1서울대학교 의과대학 분당서울대학교병원 신경외과학교실, 2Faculty of Medicine Universitas Indonesia, Jakarta, Indonesia,
3서울대학교 의과대학 분당서울대학교병원 이비인후과학교실
권지연
1, Nurani Rahma Arafah
2, 조성우
3, 황기환
11Department of Neurosurgery, Seoul National University Bundang Hospital, Seoul National University College of Medicine, Seoul, Korea
2Faculty of Medicine Universitas Indonesia, Jakarta, Indonesia
3Department of Otorhinolaryngology-Head and Neck Surgery, Seoul National University Bundang Hospital, Seoul National University College of Medicine, Seoul, Korea
Ji-Eyon Kwon
1, Nurani Rahma Arafah
2, Sung-Woo Cho
3, Kihwan Hwang
1추체첨부에 생긴 지주막낭에 의해 유발된 희귀 삼차 신경통:
증례보고
J Korean Skull Base Society 15권 2호 : 141~146, 2020
종설1 원저1 원저2
증례1 원저3
증례2 증례3 증례4
증례7 증례5
증례8 증례6
증례9
Vascular compression is the most common cause of classic trigeminal neuralgia. However, other causes should be excluded. We describe a rare case of a patient presenting with typical trigeminal neuralgia associated with an arachnoid cyst in the petrous apex. A 22-year-old female patient with right trigeminal neuralgia for several years was treated with carbamazepine, which relieved the pain temporarily but was completely ineffective for the 3 months prior to presentation. Thin-slice computed tomography and magnetic resonance imaging showed a cephalocele in the petrous apex. Eventually, surgical aspiration of the cyst was performed using an endoscopic endonasal approach, which resulted in complete resolution of her pain.
Petrous apex cephalocele should be considered in the differential diagnosis of trigeminal neuralgia, as it can be easily resolved by surgical aspiration.
Rare cause of trigeminal neuralgia associated with an arachnoid cyst in petrous apex: Case report
논문 접수일 : 2020년 8월 22일 논문 완료일 : 2020년 10월 2일
주소 : Department of Neurosurgery, Seoul National University Bundang Hospital, 82 Gumi-ro 173beon-gil, Bundang-gu, Seongnam 13620, Korea
Tel : +82-31-787-7169 Fax : +82-31-787-4097 E-mail : [email protected]
교신저자
Trigeminal neuralgia, Endoscopy endonasal surgery, Arachnoid cysts, Petrous apex, Cephalocele
Key Words
Kihwan Hwang
▒ INTRODUCTION
The most common cause of classic trigeminal neuralgia is vascular compression. However, other causes, such as space-occupying lesions arising from direct compression of the trigeminal nerve within the Meckel’s cave or petrous apex, should be excluded. The medial part of the temporal bone is called the petrous apex, which is in the shape of a trimmed pyramid. Petrous apex cephalocele (PAC) is an uncommon lesion in the petrous apex, related to either a congenital or acquired herniation from the posterolateral portion of the Meckel’s cave and varies from the meningocele to the arachnoid cyst.[1] PACs are usually asymptomatic; however, they might cause painful
trigeminal neuropathy on rare occasions. Anticonvulsive medication is the first treatment of choice for trigeminal neuralgia. Surgery could be an effective choice for those who become unresponsive to medication or for those who undergo severe side effects of medication. We describe a rare case of a patient presenting with typical trigeminal neuralgia associated with an arachnoid cyst in the petrous apex.
▒ CASE REPORT
1. Clinical presentation
A 22-year-old female patient was admitted to our neurosurgery clinic with a chief complaint of right facial
Fig. 1
A B
E
C
F D
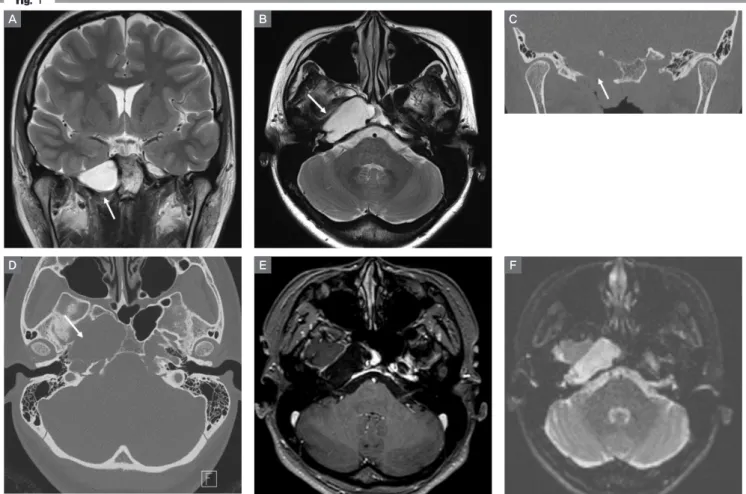
(A, B) Preoperative magnetic resonance imaging. In the T2-weighted image, a 3.5 × 1.8-cm expansile cystic lesion is found in the right foramen ovale (white arrows).
