pISSN 2288-9272 eISSN 2383-8493 J Oral Med Pain 2019;44(1):16-24 https://doi.org/10.14476/jomp.2019.44.1.16
The Revised Version of the Minnesota Multiphasic Personality Inventory in Korean College Students with Symptoms of Temporomandibular Disorders
Hye Sook Park
Department of Dental Technology, Shingu College, Seongnam, Korea
Received February 11, 2019 Revised March 19, 2019 Accepted March 19, 2019
Purpose: The purpose of this study was to assess the association of personality characteris- tics with temporomandibular disorders (TMDs).
Methods: Four hundred and fifty one college students in Gyeonggi-do completed the re- vised version of the Minnesota Multiphasic Personality Inventory (MMPI-2) and a question- naire and collected data were analyzed by IBM SPSS Statistics ver. 25.0 software (IBM Co., Armonk, NY, USA).
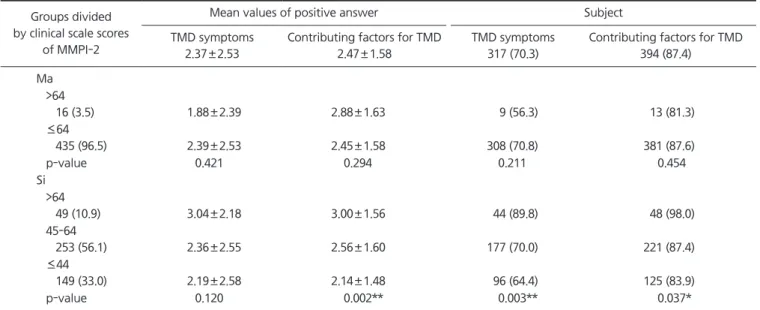
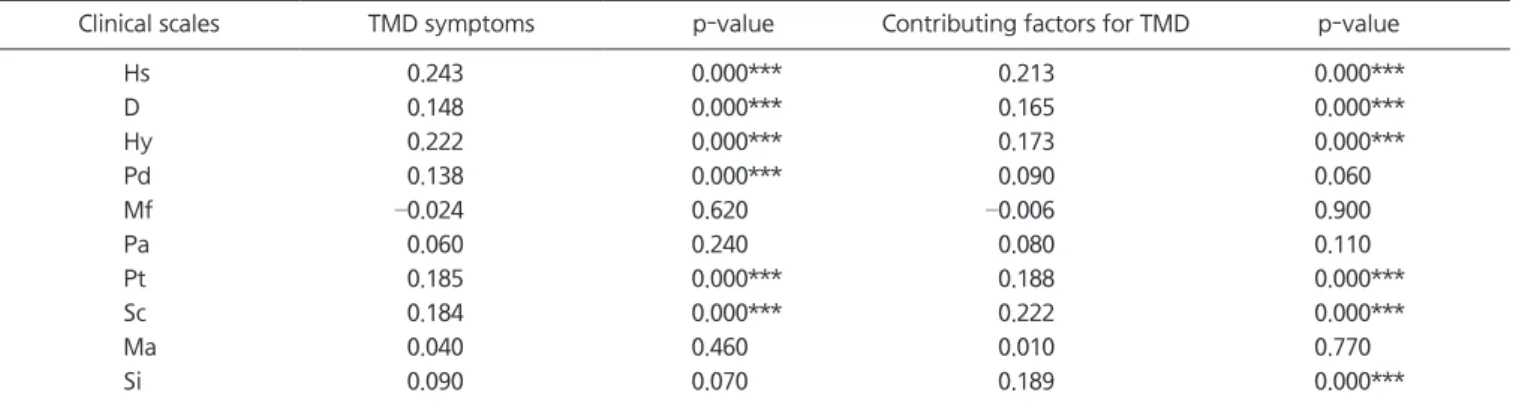
Results: Mean values of the number of positive answers of TMD symptoms were signifi- cantly higher in higher scorers on hypochondriasis (Hs), depression (D), paranoia (Pa) (Hs>60, D>64, Pa>59) (p<0.01). Higher scorers on Hs, hysteria (Hy), schizophrenia (Sc), Pa, psychas- thenia (Pt) (Hy>64, Sc>64, Pt>64) exhibited significantly higher mean values of the number of positive answers of contributing factors for TMD (p<0.01, p<0.001). Low scorers on social introversion (Si≤44) exhibited significantly lower mean value of the number of positive answers of contributing factors for TMD than high or moderate scorers on Si (Si>64, 45- 64) (p<0.01, p<0.05). The percentage of subjects who responded that they had at least one TMD symptom was significantly higher in higher scorers on Hs, Pt, D (p<0.05, p<0.01). The significantly higher percentage of higher scorers on D, Pa reported at least one contributing factor for TMD (p<0.05). The percentage of subjects who responded that they had at least one TMD symptom or one contributing factor for TMD was significantly different among three groups divided by T-score on Si (p<0.01, p<0.05). T-scores of Hs, D, Hy, Pt and Sc showed significant correlation with the numbers of TMD symptoms and contributing factors for TMD, respectively (p<0.001). A correlation was found between T-score of Pd and the number of TMD symptoms (p<0.001). T-score of Si correlated to the number of contributing factors for TMD (p<0.001).
Conclusions: Most clinical scales of MMPI-2 were found to be related to TMD. Psychologi- cal assessment including MMPI-2 may play a role in predicting treatment outcome and planning treatment of TMD.
Key Words: Contributing factor for temporomandibular disorder; Minnesota Multiphasic Personality Inventory-2; Personality; Temporomandibular disorder symptom
Correspondence to:
Hye Sook Park
Department of Dental Technology, Shingu College, 377 Gwangmyeong-ro, Seongnam 13174, Korea
Tel: +82-31-740-1575 Fax: +82-31-740-1589 E-mail: [email protected]
https://orcid.org/0000-0002-2981-3908 This study was supported by SCK
(Specialized College of Korea) of the Ministry of Education in 2018.
JOMP
Journal of Oral Medicine and PainCopyright Ⓒ 2019 Korean Academy of Orofacial Pain and Oral Medicine. All rights reserved.
CC This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/), which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.