의학
의학
의학
의학 석사학위
석사학위
석사학위
석사학위 논문
논문
논문
논문
Expression of Epidermal Growth
Expression of Epidermal Growth
Expression of Epidermal Growth
Expression of Epidermal Growth
Factor
Factor
Factor
Factor Receptor
Receptor
Receptor
Receptor in
in
in
in H
H
Hypopharyngeal
H
ypopharyngeal
ypopharyngeal
ypopharyngeal
C
C
C
Cancer and Effect of EGF in
ancer and Effect of EGF in
ancer and Effect of EGF in
ancer and Effect of EGF in
Progression of
Progression of
Progression of
Progression of H
H
H
Hypopharyngeal
ypopharyngeal
ypopharyngeal
ypopharyngeal
C
C
C
Cancer
ancer
ancer
ancer
아
아
아
아 주
주
주 대
주
대
대
대 학
학
학 교
학
교
교
교
대
대
대
대 학
학
학 원
학
원
원
원
의
의
의
의
학
학
학
학
과
과
과
과
김
김
김
김 윤
윤
윤
윤 태
태
태
태
Expression of Epidermal Growth
Expression of Epidermal Growth
Expression of Epidermal Growth
Expression of Epidermal Growth
Factor
Factor
Factor
Factor Receptor
Receptor
Receptor
Receptor in
in
in
in H
H
Hypopharyngeal
H
ypopharyngeal
ypopharyngeal
ypopharyngeal
C
C
C
Cancer and Eff
ancer and Eff
ancer and Eff
ancer and Effect of EGF in
ect of EGF in
ect of EGF in
ect of EGF in
P
P
P
Progression of
rogression of
rogression of H
rogression of
H
Hypopharyngeal
H
ypopharyngeal
ypopharyngeal
ypopharyngeal
C
C
C
Cancer
ancer
ancer
ancer
by
Yun Tae Kim
A Dissertation Submitted to The Graduate School of Ajou
University in Partial Fulfillment of the Requirements for the
Degree of
MASTER OF MEDICAL SCIENCES
Supervised by
Chul-Ho Kim, M.D., Ph.D.
Department of Medical Sciences
Department of Medical Sciences
Department of Medical Sciences
Department of Medical Sciences
The Graduate School, Ajou University
The Graduate School, Ajou University
The Graduate School, Ajou University
The Graduate School, Ajou University
August
August
August
김윤태
김윤태
김윤태
김윤태의
의
의
의 의학
의학
의학
의학 석사학위
석사학위
석사학위
석사학위 논문을
논문을
논문을 인준함
논문을
인준함
인준함
인준함....
심사위원장
심사위원장
심사위원장
심사위원장
김
김
김
김 철
철 호
철
철
호
호
호
인
인
인
인
심
심
심
심 사
사
사 위
사
위
위
위 원
원
원
원
박
박
박
박
기
기
기
기
현
현
현
현
인
인
인
인
심
심
심
심 사
사
사 위
사
위
위
위 원
원
원
원
정
정
정
정
연
연
연
연
훈
훈
훈
훈
인
인
인
인
아
아
아
아 주
주 대
주
주
대
대
대 학
학
학
학 교
교
교
교
대
대 학
대
대
학
학
학 원
원
원
원
2007
2007
2007
2007
년
년
년
년
6
6
6
6
월
월
월
월
22
22
22
22
일
일
일
일
-ABSTRACT-
Expression of Epidermal Growth Factor Receptor in
hypopharyngeal cancer and Effect of EGF in Progression of
hypopharyngeal cancer
Background and Objectives: The EGFR is a member of the erbB family of receptor
tyrosine kinase proteins, which also includes HER2/neu (erbB2), HER3 (erbB3), and HER4 (erbB4). High levels of EGFR expression are correlated with poor prognosis and resistance to radiation therapy in a variety of cancers, mostly in head and neck squamous cell carcinoma (HNSCC). So we examined the expression of EGFR in hypopharyngeal cancer and the effect of EGF in progression of hypopharyngeal SCC in the hypopharyngeal SCC cell line (FaDu).
