Address reprint requests to Dae Yul Kim, MD, PhD.
Department of Rehabilitation Medicine, Asan Medical Center, University of Ulsan College of Medicine 88, Olympic-ro 43-gil, Songpa-gu, Seoul 138-736, Korea
TEL: 82-2-3010-3793, FAX: 82-2-3010-6964, E-mail: [email protected] 투고일: 2013년 9월 11일, 수정일: 2013년 11월 19일, 게재확정일: 2013년 11월 19일
INTRODUCTION
Distal symmetrical sensorimotor polyneuropathy is the
most common form of diabetic peripheral polyneuropa- thy (DM PPN).
1Electrodiagnostic study is an objective and quantifiable tool for the diagnosis of DM PPN, and
무증상의 당뇨병성 신경병증을 배제에 필요한 최소한의 전기진단 검사의 적용
울산대학교 의과대학 서울아산병원 재활의학과
김대열∙문혜진∙양서연
– Abstract –
Applicability of a Simplified, Electrodiagnositic Study for Exclusion of Subclinical Diabetic Polyneuropathy
Dae Yul Kim, MD, PhD, Hye Jin Moon, MD, Seoyeon Yang, MD.
Department of Rehabilitation Medicine,
Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
목목적적:: 본 연구의 목적은 무증상 당뇨병성 말초신경병증을 배제하는데 있어서 당뇨병 환자의 전기진단 학적 검사를 최소화하는 방법을 찾는 것이다.
방
방법법:: 본 전기진단 검사실에 의뢰된 975명의 제 2형 당뇨병 환자들을 연구 대상으로 하였다. 신경전 도검사에서 아래의 4개 항목으로 총 15가지의 검사 종류의 조합을 만들었다. 즉 비골 운동신경전도검 사, 비골 F 검사, 경골 운동신경전도검사와 F 검사 4가지 종류로 조합을 정하였다. 모든 조합에서 비 복 감각신경전도검사는 반드시 포함되었다. 그래서 각 조합 방법에 따른 특이도, 음성 예측값 및 비정 상 수치 빈도를 계산하였다.
결
결과과:: 연구기준에 포함된 무증상의 528명 환자 중에서 96명이 무증상 당뇨병성 말초신경병증으로 진 단되었다. 최소화한 신경전도검사 조합들 중에서 비복신경 감각신경전도검사, 비골 운동신경전도검사, 비골 F 검사 및 경골 F 검사의 조합이 가장 높은 음성 예측값(94.3%)을 보였으며 다른 조합들에 비 해 의미 있게 비정상 수치 빈도를 보였다.
결
결론론:: 무증상의 당뇨병 환자에서 당뇨병성 말초신경병증을 배제하는 데 있어서 상기 최소화된 신경전 도검사 조합은 시간 및 비용을 절약하고, 신경전도검사를 통한 환자의 고통을 최소화할 수 있을 것으 로 판단된다.
Key Words:
당뇨병성 신경병증, 전기진단, 신경전도검사, 다발신경병증which can diagnose the subclinical stage of DM PPN.
2Currently, nerve conduction study (NCS) is commonly being used as the standard test for diagnosis of DM PPN in diabetic patients. There are many previous recommen- dations regarding the NCS criteria for the diagnosis of DM PPN, although no formal consensus exists. Some authors have recommended that study subjects with more than two abnormal measures in the upper and lower limbs, as seen on NCS, should be regarded as hav- ing DM PPN.
3-5This definition may not reflect the true pathogenesis of distal symmetrical polyneuropathy, which first affects the longest nerve. And if we use the above criteria for diagnosing DM PPN, we must exam- ine all possible nerves in order to find an abnormal nerve. One study suggested that distal latencies or con- duction velocities (CV) of the sural sensory nerve action potential (SNAP) and tibial compound muscle action potentials (CMAP) should be regarded as the gold stan- dard for the diagnosis of DM PPN.
6And one author indi- cated that the definition of DM PPN suggested an abnor- mal sural SNAP, (distal latency and/or amplitude) and peroneal CMAP (amplitude and/or F-wave) response.
7The American Association of Electrodiagnostic Medi- cine (AAEM) recommended that the minimum definition criterion is an abnormality of any two, separate nerve conduction, one of which must be the sural nerve.
8Many patients suffer from multiple, electrical stimula- tions during NCS. Recently, we have attempted to find a more sensitive and an additional nerve study for diagnos- ing DM PPN in diabetic patients.