(C, D) Computed tomography scan also shows this lesion involving the right sphenoid sinus with a medial posterior relationship to the right paraclival internal carotid artery without effusion of mastoid air cell (white arrows). (E) Non-enhanced lesion with mainly cystic portion in T1-weighted image and (F) no restricted diffusion in diffusion-weighted image revealed that this lesion is more likely to be the petrous apex cephalocele than cystic schwannoma.
pain with increasing severity in the 3 months before admission. She had been experiencing pain on her entire face for the last 15 years without any specific history of trauma. The pain was provoked by external stimulation, such as chewing food or brushing teeth, would last for minutes to hours, and was relieved with the cessation of the stimulation or by medications. She experienced a severe shooting pain in the right cheek with a severity index of numeral rating scale (NRS) 8, followed by ache, discomfort, and tingling sensation. Later, it radiated to the right half of her face. At first, she was diagnosed with right trigeminal neuralgia. She had already received several treatments with carbamazepine and other oral analgesics. After pharmacological medication, her facial pain severity index reduced to NRS 5. In the last few months, she noted that carbamazepine only partially relieved her symptoms; however, bothersome right facial neuropathic pain was persistent.
Neurological examination was unremarkable, including facial expression and sensation, which were intact and symmetrical. Nevertheless, preoperative magnetic resonance imaging (MRI) revealed compression of the pathway of the right trigeminal nerve, the so-called Meckel’s cave, by a cystic mass in the petrous bone. The brain MRI revealed an expansive cystic lesion (3.5 × 1.8 cm) without avid enhancement in the right foramen ovale,
expanding to the right cavernous sinus and clivus, and spaying trigeminal nerve bundle (Fig. 1).
Following evaluation of the patient’s history, physical examination, and imaging work-up, the patient was found to have resistance to pharmacological therapy for trigeminal neuralgia suggestive of PAC. She was then admitted for an elective surgery using the procedure of cyst decompression via an endoscopic endonasal approach.
2. Operation
The patient underwent an image-guided endoscopic endonasal transpterygoid approach, which would maximize the exposure of the cephalocele in the far lateral recesses of the sphenoid sinus.[2] The procedure consisted of cyst decompression and fat grafting, followed by duroplasty and skull base reconstruction conducted by the combined cooperation of the neurosurgeon and otolaryngologist.
Fascia lata graft and autologous fat were harvested from the patient’s thigh to reconstruct the skull base defect. In order to repair the defects in the skull base successfully, meticulous multilayered reconstruction is crucial to repair the cerebrospinal fluid (CSF) leaks after the operation.[2]
The main procedure started on the right side, where the petrous apex was exposed and drilled by an otolaryngologist using a transpterygoid approach. After the dura was opened, an arachnoid-lined cyst was
Fig. 2
A B C
Intraoperative view.
(A) The arachnoid cyst (asterisk) is found to open and decompress. The fanned trigeminal nerve root (letter T) is identified. (B) Positioning of the autologous fat graft (letter F).
(C) A vascularized nasal septal flap (NSF) is covered.
identified using angled endoscopes, with the aid of image guidance. The cyst was punctured, and a CSF-like clear cystic fluid was expelled with high pressure. There was no brain parenchyma or mass-like lesion, and the surgeon concluded that the cyst was the most characteristic of a petrous apex arachnoid cyst (Fig. 2). Thinned trigeminal nerve was identified after fluid aspiration and bleeding control. Subsequently, we performed reconstruction of the skull base, fat tissue filling, and repair of the dura.
Finally, the prepared nasoseptal flap was applied, and hemostasis was performed meticulously.