Materials and Methods: We performed immunohistochemical stains on 57 specimens of
each normal mucosa and hypopharyngeal SCC with EGFR antibody. For Western blot, fresh normal and cancer tissue from the hypopharynx obtained from three patients were used. We performed RT-PCR and Western blot analyses of FaDu cells. Proliferative of the FaDu cells was assayed by counting the number of the cells after treatment by EGF of different concentration of 0, 10, 30 ng/㎖. Dispersion of the cells was observed by measuring the separation and morphologic changes of the cells after colony of FaDu cells was formed in the media and then was treated with EGF of 10ng/㎖ or 30ng/㎖ for 24 hours. Tumor cell invasiveness was assessed by the membrane invasion assay. RT-PCR and zymography were performed to examine the roles of matrix metalloproteinase-2(MMP-2) and MMP-9, as well as the relationship between EGF and MMPs in FaDu invasiveness.
Results: The positive rates of EGFR expression in hypopharyngeal SCC were 63.2%.
EGFR staining was significantly correlated with pathologic stage (p<0.05). The increased expresssion of EGFR mRNA(RT-PCR) and protein (Western Blot) were detected in hypopharyngeal cancer tissue. Exogenous EGF significantly enhanced the growth of FaDu
in a dose-dependent manner 30ng/㎖ (p<0.05). EGF markedly enhanced the invasiveness of cancer cells in a Transwell invasion chamber in a dose-dependent manner (p < 0.05). MMP expression was detected in the FaDu cells, and exogenous EGF enhanced the expression and its activity in the RT-PCR and zymogram analysis.
Conclusions: These results suggest that EGF may play an important role in the progression
of hypopharyngeal cancer.
Key words : EGF, EGFR, hypopharyngeal cancer, matrix metalloproteinase, proliferation, invasion
TABLE OF CONTENTS
ABSTRACT ... i
TABLE OF CONTENTS ... iii
LIST OF FIGURES...v
LIST OF TABLES ... vi
Ⅰ. INTRODUCTION... 1
Ⅱ. MATERIALS AND METHODS ... 3
A. MATERIALS ... 3
1. Patients ... 3
2. Immunohistochemistry ... 3
3. Cell and Cell culture ... 4
B. METHODS... 4
1. Reverse Transcriptase-Polymerase Chain Reaction ... 4
2. Western blotting ... 4
3. Effect of EGF on Proliferation ... 5
4. Effect of EGF on colony dispersion ... 5
5. Effect of EGF on wound healing ... 5
6. Effect of EGF on Invasion... 6
7. RT-PCR of MMP-2 and MMP-9 ... 6
8. Zymography of MMP-2 and MMP-9 ... 6
9. Statistical Methods ... 7
Ⅲ. RESULTS... 8
A. Expression of EGFR in Human Hypopharyngeal Caner Tissue ... 8
B. Western blot in hypopharyngeal cancer tissue and RT-PCR and Western blot in Human Hypopharyngeal Cancer Cells ... 11
C. Effect of EGF on proliferation of FaDu cells ... 13
D. Effect of EGF on colony dispersion ... 14
F. Effect of EGFR on Cell Invasion ... 16 G. RT-PCR of MMP-2 and MMP-9... 17 H. Zymography of MMP-2 and MMP-9 ... 18 Ⅳ. DISCUSSION... 19 Ⅴ. CONCLUSION ... 23 REFERENCES ... 24 국문요약 ... 32
LIST OF FIGURES
Fig. 1. A: Immunohistochemistry ... 9
B: Survival rate... 9
Fig. 2. Expression of EGFR in human pharyngeal cancer tissues...11
Fig. 3. Analysis of expression of EGF and EGFR in the FaDu cell line ... 12
Fig. 4. Proliferative activity of EGF ... 13
Fig. 5. Scatter activity of EGF. ... 14
Fig. 6. Wound healing activity of EGF... 15
Fig. 7. Invasion assay of EGF ... 16
LIST OF TABLE
Table 1. Correlation between the Expression Pattern of EGFR and Clinicopathologic Factors ... 10
I.