9However, there is no formal consensus on the NCS protocol which is sensitive and specific enough to rule out PPN in asymptomatic dia- betic patients. One author suggested that complete electro- diagnostic tests for diagnosing DM PPN have not always been used due to a lack of patient compliance, their time- consuming aspect, and their lack of cost effectiveness.
10Therefore, definition of DM PPN has been based upon patients’ neuropathic symptoms or signs. In this respect, it doesn’t seem necessary for us to do more additional nerve study for diagnosing subclinical stage of DM PPN.
The purpose of our study is to define a simplified elec- trodiagnostic protocol for diabetic patients without neu- ropathic symptoms. We expect that we may rule out patients without DM PPN using a simplified NCS.
MATERIALS AND METHODS
Nine hundred and seventy five patients with type II
diabetes mellitus who were referred to our electromyo- graphic laboratory were prospectively enrolled in our study. These patients were referred to our laboratory for a screening test for DM PPN or due to their neuropathic symptoms. All patients underwent a detailed neurologic examination including muscle power, muscle tone, pin- prick test, and a vibratory and light touch sensation test of both the upper and lower extremities. We checked for neuropathic symptoms including pain, a tingling sense, paresthesia and/or subjective sensory change throughout the interview.
Patients were excluded if they had other combined neuropathy confirmed by electrodiagnostic study, and including carpal tunnel syndrome, mono-neuropathy or radiculopathy. We also excluded patients with an abnor- mality seen on any neurologic examination, symptoms or sign of neuropathy, and concomitant diseases which could affect peripheral nerve function, and including malnutrition or alcoholic hepatitis. We also excluded patients who had undergone a peroneal NCS which recorded at tibialis anterior muscle because of atrophy of the extensor digitorum brevis (EDB) muscle.
NCS was measured using a 4-channel, electro-physio- logical machine (Medelec
�by Company of Oxford, United Kingdom) and a surface electrode. The skin sur- face temperature was equalized and maintained at 32~34
℃ during NCS. Abnormal NCS measures were defined
as those with amplitudes lower than, and slowed nerve conduction relative to standard values of our electrodiag- nostic laboratory. Abnormal peroneal CMAP was defined if it had any of the following; onset latency above 6.2 ms, peak to peak amplitude below 2 mV or CV below 50m/s. Abnormal tibial CMAP was defined if it had any of the following: onset latency above 5 ms, peak to peak amplitude below 5 mV or CV below 40m/s.
And we defined abnormal sural SNAP if peak latency was above 3.9 ms or onset to peak amplitude was below 10㎶.
Motor NCSs were measured from the median (record- ed at the abductor pollicis brevis), ulnar (recorded at the abductor digiti minimi), peroneal (recorded at the EDB) and tibial (recorded at the abductor hallucis) nerves.
Antidromic sensory NCSs were measured from the
median, ulnar and sural nerves. These nerves were stim-
ulated at fixed point. The motor nerves were stimulated
10 cm away from the active electrode and the sensory
nerves were stimulated 14 cm away from the active elec-
trode. Minimal F-responses were measured from the
median, ulnar, peroneal and tibial nerves. These NCSs were performed primarily on the right side of the body, however, the left side was used if a local nerve lesion was suspected based on the patient’s history and the clin- ician’s judgments, or if the NCS had an abnormal value on the right side of the body. For the F response, 10 stimuli were given at a frequency of 1/s. An F-response was defined as an action potential of an amplitude exceeding 20㎶ and a latency within a reasonable range for the investigated nerve, and excluding spurious volun- tary activity. The latency to the onset of the first deflec- tion from the baseline was recorded for each stimulus, and the shortest latency was determined for the minimal F-response. Abnormal values were defined as a minimal F-response of ≥50 m/s in peroneal and tibial nerves.
The electrodiagnostic criteria for distal symmetric polyneuropathy are abnormalities of at least 3 parame- ters of nerve conduction study (distal latency, amplitude, conduction velocity, and minimal F response) in two separate nerves, one of which must be the sural nerve.
