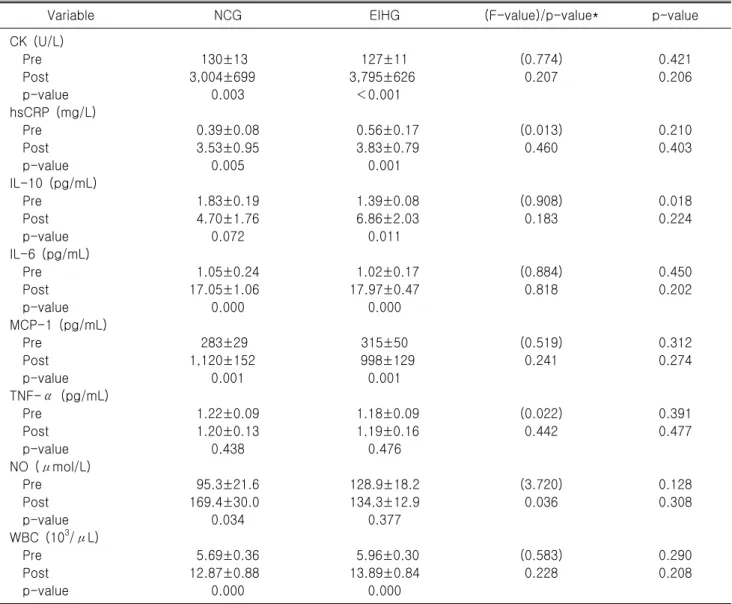
2. 100 km 전후와 집단 간 염증, 항염증 및 혈관
조절인자의 변화100 km 전후 집단 간 염증, 항염증 및 혈관조절인자의 변화 는 Table 3에 나타난 바와 같다. 100 km 출발 전 CK, hsCRP, IL-6, MCP-1, TNF-α, NO, 그리고 white blood cell (WBC)에서
두 집단 간 모두 유의한 차이가 없었으나 , IL-10에서 EIHG가 NCG보다 유의하게 낮은 것으로 나타났다(p<0.05). 100 km 완주 전후에서는 CK, hsCRP, IL-6, MCP-1, WBC가 두 집단 모두 각각 유의하게 증가하였고, TNF-α는 유의한 차이가 없었다. 반면, IL-10은 NCG에서 100 km 전후에 유의한 차이가 없었으나 EIHG에서만 100 km 전후의 유의한 증가를 나타내었 다. NO는 NCG가 100 km 완주 후에 유의하게 증가하였으나 EIHG는 100 km 전후에 유의한 차이가 없었다.
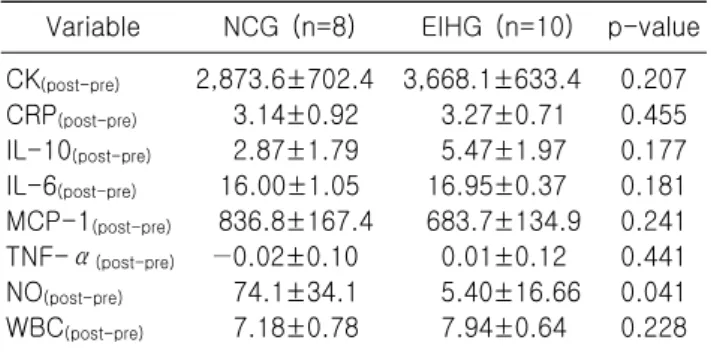
3. 100 km 전후 염증, 항염증 및 혈관조절인자의
집단 간 차이비교100 km 전후 염증, 항염증 및 혈관조절인자의 집단 간 차이 비교는 Table 4에 나타난 바와 같다. 항염증 인자와 염증 인자에 서 NO를 제외한 모든 항목에서 두 집단의 전후 차에 대한 값을 비교하였을 때 유의한 차이가 없었다 . 그러나 혈관조절 인자 특히 혈관의 확장을 유도하는 NO의 100 km 전후 차이 값을 비교하였을 때 EIHG가 NCG보다 유의하게 낮은 것으로 나타났다.
고 찰