Introduction
With over 500,000 cases worldwide and a high mortality rate, head and neck squamous cell carcinoma (HNSCC) is the sixth most common cancer in men. Even with improved treatments, the overall survival rate has been less than 50% for the past 30 years(Greenlee, et al,2001). Among cancers of the head and neck, hypopharyngeal carcinoma has very high invasion and metastasis rates, making locoregional control of these cancers difficult. The 5- year overall survival rate for all patients with hypopharyngeal carcinoma is only 30%, which is essentially unchanged from the rate recorded two decades ago, in spite of various treatment trials. An understanding of the mediators of the critical steps in the metastatic process is essential for the development of targeted therapies for hypopharyngeal carcinoma.
Patients with advanced HNSCC are at greatest risk for recurrence, but the TNM system for tumor staging is inadequate for distinguishing outcome and tailoring therapy in these patients. The characterization of the molecular mechanisms involved in the pathogenesis of HNSCC has been undertaken to develop new approaches for identifying patients at highest risk for progression or recurrence of disease and to select patients who could benefit from multimodal and molecularly targeted therapies.
Recent research efforts have attempted to exploit biologic differences that may exist between normal and malignant cells, to develop tumor-specific therapies. The epidermal growth factor (EGF) and its receptor (EGFR, ErbB-1, or HER-1) were not only shown to play an influential role in cellular growth and differentiation in healthy tissues, but also in tumorigenesis and the progression of malignant disease(Arteaga,2003). As well as being expressed on the surface of healthy cells, the EGFR is commonly expressed at high levels in a variety of epithelial tumors, including HNSCC. The aberrant activation of the EGFR leads to enhanced proliferation and other tumour-promoting activities, which provide a strong rationale to target this receptor. During the past decade, intense research has initiated a new era of cancer treatment, that of molecular therapeutics. Today, the EGFR is a prime target for new anticancer therapy, with a broad range of inhibitors currently under investigation (Baselga,2001). Promising preclinical studies have prompted the development of clinical trials testing EGFR inhibitors as single agent therapy or in combination with conventional cytotoxic therapy, with response rates lower than anticipated in the advanced disease setting.
The clearest benefit of EGFR-inhibitor treatment to date is noted when it is combined with RT to treat locally advanced head and neck cancer(Bonner, et al,2006).
In normal cells, the expression of EGFR ranges from 40,000 to 100,000 receptors per cell(Carpenter and Cohen,1979). In HNSCC, EGFR and its ligand, TGF, are overexpressed in 80–90% of cases; the corresponding magnitudes of increase are 1.7-fold (P = 0.005) and 1.9-fold (P = 0.006) respectively, when compared to controls(Grandis and Tweardy,1993). The nature of the protein overexpression is thought to result from enhanced transcription, with no apparent change in mRNA stability; gene amplification has been observed less frequently. Overexpression of EGFR is observed in 42% to 80% of HNSCCs studied(Miyaguchi, et al,1991). Grandis et al. demonstrated that EGFR overexpression provided independent prognostic value for both local control and survival in 91 head and neck squamous carcinoma patients treated with surgical resection - postoperative radiotherapy(Rubin Grandis, et al,1998). EGFR overexpression was also associated with both an increased risk of local relapse and an adverse overall survival, independent of tumor stage.
Therefore we investigated the expression and distribution of the EGFR in hypopharyngeal squamous cell carcinoma by immunohistochemistry and effect of EGF in progression of hypopharyngeal SCC in the hypopharyngeal SCC cell line.
II.