We devised a total 15 NCS protocols using four NCS parameters, i.e; peroneal CMAP, peroneal F-response, tibial CMAP and tibial F-response. Each NCS protocol was composed of combinations of 1~4 NCS parameters from among the above, four NCS parameters. Therefore, we made 15 protocols as follows: peroneal CMAP, tibial CMAP, peroneal F response, tibial F response, peroneal CMAP + tibial CMAP, peroneal CMAP + tibial F response, peroneal CMAP + peroneal F response, tibial CMAP + tibial F response, tibial CMAP + peroneal F response, tibial F response + peroneal F response, tibial CMAP + tibial F response + peroneal F response, per- oneal CMAP + tibial F response + peroneal F response, peroneal CMAP + tibial CMAP + tibial F response, per- oneal CMAP + tibial CMAP + peroneal F response, and peroneal CMAP + tibial CMAP + peroneal F response + tibial F response. Sural SNAP was included in all of these protocols.
We compared the sensitivity, specificities, and nega- tive predictive value among the 15 NCS protocols. Neg- ative predictive value was defined as the proportion of the study subjects without DM PPM among those who have normal values in all NCS parameters affiliated with each NCS protocol. We also calculated the frequency of abnormal value which was defined that the percentage of the subjects with an abnormal value in any of the NCS parameters within the NCS protocol among the total 528 subjects without neuropathic symptoms. The NCS protocol
with a high frequency of an abnormal value, was very important because we also commonly used the criteria of DM PPN recommended by Dick et al.
3-5Sensitivity =
Number of subjects who have abnormal value in any NCS parameters within NCS protocol Number of the subjects with DM PPN
Specificity =
Number of the subjects who have normal value in all NCS parameters within NCS protocol Number of the patients without DM PPN
Negative predictive value =
Number of the subjects without DM PPN
Number of the subjects who have normal value in all NCS parameters within NCS protocol
Frequency of abnormal value =
Number of the subjects who have abnormal value in any NCS parameters within NCS protocol Number of the subjects without neuropathic symptom (n=528)
Demographic and laboratory data, including age, dura- tion of diabetes, body mass index, and hemoglobin A1C (Hb A1C) titer, were recorded.
STATISTICAL METHODS
The differences in the general characteristics of diabetic patients with and without DM PPN were analyzed using the Chi-square and Student t-tests. McNemar’s test was used to compare the sensitivity, specificity and frequency of abnormal values among the 15 NCS protocols. Statisti- cal significance was defined as a p value of <0.05. All statistical analysis was performed using SPSS version 18.
RESULTS
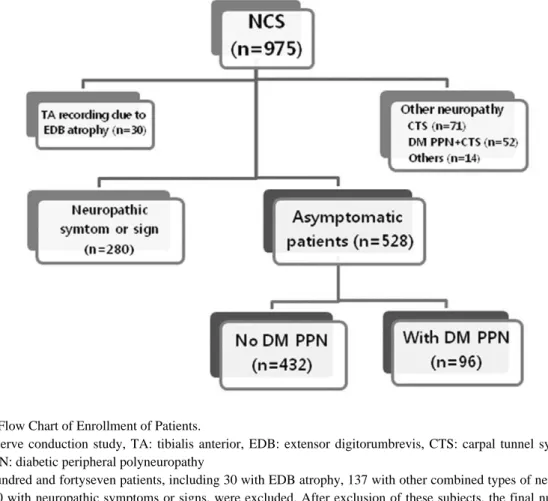
Figure 1 shows the patient enrollment in flow chart.
The total of patients who were enrolled in our study were 528.
Table 1 shows the comparisons of the subjects demo- graphic and laboratory data in patients without DM PPN (274 males and 158 females) and with DM PPN (61 males and 35 females). The patients with DM PPN had a longer duration of diabetes mellitus than those without DM PPN (135.4 ± 92.6 vs.75.5 ± 69.1 months, p<0.05). No other variables were significantly different between the two groups.
Table 2 shows the specificity and sensitivity of each
NCS protocol. Because we wanted to rule out the
patients without DM PPN among the asymptomatic
patients using a simplified NCS protocol, if possible, an
NCS protocol with high specificity was important. The
NCS protocols with a high specificity were the tibial
CMAP (98.8 %), peroneal CMAP (97.7%), and peroneal
CMAP + tibial CMAP (96.5%), however, these proto-
cols have low sensitivity and a high false negative rate.
Therefore we could not consider the specificity of each of these NCS protocols only.
Table 3 shows the negative predictive values of the NCS protocols. However, if we examine more NCS parameters, the negative predictive value is increased.
