Many problems are associated with joint reconstruction of total hip replacement for patients with developmental dysplasia of the hip; these include leg length discrepancy, failure of acetab- ular formation, developmental failure of the femur, muscular atrophy and pelvic imbalance on ambulation2,3,5-7,11-14,16-18,21). Particularly, complications increase as the extent of dislocation in the Crowe Classification gets more severe, depending on the degree of developmental dysplasia of the hip joint1). We per- formed cementless total hip arthroplasty with subtrochanteric shortening osteotomy in five patients with Crowe IV develop- mental dysplasia of the hip. The purpose of the current study is to introduce a surgical technique of total hip arthroplasty, by which a postsurgical neurologic deficit can be prevented and excellent clinical and radiological outcome can be obtained in patients with Crowe IV developmental dysplasia of the hip.
MATERIALS AND METHODS
Twelve of the two hundred thirteen hip joints, which under- went hip joint arthroplasty at our hospital from October 1995 through November 1997, were diagnosed as having secondary hip joint arthritis due to developmental dysplasia of the hip.
Among them, six hip joints from five patients belonging to the Crowe Classification IV were used as the subjects of the current study. An average following period was 61.2 months (range of 40 to 77 months).
1. Age, sex and preoperative conditions
All five patients were females. The age distribution ranged from 22 to 61 years with a mean age of 35.4. There were 2 patients with right hip joint involvement, 2 with left hip joint involvement and 1 with bilateral hip joint involvement. The average of preoperative leg length discrepancy was 4.1 cm (2.0 to 5.5 cm) and the mean preoperative Harris hip score was 67.1 (61 to 71) (Table 1).
2. Acetabular cup and femoral stem
The Duraloc 1200 series acetabular cup (DePuy, Warsaw,
466 466 466 466 Address reprint requests to
Kyoung-Ho Moon, M.D.
Department of Orthopedic Surgery, Inha University Hospital 7-206, 3-Ga Shinheung-dong, Jung-gu, Incheon 400-103, Korea Tel: +82.32-890-3663, Fax: +82.32-890-3099
E-mail: [email protected]
Purpose:The purpose of the current study is to introduce a surgical technique of total hip arthroplasty, by which a postsurgical neuro- logic deficit can be prevented and excellent clinical and radiological outcome can be obtained in patients with Crowe IV developmental dysplasia of the hip.
Materials and Methods:Twelve hip joints underwent hip joint arthroplasty at our hospital between October 1995 and November 1997 due to hip joint arthritis secondary to developmental dysplasia of the hip. Among them six hip joints of five patients which belonged to the Crowe Classification IV were operated using cementless total hip arthroplasty with subtrochanteric shortening osteotomy. The medi- cal records and radiographs of these five patients were reviewed. The average follow up period was 61.2 months (range of 40 to 77 months). Preoperative Harris hip score ranged from 61 to 71 (average, 66.2) points. Leg length discrepancy ranged from 2.0 to 5.5 (average, 4.1) cm.
Results: Harris Hip Score was improved to 95.3 (87 to 100) points at the last follow-up examination. The postoperative leg length was same bilaterally in five cases except for one case. Bone union in the osteotomy site was obtained three months after surgery. The radi- olucent area and findings of movement of the acetabular cup were not observed. Subcidence of the femoral stem or pedestal formation was not observed in five cases. In one case, revision was done for the subcidence of 5 mm or more with radiolucent line around the entire stem and pedestal formation at 48 months postoperatively. One case showed femoral nerve paralysis immediately after the surgery, which recovered completely in six months after the surgery.
Conclusion:This surgical technique is a useful method in total hip arthroplasty for the Crowe IV developmental dysplasia of the hip with- out permanent neurologic deficit.
Key Words: Developmental dysplasia of the hip, Total hip arthroplasty, Subtrochanteric shortening osteotomy
Cementless Total Hip Replacement Arthroplasty with Subtrochanteric Shortening Osteotomy in Crowe IV Developmental Dysplasia of the Hip
Kyoung-Ho Moon, M.D., Tong-Joo Lee, M.D., Seung-Do Cha, M.D., Young-Ha Park, M.D.