Materials and methods
A. Material 1. Patients
57 patients admitted for hypopharyngeal squamous cell carcinoma at Ajou University Hospital and Yonsei University Medical Center in Korea were enrolled in this study between 1994 and 2002. Surgically removed specimens of hypopharyngeal squamous cell carcinoma, excluding carcinoma in situ and verrucous carcinoma were used. None of the patients had undergone radiotherapy or chemotherapy before surgical excision. The tumors were classified according to the 2002 AJCC TNM classification system. The average age at clinical onset was 60 years, with a range of 37-76 years. 6 patients had stage I or II disease and 51 patients, stage III or IV. The histologic typing was based on the World Health Organization (WHO) system. Of the 57 tumors, 13 were well differentiated, 29 moderately differentiated, and 15 poorly differentiated.
2. Immunohistochemistry
Formalin-fixed, paraffin-embedded tissue was cut into 5-µm sections and then dewaxed and rehydrated via serial passage through xylene and a graded series of ethanol. Endogenous peroxidase activity was blocked by incubation for 45 minutes in 6% hydrogen peroxide in methanol. The primary antibodies were a human EGFR polyclonal antibody used in a concentration of 50µg/㎖ (Cell Signaling technology, Danvers, MA). Primary antibody incubations were carried out for 2 hours at 25℃. The sections were extensively washed in phosphate-buffered saline and then incubated with the appropriate biotinylated second antibody followed by avidin-peroxidase. Goat and rabbit Vectastain-elite immunoperoxidase kits (Vector Laboratories, Burlington, VT) were purchased for this purpose and were used in accordance with manufacturer’s instructions. The chromogenic reaction was carried out with 3-3'-diaminobenzidine in a peroxidase substrate solution and lasted 4 minutes. Haematoxyline was used for nuclear staining. For each experiment, negative controls omitting either primary or secondary antibodies were included to examine nonspecific staining. The slides were reviewed by at least two pathologists and scored
semiquantitatively as follows: - no staining, ± definite but weak staining, + moderate staining, and ++ strong staining. Tumor samples were scored positive if tumor cells were scored + or ++ and stained more than 30% of cancer cells.
3. Cell and Cell culture
FaDu cells, a hypopharyngeal cancer cell line, were obtained from American Type Culture Collection (ATCC) and were cultured in Eagle’s minimum essential medium containing 25 mM NaHCO3 (EMEM), 10% FBS, glutamine, 1% essential amino acids, vitamine, and streptomycin under 5% CO2 atmosphere at 37℃ .
B. Methods
1. Reverse Transcriptase–Polymerase Chain Reaction
Total RNA from fresh hypopharyngeal cancer tissues and FaDu cells was extracted using TRIzol® (Invitrogen, Groningen, Netherlands). cDNA was prepared using the Omniscript Reverse Transcriptase kit (Qiagen, Germany) according to the manufacturer’s instructions. To determine the effects of EGF, cells were treated with EGF (0, 10ng/㎖, 30ng/㎖). The sequences of PCR primers were as follows: EGF-F: 5′-ACA TCG TCA CTT CTG GC-3′; EGF-R: 5′-ATC CAT CCT ATG TTT GTT CG-3′; EGFR-F: 5′-AGT AGC CTG ATT GTG CAT TT-3′; EGFR-R: 5′-TCT TTC ATG ATG CCC TC-3′. PCR products were separated by electrophoresis in 1.5% agarose gels and were detected under UV light (Bio-Rad, Hercules, CA).
