Perinatology Vol. 32, No. 2, June, 2021 https://doi.org/10.14734/PN.2021.32.2.100
Case report
Perinatology
pISSN 2508-4887•eISSN 2508-4895
Hannah Cho, MD1, Ju Sun Heo, MD1, Ki Hoon Ahn, MD, PhD2, Soon-Cheol Hong, MD, PhD2
1Department of Pediatrics,
2Department of Obstetrics &
Gynecology, Korea University Anam Hospital, Korea University College of Medicine, Seoul, Korea
Trisomy 9 mosaicism is a rare chromosomal abnormality with distinct and recognizable clinical features. In this report, we present an extremely low birth weight (ELBW) infant with trisomy 9 mosaicism. A male preterm infant born at 31+3 weeks of gestation, weighing 922 g, was delivered by cesarean section. Prenatal findings revealed severe intrauterine growth restriction and oligohydramnios. The result of non-invasive prenatal test was a low risk for chromosomal anomalies including trisomy 9. After birth, dysmorphic features were present, such as microcephaly, palpebral fissure, low set ears, a bulbous nose, micrognathia, and a high-arched palate. He also had a single umbilical artery, bilateral inguinal hernia, and cryptorchidism. Intra-organ evaluation revealed ventriculomegaly, mesocardia, absent right brachiocephalic trunk with double superior vena cava, and bilateral renal hypoplasia. He needed the respiratory support of a humidified high-flow nasal cannula until 4 months of corrected age. He had feeding difficulties requiring tube feeding because of poor oral sucking. The result of a postnatal chromosome study confirmed trisomy 9 mosaicism. To the best of our knowledge, this is the first case of an ELBW infant with trisomy 9 mosaicism in South Korea.
Key Words: Chromosome 9, trisomy mosaic; Infant, Extremely low birth weight; Congenital abnormalities
Introduction
Trisomy 9 is an uncommon chromosome disorder with high neonatal mortality and is seen more generally in cases of mosaicism.1-3 Since the first case report of trisomy 9 mosaicism by Haslam in 1973,4 more than 200 cases have been described in the literature.
As more surviving cases have been reported, the characteristic phenotypes and medical conditions in this unique group have been described in detail. Jones et al. reported on these clinical features: intrauterine growth restriction (IUGR), craniofacial abnormalities, skeletal abnormalities, congenital heart defects, and renal or genital abnormalities.5 Recently, Bruns and Campbell6 reported on the developmental delay of this population. However, there are few cases of preterm or extremely low birth weight (ELBW) infants diagnosed with trisomy 9 mosaicism. In this report, we present an ELBW infant diagnosed with trisomy 9 mosaicism.
Case
A 41-year-old mother (para 1) was transferred to our hospital at 30+4 weeks of gestation due to IUGR. There were no underlying diseases except for gestational diabetes mellitus.
Prenatal nuchal translucency and alpha-fetoprotein levels were normal. Non-invasive prenatal test (NIPT) results, including trisomy 9, indicated that the mother was in the low-risk group. In our hospital, prenatal ultrasonographic findings revealed severe IUGR, Received: 13 January 2021
Revised: 16 February 2021 Accepted: 3 March 2021 Correspondence to Ju Sun Heo, MD
Department of Pediatrics, Korea University Anam Hospital, 73 Goryeodae-ro, Seongbuk-gu, Seoul 02841, Korea
Tel: +82-2-920-6281 Fax: +82-2-922-7476 E-mail: [email protected] Co-correspondence to Ki Hoon Ahn, MD, PhD Department of Obstetrics &
Gynecology, Korea University Anam Hospital, 73 Goryeodae-ro, Seongbuk-gu, Seoul 02841, Korea Tel: +82-2-920-6777
Fax: +82-2-921-5357 E-mail: [email protected] Copyright© 2021 by The Korean Society of Perinatology
This is an Open Access article distributed under the terms of the Creative Com- mons Attribution Non-Commercial License (http://creativecommons.org/
license/by-nc/4.0/), which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided that the original work is properly cited.