Department of Orthopedic Surgery, College of Medicine, Inha University, Inchon, Korea
U.S.A.) was used in three hip joints. The Duraloc 100 series� acetabular cup (DePuy, Warsaw, USA) was used in two hip joints including one revision case. The Harris-Galante�cup (Zimmer, Warsaw, U.S.A.) was used for the one hip joint. A S-ROM� femoral stem (DePuy, Stanford, U.S.A.) as a femoral stem was used for 4 hip joints. The AML�femoral stem (DePuy, War- saw, U.S.A.) was used for two hip joint. The one case of these was used for revision case.
3. Surgical procedure and postoperative manage- ment
All surgeries were performed by the first author and the pos- terior lateral approach was used in the lateral decubitus posi- tion for all the cases. In all cases, the sciatic nerve was identified and the proximal segment of the nerve was retracted medially in order to prevent the sciatic nerve damage during the surgery.
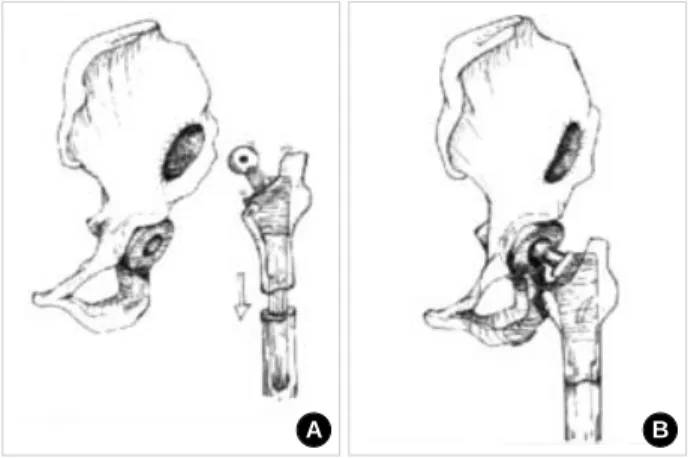
The acetabular cup was then fixed at the true acetabulum after the subtrochanteric osteotomy was done (Fig. 1) and proximal segment was displaced upward (Fig. 2A). A bone graft using the autogenous femoral head was performed for one case where bone grafting was necessary due to severe acetabular defect. A femoral stem was inserted into the proximal segment, and
bone shortening was carried out in the distal segment at the location where leg length discrepancy could be maximally cor- rected in order to avoid excessive tension on the sciatic nerve and by referencing the radiological measurement of the short- ening amount compare to the healthy femur (Fig. 2B). The femoral stem was inserted into distal segment of the femur
Case Age/Sex Side f/u (m) Preop.
LLD* (cm) Postop. LLD (cm) Preop. HHS� last f/u HHS Bone shortening (cm)
Polyethylene wear rate (mm/year)
1 26/F Both 62 None 0 71 100 4.0 0.204
2 22/F Right 65 5.5 1.0 67 97 3.0 0.210
3 61/F Left 62 2.0 0 61 87 4.0 0.043
4 41/F Right 77 4.0 0 62 94 4.0 0.215
5 27/F Left 40 5.0 0 71 98 3.5 0.135
*LLD: Limb length discrepancy. �HHS: Harris hip score.
Table 1.Case Summary
Fig. 2.(A) The proximal segment of the femur was displaced up- ward. The acetabulum was made at the true acetabular site. (B).
The acetabular component was placed in the true acetabular site.
Femoral trial was inserted in the proximal segment of the femur.
And then proper length of bone was removed at the distal seg- ment of femur to prevent stretching of the sciatic nerve.
A B
Fig. 1.(A) Schematic diagram shows Crowe IV congenital dyspla- sia of the hip. (B) Osteotomy was performed at the subtrochanter- ic area of the femur.
A B
Fig. 3.(A) The true femoral component was inserted into the femur.
(B) The femoral head was reduced at the acetabular component.
A B
after deciding how much altered anteversion angle of the proxi- mal femur should be corrected following investigation on sta- bility of the artificial hip joint and then, the hip joint was reduced (Fig. 3).
A partial weight bearing using two crutchs was permitted for 6 weeks after fixing it with a hip spica cast. Total weight bearing was permitted when bone union was judged to be radi- ologically completed in the osteotomy site.
4. Clinical and radiological evaluations
Harris hip score9)was used for clinical evaluation of the hip joint.