2. Western blotting
Fresh hypopharyngeal cancer tissues were prepared, and exponentially growing cells in 10cm2 dishes were rinsed several times with phosphate-buffered saline (PBS) and fed with EMEM supplemented with 10% fetal bovine serum and human recombinant EGF (0, 10 ng/
㎖, 30 ng/㎖) (R&D Systems Inc., Minneapolis, MN, USA). The cells were cultured for 3
days in a humidified CO2 incubator. Control cells were similarly washed and cultured in medium without EGF. Cells were washed with PBS and extracted with EBC buffer (120 mmol/L NaCl, 0.5% NP-40, 40 mmol/L Tris, pH 8.0, 1 mmol/L EDTA) with protease
inhibitors (100 µg/㎖ of phenylmethylsulfonyl fluoride and 1 µg/㎖ leupeptin). The extracts were centrifuged at 10,000 g for 10 minutes; the supernatants were used for Western blot analyses. Protein content was measured with a Bio-Rad protein assay kit (Bio-Rad, Hercules, CA). Twenty micrograms of protein was resolved by SDS-polyacrylamide gel electrophoresis, transferred to nitrocellulose filters (Amersham, Arlington Heights, IL), and incubated overnight at 4°C with EGFR antibodies, anti-human EGF antibodies. After washing, the filters were incubated with peroxidase-conjugated donkey anti-rabbit antibody (Amersham) or donkey anti-mouse antibody (Amersham) and were visualized using an enhanced chemiluminescence detection system (Amersham).
3. Effect of EGF on Proliferation
FaDu cells were plated in culture plates(Coster, Cambridge, MA, USA) at a density of approximately 1ⅹ105
/well in the absence of serum. EGF(0, 10ng/㎖, 30ng/㎖) was added and cells were cultured for 5 days. Cells were counted by haemocytometer at Day 1, Day 3, and Day 5. 7 separate experiments were done to obtain statistically significance.
4. Effect of EGF on Colony dispersion
FaDu cells were subcultured and maintained in growth medium until colonies >16 cells were established. Cultures were then deprived of growth factors and serum for 48 hours prior to treatment with EGF (0, 10ng/㎖, 30ng/㎖) at the times and conducted in cells pretreated for 2 hours with mitomycin C (8 ㎍/㎖). To confirm the effect of EGF, cells were treated with EGF (0, 10ng/㎖, 30ng/㎖). Colony dispersion was documented by photography at 6 hours, 12 hours, 18 hours, and 24 hours.
5. Wound healing assay
FaDu cells were plated in culture plates at a density of approximately 1ⅹ105
/well in the absence of serum. Confluent cell monolayers were then deprived of growth factors for 48 hours and a cell-free area was introduced by scraping the monolayer with a sterile pipette tip followed by extensive washing to remove cellular debris. In vitro reepithelialization was monitored by the repopulation of the cleared area with cells over time. To confirm the effect
of EGF, cells were treated with EGF(0, 10ng/㎖, 30ng/㎖). Wound healing was documented by photography at 12, 24, 36 and 48 hours.
For objective measurements, distance between both side was measured by computer calculator at five points(per one field) in 48 hours. The average distance at seven fields was compared each other( control vs EGF treatment group and EGF 10ng/㎖ vs EGF 30ng/㎖).
6. Effect of EGF on Invasion
Transwell chambers (Costar) were used to verify the degree of invasiveness depending on the administration of EGF. First, type I collagen (6 ㎍/filter) melted in EMEM 100 ㎕ was poured into the upper part of a polyethylene filter (8 ㎛ pore-sized); coating was carried out in a laminar flow hood for one night. 500 ㎕ of 0.5% FBS medium was put into the lower part of each well, and the wells were adjusted to EGF densities of 0, 10, and 30 ng/㎕. After preprocessing with mitomycin C (8 ㎍/㎖) for 30 minutes, 105 cells (in 100 ㎕ of growth medium) were attached to the top of the filter of the upper well. After this chamber was cultivated in 5% CO2 at 37℃ for 48 hours, the filter of the upper well was removed and the cells passed through the pore. The attached cells on the lower part were dyed with hematoxylin and counted using a light microscope.