3. Postoperative management
Postoperative MRI showed a grossly removed previous large cystic lesion (Fig. 3). The fat graft was filled in the right petrous apex lesion. We could not see any unusual postoperative findings at the paranasal sinuses or abnormal mass in the pituitary gland.
On postoperative day 1, the patient showed transient sixth cranial nerve (CN) palsy (diplopia) and complained of slight facial numbness, which resolved naturally 1 month after surgery. On MRIs taken 3 months later, the previous large cystic lesion in the right petrous apex was removed and obliterated with a fatty graft without a reduction in volume (Fig. 4). Despite these events, her neuralgia
Fig. 4
A B
Follow-up magnetic resonance imaging 3months after the operation.
(A, B) The lesion in the right petrous apex (white arrows) was still obliterated with fatty graft without the reduction of volume.
Fig. 3
A B
Postoperative magnetic resonanceimaging.
(A, B) T2-weighted image displaying a grossly removed previous large cystic lesion (white arrows) in the right petrous apex filled with fatty graft.
symptoms decreased with each passing day without specific supplements.
▒ DISCUSSION
We describe a rare case of a patient with an arachnoid cyst confined to the Meckel’s cave with trigeminal neuralgia. Irritation of the trigeminal nerve triggers intense, piercing, electric shock-like pain and branches to the forehead, cheek, and lower jaw. The main cause of pain is contact between an artery or vein and the trigeminal nerve at the base of the brain. This sets pressure on the nerve as it enters the brain and causes the nerve to misfire. Other causes of trigeminal neuralgia include pressure of a space-occupying lesion on the nerve.
We present the successful decompression of an arachnoid cyst in the petrous apex via the endoscopic endonasal transpterygoid approach. Surgical manipulation of the cystic mass via endoscopy may cause indirect stretching of the delicate abducent nerve (CN 6th) with resultant neuropraxia in this case. This complication is difficult to
identify and prevent intraoperatively as the nerve lies on the back side of the view of the operation field.
PAC is a rare lesion and has been inconsistently referred to as both a meningocele and an arachnoid cyst. It is difficult to distinguish between a meningocele and an arachnoid cyst by determining the presence of a dural lining on MRIs.[3] The term PAC is more inclusive as the lesion is either a congenital or acquired herniation of the posterolateral Meckel’s cave margin and contents of the petrous apex, and the term meningocele or arachnoid cyst could be most applicable depending on the surgeon’s findings on the lesion walls.[1] On the contrary, other findings such as inflammation or neoplasms should also be differentiated. For the differential diagnosis of imaging findings, PAC is usually located outside the petrous apex (posterior portion of the Meckel’s cave); however, inflammatory lesions are found inside the petrous apex.
Moreover, the diffusion-weighted imaging sequence might help distinguish a PAC from an inflammatory lesion.[4] If it is accompanied by CSF otorrhea, mastoid or middle ear effusion should be considered for an unusual type of PAC.[1]
Table 1. Cases of patients who underwent trigeminal neuralgia associated with the petrous apex cephalocele in the literatures
Case
No.
Age (yr)
/Sex Clinical presentation Side Surgical
diagnosis Treatment Approach Treatment outcome Reference
1 25/F Ipsilateral TN and CNVI palsy, headache Left Meningocele Surgery Infratemporal postauricular Craniotomy
Improved CN VI palsy and remained CN V symptoms [1]
2 48/F Ipsilateral TN and CN
III palsy Left Meningocele Surgery N/A N/A
3 64/F Ipsilateral TN Left Meningocele Surgery Endoscopic endonasal
approach Symptom resolved [3]
4 55/F
Ipsilateral TN with lower facial paresthesia
Right Arachnoid cyst Surgery
Subtemporal intradural approach via lateral temporal craniotomy
Symptom resolved [6]
5 44/M
Ipsilateral TN, dysaesthesia, vertigo and diplopia
Right Arachnoid cyst Surgery
Lateral suboccipital retrosigmoid approach (cyst was spread out into cerebellopontine angle)
Symptom resolved [7]
6 57/F Ipsilateral TN Left Arachnoid cyst Cyst drain Percutaneous needle
aspiration Symptom resolved [5]
7 42/F Ipsilateral TN Left Arachnoid cyst Medication N/A N/A [8]
8 22/F Ipsilateral TN Right Arachnoid cyst Surgery Endoscopic endonasal
approach Symptom resolved Present
case F: female, M: male, TN: trigeminal neuralgia, CN: cranial nerve, N/A: not applicable.