Anterior-posterior and lateral radiographic findings of the hip joint were examined immediately after the operation, and postoperatively at 6 weeks, 3 months, 6 months, and every one year after then. Evaluations were done by dividing the femoral component into the seven zones of Gruen8)and by dividing the
A B
Fig. 4. (A) This shows preoperative radiograph of a 22-age-old female. (B) The AP radiograph shows the last follow-up radiograph.
C
A B
Fig. 5. (A) This shows preoperative radiograph. (B) The AP radio- graph shows pre-revision radiograph. (C) The AP radiograph shows the last follow-up radiograph.
acetabular cup into the three zones of DeLee and Charnley4). Furthermore, bony union at the osteotomy site was observed.
The polyethylene wear was evaluated using Martell’s method19).
RESULTS 1. Evaluation of clinical functions
Harris hip score was improved to 95.3 (87 to 100) points at the last follow-up examination. The score of the revision case was 67 points preoperatively and 97 points at the last follow-up after revision. The postoperative leg length was same bilateral- ly in five cases except for one case in which the leg length dis- crepancy was 1 cm postoperatively. The actual average length- ening of the affected side was 3.6 cm (2.0 to 4.5).
2. Radiological evaluation
In all cases, bone union at the osteotomy site was obtained in three months after the surgery. The radiolucent area and findings of movement of the acetabular cup were not observed. Radiolu- cent line around the femoral stem were observed in hips oper- ated with S-ROM stems at zones 2, 3, 4, 5 and 6. Radiolucent line of 1 mm or less was observed at zone 4 in the two cases operated with the AML stem. Endosteal new bone formation was observed in five cases. Subcidence of the femoral stem or pedestal formation was not observed in five cases. In one case, revision was done for the subcidence of 5 mm or more with radiolucent line around the entire stem and pedestal formation at 48 months postoperatively. In this revision case, the S-ROM femoral stem was replaced with a AML stem. The average polyethylene wear rate was 0.168 (0.043-0.215) mm/year.
3. Complications
During the insertion of the femoral stem, a linear fracture occurred at the proximal femur in one case and at the distal femur in one case. Those fractures were fixed with Dall-Miles steel wires. One case showed femoral nerve paralysis immedi- ately after the surgery, which recovered completely in six months after the surgery.
CASE REPORT 1. Case 1
A 26-year-old female with bilateral developmental dysplasia of the hip Crowe IV scored 71 points bilaterally in the Harris Hip Score before surgery, and there was no leg length discrep- ancy (Fig. 4A). Bilateral total hip replacement was performed simultaneously and bone shortening of 4.0 cm was carried out bilaterally using a Duraloc 1200�cups and a S-ROM�femoral
stems. Bone union was obtained in the osteotomy site three months after surgery. During the insertion of the femoral stem, a linear fracture in the right proximal femur developed, which was fixed with Dall-Miles steel wire. Partial paralysis of left femoral nerve was observed postoperatively, which recovered completely in six months after surgery (Fig. 4B). At the last follow-up, the Harris hip score on both sides was 100 points.
2. Case 2
A 22-year-old female with developmental dysplasia of the hip Crowe IV on the right side scored 67 points in the Harris hip score before surgery and the right lower limb was about 5.5 cm shorter than the left limb (Fig. 5A). A Harris-Galante� cup and a S-ROM�stem were used and an approximately 3.0 cm bone shortening was carried out. After surgery, the leg length discrepancy was improved to 1.0 cm (Fig. 5B). The revision was done for the subcidence of stem by 5 mm or more with radiolucent line around the entire stem and pedestal formation at 48 months postoperatively. The S-ROM�femoral stem was revised with a AML stem. The Harris hip score at the last fol- low-up was 97 points.