7. RT-PCR of MMP-2 and MMP-9
Using 50-100 ㎎ of frozen FaDu cells, RNA was prepared as described above. The primer pairs used for MMP-2 and MMP-9 were as follows;
MMP-2-F, 5'-ACCTGGATGCCGTCGTGGAC-3'; and MMP-2-R, 5'-TGTGGCAGCACCAGGGCAGC-3'; and MMP-9-F, 5'-GGGGAAGATGCTGCTGTTCA-3' and MMP-9-R, 5'-GGTCCCAGTGGGGATTTACA-5'-GGGGAAGATGCTGCTGTTCA-3'. After denaturation for 3 minutes at 96℃, the samples were amplified by PCR for 30 cycles of 30 seconds at 96℃,
30 seconds at 55℃, and 30 seconds in 72℃, with extension for 5 minutes at 72℃ .
8. Zymography of MMP-2 and MMP-9
Cultures were deprived of growth factors and serum for 48 hours prior to treatment with EGF (0, 10 ng/㎖, 30 ng/㎖) for the indicated periods of time. After quantification of the
protein in the supernatant, 30 ㎍ of protein from each sample was mixed with 15 ㎕ APMA and the samples were activated for 1 hour at 37℃. Cytoplasm samples were obtained after 24 hours using the MightySlim™ SX 250 (Hoefer, San Francisco, CA, USA) process. Each 10 ㎕ sample was placed in sample buffer for 10 minutes, and then electrophoresed in a polyacrylamide gel at 125 V for 120 minutes at 4℃ using the Novex XCell II. The gel was incubated in renaturation buffer for 60 minutes at room temperature, and then incubated in 100 ㎖ of developing buffer at 37℃ for 18 hours with light shaking. The gel was stained with Coomassie blue for 3 hours and washed with water. After decolorization in 400 ㎖ methanol, 100 ㎖ acetic acid, and 500 ㎖ distilled water, cell images were taken every 10 minutes using an image analyzer.
9. Statistical Methods
Student’s t test and one-way ANOVA test (for the invasion assay) were used for statistical analyses of the data. Patient survival rates were calculated using the Kaplan-Meier method, and statistically significant differences in survival were identified using the log-rank test. All statistical analyses were conducted using SPSS 10.0 statistical software (SPSS, Chicago, IL). A p value of less than 0.05 was considered statistically significant.
III.
Results
A. Expression of EGFR in Human Hypopharyngeal Cancer Tissue
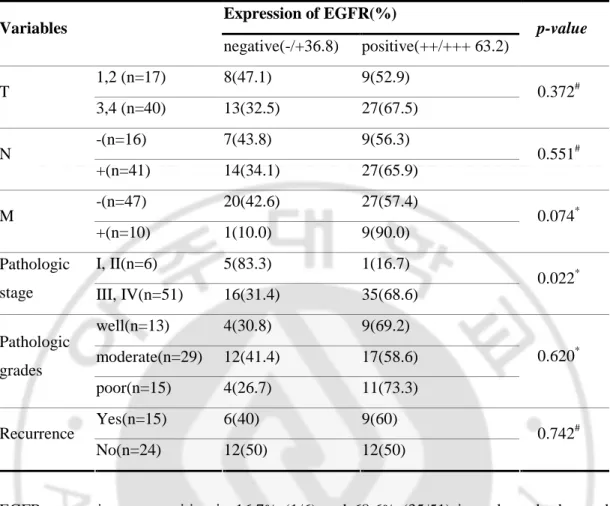
EGFR overexpression was observed in 63.2%(36/59) of hypopharyngeal cancer tissues. In most of the specimens, EGFR expression was primarily seen in the cell membrane and the cytoplasm of cancer cells (Fig. 1A). The rate of EGFR expression was 52.9% in patients with tumors less than 4 cm (stage T1 or T2) and 67.5% in tumors more than 4 cm (stage T3 and T4). Thus, it could be observed that the expression of EGFR increased according to tumor size. However, there was no statistical significance (Table 1). In cases of lymph node metastasis, EGFR expression was observed in 36 out of 57 (63.1%). But, a statistically nonsignificant increase in EGFR expression was seen in 27 out of 41 cases (65.9%) where there was lymph node metastasis. EGFR expression seemed to be increased in cases of distant metastasis (90%), however there was no significant difference compared to those without distant metastasis (57.4 %). EGFR expression was positive in 16.7% (1/6) and 68.6% (35/51) in early and advanced stage carcinoma, respectively, demonstrating that there was a significant increase in EGFR expression according to tumor stage (p<0.05). Pathologic cell differentiation did not seem to affect EGFR expression. There was no statistically significant difference between groups with and without recurrence (60%, 50%). Of the 57 patients, 20 (35.1%) died during the follow up period. The cause of death was local recurrence in 11 cases, distant metastasis in 9 cases, and both in no case. Survival analysis was performed using the Kaplan-Meier method and the statistical significance was evaluated by the log-rank test(Fig. 1B). There showed a difference of survival rate between the groups with negative and positive EGFR expression, but the p-value was 0.053, resulting in no statistical significance.