Lesions of the petrous apex can influence the adjacent anatomical structures, such as the internal carotid artery, trigeminal ganglion, abducens nerve, jugular bulb, and petrosal sinuses. Therefore, these lesions can present with various clinical signs and symptoms, depending on the characteristics of the pathological procedure, size, and location. Trigeminal neuralgia classically has been related to neurovascular compression in the prepontine cistern at the nerve root entry-zone or in Meckel’s cave due to an abnormal vessel, tumor, cyst, and so on. However, the arachnoid cyst in the petrous apex may cause compression of the trigeminal ganglion; therefore, the patient in this case suffered from trigeminal neuralgia. Only a few cases of PACs with trigeminal symptoms have been reported in the literature (Table 1).[1,3,5-8]
The petrous apex is located deep within the skull base and can be challenging to access with traditional microsurgical approaches. However, it can be accessed easily via an endoscopic endonasal approach, depending on the site of the lesion and the degree of pneumatization of the petrous apex and sphenoid sinus.[2,9-11] There are several advantages in using the endoscopic approach:
reduced risk to the facial nerve and vestibulo-cochlear function (compared with middle and lateral fossa approaches), reduced operative time and hospital stay, and ease of nasendoscopic examination of the postoperative site in the outpatient department.[9] In addition, Bigder et al. [5] suggested aspiration of the arachnoid cyst via the foramen ovale using a percutaneous needle. They developed a technique of percutaneous glycerol rhizotomy without injecting glycerol or other agents, which resulted in the successful relief of a patient’s painful trigeminal neuropathy.
In conclusion, PAC should be considered in the differential diagnosis of trigeminal neuralgia, which might
be easily resolved by surgical aspiration.
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
REFERENCES
1. Moore KR, Fischbein NJ, Harnsberger HR, Shelton C, Glastonbury CM, White DK, et al. Petrous apex cephaloceles. AJNR Am J Neuroradiol 2001;22:1867- 71.
2. Schmidt RF, Choudhry OJ, Raviv J, Baredes S, Casiano RR, Eloy JA, et al.
Surgical nuances for the endoscopic endonasal transpterygoid approach to lateral sphenoid sinus encephaloceles. Neurosurg Focus 2012;32:E5.
3. Alobaid A, Schaeffer T, Virojanapa J, Dehdashti AR. Rare cause of trigeminal neuralgia: Meckel's cave meningocele. Acta Neurochir (Wien) 2015;157:1183-6.
4. Fistouris P, Winkelmann D, Wessling J, Schick U. Meningocele of petrous apex: A case report, literature review of differential diagnosis and its radiological findings. J Neurol Clin Neurosci 2018;2:24-6.
5. Bigder MG, Helmi A, Kaufmann AM. Trigeminal neuropathy associated with an enlarging arachnoid cyst in Meckel's cave: Case report, management strategy and review of the literature. Acta Neurochir (Wien) 2017;159:2309-12.
6. Batra A, Tripathi RP, Singh AK, Tatke M. Petrous apex arachnoid cyst extending into Meckel's cave. Australas Radiol 2002;46:295-8.
7. Wörner BA, Noll M, Rahim T, Fink U, Oeckler R. Recurrent arachnoid cyst of Meckel's cave mimicking a brain stem ischaemia. Report of a rare case.
Zentralbl Neurochir 2003;64:76-9.
8. Fois P, Lauda L. Bilateral Meckel's cave arachnoid cysts with extension to the petrous apex in a patient with a vestibular schwannoma. Otol Neurotol 2011;32:e36-7.
9. Jaberoo MC, Hassan A, Pulido MA, Saleh HA. Endoscopic endonasal approaches to management of cholesterol granuloma of the petrous apex.
Skull Base 2010;20:375-9.
10 Shin M, Kondo K, Hanakita S, Hasegawa H, Yoshino M, Teranishi Y, et al.
Endoscopic transsphenoidal anterior petrosal approach for locally aggressive tumors involving the internal auditory canal, jugular fossa, and cavernous sinus. J Neurosurg 2017;126:212-21.
11. Zakaria J, Saini P, Yanovskaya M, Tsiang JT, Ravindran K, Johans S, et al.
Endoscopic endonasal resection of Meckel's cave epidermoid cysts: Case discussion and literature review. Case Rep Neurol Med 2020;2020:7853279.