DISCUSSION
The total hip replacement performed for the patients with developmental dysplasia of the hip has been known to have many complications and unfavorable outcome as compared with that of total hip arthroplasty carried out for degenerative arthritis2,3). Particularly in the case where the femoral head is completely dislocated from the true acetabulum as in the Crowe IV rating, the acetabulum is quite inadequately formed and filled with fibrous fatty tissues. Moreover, the dislocated femoral head has a short femoral neck, and the anteversion angle is increased, resulting from the formation of the pseudo-acetabu- lum above the thin wall of the ileum. Hence, operation is diffi- cult and the clinical result is not favorable15). The location of the acetabular cup in the developmental dysplasia of the hip joint has been a controversial issue. According to Linde and Jensen17), the more severe the extent of dislocation of the femoral head before the surgery, the higher the frequency of dissocia- tion of the acetabular cup. Harris et al.10)asserted that the exact positioning of the acetabular cup within the true acetabulum was important. Linde and Jensen17)stated that the frequency of dissociation of the acetabular cup would be higher in cases where the acetabular cup was not positioned within the true acetabulum. These authors tried to position the acetabular cup exactly within the true acetabulum for all cases. In order to augu-
ment the bony defect of the superolateral part of the acetabular cup, autogenous grafting using a resected femoral head is com- monly employed. Also, the medialization of the acetabular cup can improve the inadequacy of the acetabular cup. Nevertheless, penetrating through the inner wall is undesirable. In this inves- tigation, an autogenous grafting was used in one case, and in the remaining five cases, the bony defects of the acetabulum was improved by using medialization. With respect to the method of pulling the femur down to the new joint location, an iliop- soas muscular resection and advancement of abductor muscle with joint membrane excision are necessary. When superior dislocation of the femoral head is so severe, the above method is insufficient. In all cases of the current study, reduction of the femoral head into the acetabular cup could be achieved without sciatic nerve palsy, and it was possible to correct the abnormal femoral anteversion angle with subtrochanteric shortening osteotomy20). The finding of partial paralysis of the femoral nerve shown in one case was thought to be a traction injury during the surgery. It is important to inform the patient that there may be leg length discrepancy or limping even after the surgery. It is more important to prevent the neurological paralysis than to correct the lower limb length during the surgery. In this inves- tigation, the postoperative leg length discrepancy was only 1.0 cm in one case and the leg length discrepancy could be correct- ed in the remaining five cases.
CONCLUSION
For the cementless total hip replacement of patients with Crowe IV developmental hip dysplasia, subtronchanteric short- ening osteotomy is a useful method to correct leg length discrep- ancy without permanent nerve paralysis. Excellent clinical and radiological results were obtained in medium-term follow-up.
REFERENCES
1. Cameron HU, Botsford DJ and Park YS: Influence of the Crowe rat- ing on the outcome of total hip arthroplasty in congenital hip dysplasia. J Arthroplasty, 11: 582-587, 1996.
2. Charnley J and Feagin JA: Low-friction arthroplasty in congenital sub- luxation of the hip. Clin Orthop, 91: 98-113, 1973.
3. Crowe JF, Mani VJ and Ranawat CS: Total hip replacement in con- genital dislocation and dysplasia of hip. J Bone Joint Surg, 61-A: 15-23, 1979.
4. DeLee JG and Charnley J: Radiologic demarcation of cemented sockets in total hip replacement. Clin Orthop, 121: 20-32, 1976.
5. Dooley BJ, Clifford MJ and Hjorth DP: Total hip replacement com-
bined with bone grafting for acetabular dysplasia causing severe osteoarthri- tis of the hip joint. Aust NZ J Surg, 55: 195-198, 1985.
6. Fredin HO and Unander-Scharin LE: Total hip replacement in con- genital dislocation of the hip. Acta Orthop Scand, 51: 799-802, 1980.
7. Gerber SD and Harris WH: Femoral head autografting to augment acetabular deficiency in patients requiring total hip replacement. J Bone Joint Surg, 68-A: 1241-1248, 1986.
8. Gruen TA, Mcneice GM and Amstutz HC:“Mode of failure”of cemented stem-type femoral components: a radiographic analysis of loos- ening. Clin Orthop, 141: 17-27, 1979.
9. Harris WH: Traumatic arthritis of the hip after dislocation and acetabu- lar fracture: Treatment by mold arthroplasty. An end-results study using a new method of result evaluation. J Bone Joint Surg, 51-B: 239-242, 1992.
10. Harris WH, Crothers O and Oh I: Total hip replacement and femoral- head bone-grafting for severe acetabular bone deficiency in adults. J Bone Joint Surg, 59-A: 752-759, 1977.
11. Hartofliakidis G, Stamos K and Ioannidis TT: Low friction arthro- plasty for old untreated congenital dislocation of the hip. J Bone Joint Surg, 70-B: 182-186, 1988.