Fig. 1. A: Immunohistochemistry: Paraffin sections of hypopharyngeal carcinomas
immunostained for EGFR : EGFR staining was primarily observed in the membrane of the cancer cells, but was seen occasionally seen in the both membrane and cytoplasm of cancer cells(200x). A: no staining, B: definite but weak staining (±), C: moderate staining (+), D: strong staining (++) B: Survival rate: Five-year survival of 59 patients with hypopharyngeal carcinoma according to EGFR expression. Survival was significantly poorer in patients with positive EGFR expression compared with the negative EGFR expression (p = 0.053).
Table 1. Correlation between the Expression Pattern of EGFR and Clinicopathologic Factors Expression of EGFR(%) Variables negative(-/+36.8) positive(++/+++ 63.2) p-value 1,2 (n=17) 8(47.1) 9(52.9) T 3,4 (n=40) 13(32.5) 27(67.5) 0.372# -(n=16) 7(43.8) 9(56.3) N +(n=41) 14(34.1) 27(65.9) 0.551# -(n=47) 20(42.6) 27(57.4) M +(n=10) 1(10.0) 9(90.0) 0.074* I, II(n=6) 5(83.3) 1(16.7) Pathologic
stage III, IV(n=51) 16(31.4) 35(68.6)
0.022* well(n=13) 4(30.8) 9(69.2) moderate(n=29) 12(41.4) 17(58.6) Pathologic grades poor(n=15) 4(26.7) 11(73.3) 0.620* Yes(n=15) 6(40) 9(60) Recurrence No(n=24) 12(50) 12(50) 0.742#
EGFR expression was positive in 16.7% (1/6) and 68.6% (35/51) in early and advanced stage carcinoma, respectively, demonstrating that there was a significant increase in EGFR expression according to tumor stage (p<0.05). It was seemed that other variables(T, N, M, grade, recurrence) were correlated with expression of EGFR, but there was not significant. # calculated by Pearson Chi-Square's test (p<0.05)
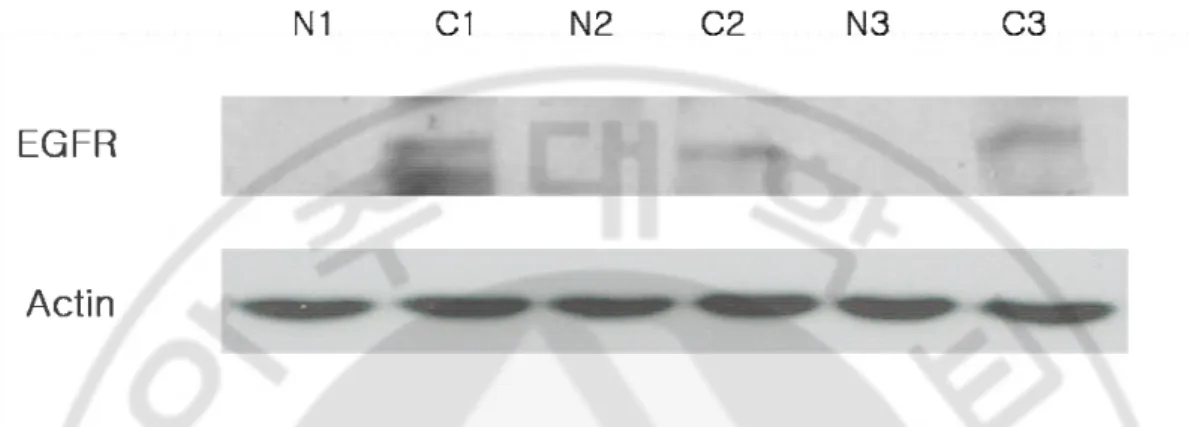
B. Western Blot in Hypopharyngeal Cancer Tissue and RT-PCR and Western Blot in human Hypopharyngeal Cancer Cell Line
Western blotting was performed on the 3 patients, and EGFR was strongly expressed in the carcinoma cells and not in the normal tissues (Fig. 2).