Trisomy 9 Mosaicism in an Extremely Low
Birth Weight Infant
2021 June;32(2):100-103
www.e-kjp.org
https://doi.org/10.14734/PN.2021.32.2.100101
Perinatology
oligohydramnios, and heart anomalies such as dextrocardia, pulmonary regurgitation, and left ventricular outflow tract stenosis. Chromosome analysis on amniotic fluid was done.
However, before the diagnosis was confirmed, the emergency cesarean section was performed because of fetal distress and severe IUGR. After delivery, the result of chromosome study reported as trisomy 9 mosaicism.
A male preterm infant was born at 31+3 weeks of gestation.
Birth weight was 922 g (2nd percentile), length was 34 cm (<1st percentile), and head circumference was 24.5 cm (<1st percentile). Apgar scores were 3, 6, and 7 at 1, 5, and 10 minutes, respectively. He had dysmorphic features such as microcephaly, short and upwardly slanting palpebral fissure, low
set ears, a bulbous nose, micrognathia, high arched palate, right torticollis, and a single palmar crease (Fig. 1). He also had a single umbilical artery, bilateral inguinal hernia, and cryptorchidism.
Ventriculomegaly was found on brain sonography. Mesocardia and absent right brachiocephalic trunk with double superior vena cava were confirmed by echocardiography. Bilateral renal hypoplasia was observed on kidney sonography. Trisomy 9 mosaicism, primarily diagnosed by amniocentesis, was confirmed using chromosome analysis of the baby’s peripheral blood; a mosaic complement with trisomy 9 in 9% of cells and a normal male complement in 91% of cells (Fig. 2).
The patient had been hospitalized for a long time in the neonatal intensive care unit. He did not need a tracheal intubation, but needed the prolonged respiratory support of a humidified high- flow nasal cannula until 4 months of corrected age (CA). There were severe inspiratory stridor and suprasternal retraction, especially during oral feeding. Glossoptosis, and retroverted epiglottis were found during suspension laryngoscopy. There were no abnormalities in the trachea or subglottic area. He continued tube feeding because of poor oral sucking power and inappropriate sucking reflex. Bilateral sensorineural hearing loss (SNHL) was also diagnosed by auditory steady- state responses and he started to wear hearing aids. He was discharged at 5 months CA. He needed oxygen support by the nasal prong and tube feeding at that time. Recently, his age was 10 months CA. He doesn’t need any respiratory support but he still needs tube feeding. He could not lift or rotate his head in a prone position, roll over, or sit with support.
Fig. 1. Clinical photo of our patient. Typical dysmorphic face, short and upwardly slanting palpebral fissure, low set ears, a bulbous nose, and micrognathia.
A B
Fig. 2. Chromosome analysis shows both of the mosaic karyotypes, (A) 47XY, +9 in 9% of cells and (B) 46XY in 91% of cells.