Therefore, an NCS protocol with four NCS parameters (Protocol E; peroneal CMAP + tibial CMAP + peroneal F + tibial F) would have the highest negative predictive value (94.7%). Among the four protocols consisting of
three NCS parameters, two protocols marked with A (tibial CMAP + tibial F + peroneal F) and B (peroneal + tibial F + peroneal F) had high negative predictive values (94.3% and 94.3%) compared with the other two proto- cols (protocol C; peroneal CMAP + tibial CMAP + tibial F and protocol D; peroneal CMAP + tibial CMAP + per- oneal F) .
Table 4 indicates the frequency of an abnormal value in the 15 NCS protocols. The frequency of an abnormal value was defined as the percentage of patients with an
Table 1. Comparison of Demographic and Laboratory Data between Subjects with and without DM PPNNo DM PPN (n=432) DM PPN (n=96)
Male: Female (n) 274:158 61:35
Age (years) 56.0 ±29.6 59.7 ± 11.0
Duration of diabetes (months) 75.5 ± 69.1 135.4 ± 92.6*
Hb A1C (%) 27.1 ±20.7 27.5 ±20.9
BMI (Kg/m2) 28.0 ±25.2 29.0 ±26.3
Values are mean ± standard deviation, *p<0.05
DM PPN: diabetic peripheral polyneuropathy, Hb A1C: hemoglobin A1C, BMI: body mass index Fig. 1. Flow Chart of Enrollment of Patients.
NCS: nerve conduction study, TA: tibialis anterior, EDB: extensor digitorumbrevis, CTS: carpal tunnel syndrome, DM PPN: diabetic peripheral polyneuropathy
Four hundred and fortyseven patients, including 30 with EDB atrophy, 137 with other combined types of neuropathy and 280 with neuropathic symptoms or signs, were excluded. After exclusion of these subjects, the final number of eligible patients for this study was 528. Of these 528, asymptomatic diabetic patients, 96 were diagnosed with DM PPN by NCS.
abnormal value in any one of NCS parameters in each NCS protocol. Protocol E has the highest frequency of abnormal values (34.0%) among the 15 NCS protocols.
Protocols A and B have a significantly higher frequency of abnormal values than the other two protocols (proto- col C and D) with three NCS parameters or the 10 proto- cols with one or two NCS parameters (p<0.05). Protocol E has a significantly higher frequency of abnormal val-
ues (p<0.05) compared with protocol A. However, there was no significant difference between protocol B and E regarding the frequency of an abnormal value (p>0.05).
As we would like to simplify NCS in diabetic patients without neuropathic symptoms, we can recommend pro- tocol B rather than protocol E. We can rule out DM PPN if the patients do not have abnormal values in all NCS parameters within protocol B.
Table 2. Specificity and Sensitivity of the NCS Protocols
NCS protocols Specificity (%) Sensitivity (%)
Peroneal 97.7 40.0
Tibial 98.8 41.7
Tibial F 93.1 64.2
Peroneal F 85.4 65.8
Peroneal + Tibial 96.5 50.8
Peroneal + Tibial F 91.0 71.7
Peroneal + Peroneal F 83.8 73.3
Tibial + Tibial F 91.9 70.8
Tibial + Peroneal F 84.5 76.7
Tibial F + Peroneal F 81.9 77.5
Tibial + Tibial F + Peroneal F (= protocol A) 81.0 82.5
Peroneal + Tibial F + Peroneal F (= protocol B) 80.3 82.5
Peroneal + Tibial + Tibial F (= protocol C) 89.8 75.8
Peroneal + Tibial + Peroneal F (= protocol D) 82.9 80.8
Peroneal + Tibial + Peroneal F + Tibial F (= protocol E) 79.4 85.8
Values are mean ± standard deviation, *p<0.05,
NCS: nerve conduction study, Peroneal:peroneal compound muscle action potential (CMAP),
Tibial: tibial CMAP, Tibial F: minimal F-response of the tibial nerve, Peroneal F: minimal F-response of the peroneal nerve
Table 3. Negative Predictive Values of NCS Protocols
NCS protocols Negative predictive value (%)
(95% CI)
Peroneal 85.4 82.3-88.5
Tibial 85.9 82.9-89.0
Tibial F 90.3 87.6-93.1
Peroneal F 90.0 87.1-92.9
Peroneal + Tibial 87.6 84.6-90.6
Peroneal + Tibial F 92.0 89.5-94.6
Peroneal + Peroneal F 91.9 89.2-94.6
Tibial + Tibial F 91.9 89.3-94.5
Tibial + Peroneal F 92.9 90.3-95.4
Tibial F + Peroneal F 92.9 90.3-95.5
Tibial + Tibial F + Peroneal F (= protocol A) 94.3 92.0-96.7
Peroneal + Tibial F + Peroneal F (= protocol B) 94.3 91.9-96.7
Peroneal + Tibial + Tibial F (= protocol C) 93.0 90.6-95.5
Peroneal + Tibial + Peroneal F (= protocol D) 94.0 91.6-96.4
Peroneal + Tibial + Peroneal F + Tibial F (= protocol E) 94.7 92.0-97.5
Values are mean ± standard deviation, *p<0.05,
NCS: nerve conduction study, CI: confidence interval, Peroneal:peroneal compound muscle action potential (CMAP), Tibial: tibial CMAP, Tibial F: minimal F-response of the tibial nerve, Peroneal F: minimal F-response of the peroneal nerve
As a result, protocol B consisted of peroneal CMAP, a tibial F-response, and a peroneal F-response, had high negative predictive value (94.3%), and a significantly high frequency of abnormal values in asymptomatic patients, compared with the other NCS combinations.