12. Herold HZ: Congenital dislocation of the hip treated by total hip arthro- plasty. Clin Orthop, 242: 195-200, 1989.
13. Hess WE and Umber JS: Total hip arthroplasty in chronically dislocat- ed hips: follow-up study on the protrusio socket technique. J Bone Joint Surg, 60-A: 948-954, 1978.
14. Jensen JS, Repten JB and Arnoldi CC: Arthroplasty for congenital hip dislocation: technique for acetabular reconstruction. Acta Orthop Scand, 60: 86-92, 1989.
15. Kavanagh BF, Shaughnessey WF and Fitzgerald RH: Congenital dislocation of the hip, In: Morry BF ed. Joint replacement arthroplasty. 1st ed. New York, Churchill Livingstone: 739-748, 1991.
16. Kolmert L, Persson BM and Pettersson H: Hip arthroplasty for con- genital dislocation. Acta Orthop Scand 57: 407-412, 1986.
17. Linde F and Jensen JS: Socket loosening in arthroplasty for congenital dislocation of the hip. Acta Orthop Scand, 59: 254-257, 1988.
18. Lued KHD and Termansen NB: Hip replacement for congenital dislo- cation and dysplasia, Acta Orthop Scand, 56: 464-468, 1985.
19. Martell JM and Berdia SM: Determination of polyethylene wear in total hip replacements with use of digital radiographs, J Bone Joint Surg, 79-A: 1635-1641, 1997.
20. Sponseller PD and McBeath AA: Subtrochanteric osteotomy with intramedullary fixation for arthroplasty of the dysplastic hip. J Arthroplasty.
3(4): 351-354, 1988.
21. Woolson ST and Harris WH: Complex total hip replacement for dys- plastic or hypoplastic hips using miniature or microminiature compo- nents. J Bone Joint Surg, 65-A: 1099-1108, 1983.
목 적 :선천성 고관절 탈구의 정도가 가장 심한 Crowe IV 환자에서 무시멘트 고관절 전치환술과 동반하여 전자하 단축 절골술을 시행하여 신경 마비 없이 하지 부동을 교정하고 임상적 및 방사선적으로 좋은 결과를 얻었기에 수술 기법을 소개하고자 함에 있다.
대상 및 방법 : 1995년 8월부터 1997년 11월까지 본원에서 고관절 전치환술을 시행받은 213 고관절중 선천성 고관절 탈구에 의한 이차성 고 관절염으로 진단받고 Crowe 분류 IV에 해당하는 여섯 고관절 다섯 명을 환자를 대상으로 하였으며 무시멘트 고관절 전치환술과 동반하여 전 자하 단축 절골술을 시행하였다. 평균 추시 기간은 61.2개월(40-77개월)이었다. Harris hip score는 수술 전 평균 66.2점(61-71점)이었으며 하지 부동은 수술 전 평균 4.1 cm (2.0-5.5 cm)이었다.
결 과 : Harris Hip Score는 수술 후 마지막 진찰시 평균 95.3점(87-100점)으로 증가하였다. 하지 부동은 수술 후 1예를 제외한 4예에서 같았다. 모 든 예에서 수술 후 3개월에 절골 부위의 골유합을 얻었고 추시 관찰상 비구 컵의 방사선 투과 음영 및 이동 소견은 관찰되지 않았으며, 대퇴 스 템의 침강이나 pedestal 형성은 관찰할 수 없었다. 1예에서 추시 48개월째에 대퇴 스템이 5 mm 이상의 수직 침강 소견을 보이고 저음영선이 대 퇴 스템 주위에 전반적으로 관찰되어 재치환술을 시행하였다. 1예에서 수술 후 대퇴 신경 마비 증상을 보였으나 추시 6개월째에 완전 회복되었다.
결 론 :Crowe 분류 IV 선천성 고관절 탈구 환자에서 영구적인 신경 마비 없이 하지 부동을 교정함에 있어서 이 수술 기법이 유용함을 알 수 있 었다.
색인 단어 : 선천성 고관절 탈구, 무시멘트 고관절 전치환술, 전자하 단축 절골술
Crowe Ⅳ 발달성 고관절 이형성증 환자에서
전자하 단축 절골술과 동반하여 시행한 무시멘트 고관절 전치환술
문경호∙이동주∙차승도∙박영하
인하대학교 의과대학 정형외과학교실