Cho H, et al. ELBW infant with Trisomy 9 mosaicism
102
https://doi.org/10.14734/PN.2021.32.2.100www.e-kjp.org
Perinatology
Bruns and Campbell6 reported 25 cases of trisomy 9 mosai- cism and added several characteristics such as craniosynostosis and hemihyperplasia. The results of their study included medical conditions such as feeding or respiratory difficulties and delayed developmental status. They revealed that this group experienced feeding difficulties with most not requiring tube feeding at the time of survey completion, fewer children were affected by respiratory difficulties, including apnea and laryngomalacia. These were not consistent with our case because most of the cases (21/25) included in Bruns and Campbell’6s study were term or late preterm infants, and only one case was a very preterm infant (28 weeks of gestation) with a birth weight of 770 g. There are few reports of preterm infants with trisomy 9 mosaicism, and cases of ELBW infants are very rare.9 The female ELBW infant reported by Bruns and Campbell6 did not have any cardiac anomaly or renal problems. She needed supplemental oxygen for respiratory support. Enteral feeding used a gastric tube at birth, but full oral feeding was achieved
Discussion
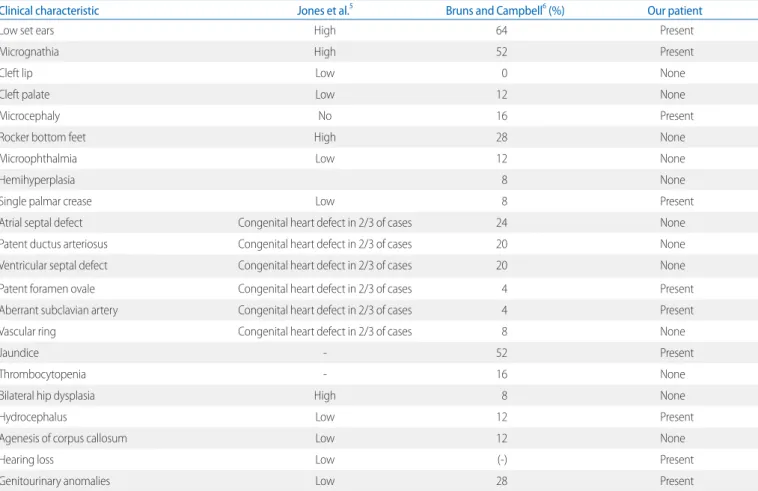
Trisomy 9 mosaicism is an uncommon chromosomal anomaly that carries a high possibility of spontaneous abortion and perinatal mortality.3 The clinical feature variability in trisomy 9 mosaicism depends on the varying degree of mosaicism or the different tissues involved.7,8 Several characteristic features of this chromosomal abnormality have been described in previous reports. Jones et al.5 summarized the typical characteristics of trisomy 9 mosaicism. The most common feature is IUGR during the perinatal period. The patient in our study had typical facial characteristics such as microcephaly, short and upwardly slanting palpebral fissure, low set ears, a bulbous nose, micro- gnathia, and a high-arched palate. Other typical features such as a single palmar crease, bilateral inguinal hernia, and cryptorchidism were also observed. Ventriculomegaly, heart problems, and hearing loss were also found in our case (Table 1).
Table 1. Clinical Characteristics of Our Patient Compared with Trisomy 9 Mosaicism Cases Reported by Jones et al.5 and Bruns and Campbell6
Clinical characteristic Jones et al.5 Bruns and Campbell6 (%) Our patient
Low set ears High 64 Present
Micrognathia High 52 Present
Cleft lip Low 0 None
Cleft palate Low 12 None
Microcephaly No 16 Present
Rocker bottom feet High 28 None
Microophthalmia Low 12 None
Hemihyperplasia 8 None
Single palmar crease Low 8 Present
Atrial septal defect Congenital heart defect in 2/3 of cases 24 None
Patent ductus arteriosus Congenital heart defect in 2/3 of cases 20 None
Ventricular septal defect Congenital heart defect in 2/3 of cases 20 None
Patent foramen ovale Congenital heart defect in 2/3 of cases 4 Present
Aberrant subclavian artery Congenital heart defect in 2/3 of cases 4 Present
Vascular ring Congenital heart defect in 2/3 of cases 8 None
Jaundice - 52 Present
Thrombocytopenia - 16 None
Bilateral hip dysplasia High 8 None
Hydrocephalus Low 12 Present
Agenesis of corpus callosum Low 12 None
Hearing loss Low (-) Present
Genitourinary anomalies Low 28 Present
2021 June;32(2):100-103
www.e-kjp.org
https://doi.org/10.14734/PN.2021.32.2.100103
Perinatology
Ethics statement
This case report is published with the consent of his parents.
References
1) Bowen P, Ying KL, Chung GS. Trisomy 9 mosaicism in a newborn infant with multiple malformations. J Pediatr 1974;85:95-7.
2) Levy I, Levy Y, Mammon Z, Nitzan M, Steinherz R. Gastrointestinal abnormalities in the syndrome of mosaic trisomy 9. J Med Genet 1989;
26:280-1.