DISCUSSION
To our knowledge, this study is the first to define a simplified NCS protocol for diabetic patients without neuropathic symptoms or signs. We suggested a simpli- fied NCS protocol which is composed four NCS parame- ters (sural SNAP + peroneal CMAP + peroneal F- response + tibial F-response). This NCS protocol has a high negative predictive value and a high frequency of abnormal values found in asymptomatic diabetic patients.
AAEM suggested that if the sural SANP and peroneal CMAP are normal in one lower extremity, there is no evidence of typical distal symmetric polyneuropathy, and so no further NCS is necessary.
11However, this rec- ommendation was not based on a clinical study or the results of previous studies. And this suggestion was not limited to DM PPN.
Four parameters (peroneal CMAP, peroneal F- response, tibial CMAP and tibial F-response) were selected based on the characteristics of DM PPN. DM
PPN is usually characterized by the severity of distal to proximal gradient with the longest nerves of lower extremities being affected earlier than the nerves of proximal or upper extremities.
12,13Therefore, our NCS protocols did not include median or ulnar NCS. In DM PPN, it is believed that sensory nerve conduction, espe- cially the sural nerve, is more impaired than motor nerve conduction.
14As we diagnosed DM PPN according to the diagnostic criteria proposed by the AAEM,
8we always included sural NCS in our NCS protocols.
Superficial peroneal SNAP and Hoffmann’s reflex (H- reflex) were not included in our NCS protocols. Superfi- cial peroneal SNAP was thought to be not elicited in
>5% of the normal population of any age group. It was difficult to obtain superficial peroneal SNAP due to motor artifact, anatomic variations, or technical errors of inexperienced investigators and it can show low ampli- tudes after middle age.
15,16H-reflex has many technical errors and it can also represent abnormal findings in older patients or patients with S1 radiculopathy.
17The H- reflex could also be very sensitive to changes in the external environment and body position.
18The SNAP is the summation of action potentials in sensory nerve axons evoked by the stimulus; its ampli- tude indirectly reflects the number of axons which can be activated. To record a SNAP uncontaminated by CMAPs, a mixed nerve can be stimulated and the SNAP
Table 4. Frequency of the Abnormal Value of Each NCS Protocol in Patients without Neuropathic SymptomsNCS protocols Frequency of abnormal value (%)
Peroneal 10.5
Tibial 10.0
Tibial F 19.4
Peroneal F 25.7
Peroneal + Tibial 13.8
Peroneal + Tibial F 22.6
Peroneal + Peroneal F 28.6
Tibial + Tibial F 21.7
Tibial + Peroneal F 28.8
Tibial F + Peroneal F 31.0
Tibial + Tibial F + Peroneal F (= protocol A) 32.8*
Peroneal + Tibial F + Peroneal F (= protocol B) 33.3*
Peroneal + Tibial + Tibial F (= protocol C) 24.5
Peroneal + Tibial + Peroneal F (= protocol D) 31.0
Peroneal + Tibial + Peroneal F + Tibial F (= protocol E) 34.0*
Values are mean ± standard deviation, *p<0.05
NCS: nerve conduction study, Frequency of abnormal value: The proportion of the subjects who have an abnormal value in any NCS parameter within the NCS protocol among the total 528 subjects without neuropathic symptoms, Peroneal:peroneal compound mus- cle action potential (CMAP), Tibial: tibial CMAP, Tibial F: minimal F-response of the tibial nerve, Peroneal F: minimal F-response of the peroneal nerve
recorded from a purely sensory branch or a pure sensory nerve can be investigated for stimulation and recording.