3) Stoll C, Chognot D, Halb A, Luckel JC. Trisomy 9 mosaicism in two girls with multiple congenital malformations and mental retardation. J Med Genet 1993;30:433-5.
4) Haslam RH, Broske SP, Moore CM, Thomas GH, Neill CA. Trisomy 9 mosaicism with multiple congenital anomalies. J Med Genet 1973;10:
180-4.
5) Jones KL, Jones MC, Del Campo M. Smith's recognizable patterns of human malformation. 7th ed. Philadelphia (PA): Saunders; 2013.
6) Bruns DA, Campbell E. Twenty-five additional cases of trisomy 9 mosaic:
birth information, medical conditions, and developmental status. Am J Med Genet A 2015;167A:997-1007.
7) Zen PR, Rosa RF, Rosa RC, Graziadio C, Paskulin GA. New report of two patients with mosaic trisomy 9 presenting unusual features and longer survival. Sao Paulo Med J 2011;129:428-32.
8) Bruns D. Presenting physical characteristics, medical conditions, and developmental status of long-term survivors with trisomy 9 mosaicism.
Am J Med Genet A 2011;155A:1033-9.
9) Okumura A, Hayakawa F, Kato T, Kuno K, Watanabe K. Two patients with trisomy 9 mosaicism. Pediatr Int 2000;42:89-91.
10) Bianchi DW, Chiu RWK. Sequencing of circulating cell-free DNA during pregnancy. N Engl J Med 2018;379:464-73.
11) Taylor-Phillips S, Freeman K, Geppert J, Agbebiyi A, Uthman OA, Madan J, et al. Accuracy of non-invasive prenatal testing using cell-free DNA for detection of Down, Edwards and Patau syndromes: a systematic review and meta-analysis. BMJ Open 2016;6:e010002.
12) Gil MM, Quezada MS, Revello R, Akolekar R, Nicolaides KH. Analysis of cell-free DNA in maternal blood in screening for fetal aneuploidies:
updated meta-analysis. Ultrasound Obstet Gynecol 2015;45:249-66.
13) Mackie FL, Hemming K, Allen S, Morris RK, Kilby MD. The accuracy of cell-free fetal DNA-based non-invasive prenatal testing in singleton pregnancies: a systematic review and bivariate meta-analysis. BJOG 2017;124:32-46.
at the time of the survey. In that case, trisomy 9 was present in 6% of cells. She showed milder symptoms compared to our case. This could be related to the lower proportion of cells with trisomy 9 and the lower number of infiltrated organs in the case of literature. Unlike this case, our case had multi- organ abnormalities, such as ventriculomegaly, SNHL, cardiac anomalies, and renal hypoplasia. Feeding and respiratory diffi- culties were more severe. Developmental delay was also accompanied at 7 months CA, as Bruns and Campbell6 revealed in this unique group. This developmental delay in our case was not only due to mosaicism, but also to preterm birth. More survival data should be collected, including those of preterm or ELBW infants.
NIPT became clinically available and was recommended as a screening option for women at increased risk of fetal aneuploidy. However, it could report unreliable results for the following reasons: confined placental mosaicism (the detected placental cells of the mosaicism are euploid, but the fetus itself is aneuploid), low fetal fraction, copy number variants, and technical error.10-13 Therefore, if abnormal findings are observed on prenatal ultrasonography, even though NIPT is normal, prenatal counselling and amniocentesis are recommended.
The strength of this report is that the current case is the first case of an ELBW infant with trisomy 9 mosaicism in South Korea. This case provides important information about the clinical characteristics at birth and short-term developmental outcomes of rare ELBW infants with trisomy 9 mosaicism.
In conclusion, trisomy 9 mosaicism is a rare chromosomal abnormality with various clinical features. ELBW infants with trisomy 9 mosaicism also show typical characteristics at birth.
Therefore, early suspicion and diagnosis could be possible.
Long-term follow-up is important for preterm infants with trisomy 9 mosaicism because of poor prognosis in feeding, respiration, and development.
Conflict of interest
No potential conflict of interest relevant to this article was reported.