The purpose of sensory conduction studies in the diagno- sis of polyneuropathy is to assess whether there is loss of peripheral sensory axons rather than to detect demyelina- tion. Therefore, our criteria for the abnormality of SNAP, which are the delay of distal latency or the decrease of the amplitude, are slightly strict.
In the diagnosis of polyneuropathy, NCS is the most informative part of the electrodiagnostic evaluation. The inclusion of NCS in the assessment of polyneuropathy gives higher level of specificity for the diagnosis. Con- ventional electrophysiologic measurements such as nerve conduction velocity, compound action potential have been used to assess the severity of diabetic polyneuropathy and have been the major efficacy end points following pharmacologic intervention trials.
Unfortunately, these measurements are not particularly sensitive and their reproducibility is, at best, good.
NCS is relatively specific and reproducible method to detect the structural damage in large nerve fibers. One study reported that decreased sural SNAP amplitude and slowed peroneal CMAP CV correlate well with the char- acteristic structural lesion of myelinated nerve fibers in the patients with DM PPN.
19In recent studies, it was attempted to find more sensi- tive NCS parameters for diagnosing the subclinical stage of DM PPN.
9However, we did not consider more distal nerve studies which are known to be more sensitive, such as medial and lateral plantar nerve studies. There- fore, we may not diagnose the subclinical stage of DM PPN. However, this is not important because DM PPN is a clinical diagnosis based on a patient’s symptoms or clinical signs, and we excluded the patients with any neuropathic symptoms or signs.
In another study, the sural SNAP amplitude and per- oneal CMAP CV were sensitive enough to differentiate the status of the other NCS in 272 symptomatic diabetic patients with or without DM PPN.
10Some author said that minimal F-response of peroneal and tibial nerve were most sensitive parameter in diabetic patients.
20Considering the previous studies and our data, a sim- plified NCS protocol may be useful to define the exclu- sion of DM PPN. However, the abbreviated protocol is not sufficient to determine the subtype or severity of the PPN. For this purpose, additional NCS should be neces- sary if any of the simplified protocol shows abnormal response.
Study limitations
There are several limitations in the current study. First, our study is not a population-based or multicenter trial, there is also potential selection bias here. Further studies are needed to include a larger number of participants, different geographic locations and demographic factors.
The second limitation was that we did not consider normal control for setting a standard of abnormal NCS values. Abnormal NCS measures were defined as those with an amplitude lower than, and a slowed nerve con- duction relative to standard values of our electrodiagnos- tic laboratory.
Third, we did not include NCS of the upper extremi- ties, DM PPN has shown that the longest nerves of the lower extremities were affected earlier than the upper extremity nerves.
11,12However, results of ulnar CMAP and SNAPs were within the normal range and we already excluded subclinical CTS. Therefore, we may not diagnose DM PPN if it has a greater affect in the upper extremities.
Even though we excluded the subjects who had both EDB atrophy, many cases showed the decrease of per- oneal CMAP amplitude at EDB recordings and the low persistence of peroneal F wave at EDB recordings.
Therefore, abnormal peroneal NCS findings could be found without diabetic polyneuropathy. Additional study should be necessary regarding the association of polyneuropathy with peroneal nerve CMAP and F response.
Finally, subclinical CTS is more commonly seen in females. In our study, we excluded the patients with sub- clinical CTS, and men were enrolled more than women by 335:193. However, the gender ratio did not differ between patients with DM PPN and those without DM PPN (Table 1).
CONCLUSION
A simplified NCS protocol (distal latency and ampli-
tude of sural SNAP + distal latency, amplitude and con-
duction velocity of peroneal CMAP + latency of per-
oneal F-response + latency of tibial F-response) may be
initially used for diabetic patients without neuropathic
symptoms. If these patients show normal values in all
NCS parameters of the simplified NCS protocol, we can
rule out DM PPN without additional NCS. Through the
simplified NCS protocol, we can save time and expense,
and can decrease the patient’s pain or discomfort result- ing from multiple electrical stimuli during NCS.
REFERENCES
1. Bansal V, Kalita J, Misra UK: Diabetic neuropathy. Post- grad Med J 2006:82:95-100
2. Bril V: Role of electrophysiological studies in diabetic neuropathy. Can J Neurol Sci 1994:21:S8-12
3. Kim KT, Park BK, Ko HY: Sensitivity of Electrodiagnos- tic Parameters in Patients with Asymptomatic Diabetic Neuropathy. J Korean Acad Rehabil Med 2003:27:75-79 4. Dyck PJ: Detection, characterization, and staging of
polyneuropathy: assessed in diabetics. Muscle Nerve 1988:11:21-32
5. Dyck PJ, Kratz KM, Lehman KA, Karnes JL, Melton LJ, O’Brien PC, et al: The Rochester Diabetic Neuropathy Study: design, criteria for types of neuropathy, selection bias, and reproducibility of neuropathic tests. Neurology 1991:41:799-807
6. de Wytt CN, Jackson RV, Hockings GI, Joyner JM, Strakosch CR: Polyneuropathy in Australian outpatients with type II diabetes mellitus. J Diabetes Complications 1999:13:74-78
7. Kong X, Lesser EA, Potts FA, Gozani SN: Utilization of nerve conduction studies for the diagnosis of polyneuropa- thy in patients with diabetes: a retrospective analysis of a large patient series. J Diabetes Sci Technol 2008:2:268- 274
8. American Association of Electrodiagnostic Medicine:
Guidelines in electrodiagnostic medicine. Muscle Nerve 1999:22:s3-s300
9. Uluc K, Isak B, Borucu D, Temucin CM, Cetinkaya Y, Koytak PK, et al: Medial plantar and dorsal sural nerve conduction studies increase the sensitivity in the detection of neuropathy in diabetic patients. Clin Neurophysiol 2008:119:880-885
10. Hsu WC, Chiu YH, Chen WH, Chiu HC, Liou HH, Chen TH: Simplified electrodiagnostic criteria of diabetic polyneuropathy in field study (KCIS No. 14). Neuroepide-
miology 2007:28:50-55
11. England JD, Gronseth GS, Franklin G, Miller RG, Asbury AK, Carter GT, et al: Distal symmetrical polyneuropathy:
definition for clinical research. Muscle Nerve 2005:31:
113-123
12. Celiker R, Basgoze O, Bayraktar M: Early detection of neurological involvement in diabetes mellitus. Elec- tromyogr Clin Neurophysiol 1996:36:29-35
13. Donofrio PD, Albers JW: AAEM minimonograph #34:
polyneuropathy: classification by nerve conduction studies and electromyography. Muscle Nerve 1990:13:889-903 14. Thomas PK, Tomlinson DR: Diabetic and hypoglycemic
neuropathy. In: Dyck PJ, Thomas PK, Griffin JW, Low PA, Poduslo JF, editors. Peripheral Neuropahty, Philadel- phia: Saunders Press, 1993, pp1219-1250
15. Karlikaya G, Tanridag T, Yuksel G, Us O: Comparison of Two Different Methods for Superficial Peroneal Nerve Conduction Studies. The Internet Journal of Neurology 2005:4
16. Ko YA, Ko YJ, Kim HW, Lim SH, Yang BW, Jung SH, et al: Nerve Conduction Study of the Superficial Peroneal Sensory Distal Branches in Koreans. Ann Rehabil Med 2011:35:548-556
17. Alrowayeh HN, Sabbahi MA: H-reflex amplitude asym- metry is an earlier sign of nerve root involvement than latency in patients with S1 radiculopathy. BMC Res Notes 2011:4:102
18. Palmieri RM, Ingersoll CD, Hoffman MA: The hoffmann reflex: methodologic considerations and applications for use in sports medicine and athletic training research. J Athl Train 2004:39:268-277
19. Sima AA, Bril V, Nathaniel V, McEwen TA, Brown MB, Lattimer SA, et al: Regeneration and repair of myelinated fibers in sural-nerve biopsy specimens from patients with diabetic neuropathy treated with sorbinil. N Engl J Med 1988:319:548-555
20. Andersen H, Stalberg E, Falck B: F-wave latency, the most sensitive nerve conduction parameter in patients with diabetes mellitus. Muscle Nerve 1997:20:1296-1302