Fig. 2. Expression of EGFR in human pharyngeal cancer tissues. Western blotting
demonstrated that EGFR was strong expressed in carcinomas in comparison with normal tissues.
The expression of EGFR mRNA by FaDu cells was detected by RT-PCR, and the EGFR protein content was detected by Western blotting. However, EGF was not detected by either RT-PCR or Western blotting (Fig. 3).
Fig. 3. Analysis of expression of EGF and EGFR in the FaDu cell line. A: RT-PCR:
The expression of EGF and EGFR mRNA was measured by RT-PCR in the hypopharyngeal cancer line FaDu. B: Western blotting: Detection of the EGFR protein in FaDu cells by Western blotting. EGF was not detected by either RT-PCR or Western blot analysis.
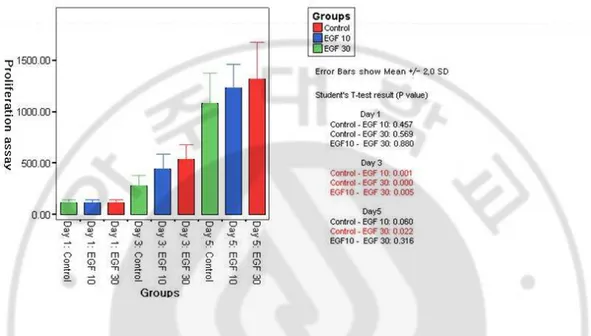
C. Effect of EGF on proliferation of FaDu cells
EGF stimulated statistically significant increase in proliferation of FaDu cells on 3rd and 5th days respectively (p<0.05). It showed the result that the case of EGF 30ng/ ㎖ considerably increased the proliferation than the case of control and 10ng/㎖ on 3rd days (Fig. 4).
Fig. 4. Proliferative acitivity of EGF. Proliferative assay of FaDu cells after treatment with
EGF for 5 days. Exogenous EGF significantly enhanced the growth of FaDu in a dose-dependent manner(* : p<0.05. calculated by one-way ANOVA).
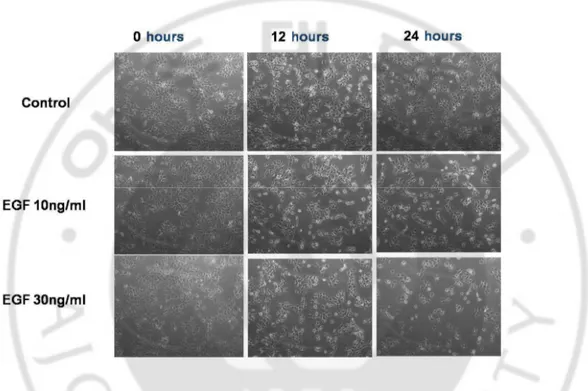
D. Effect of EGFR on colony dispersion
In the control, there was no significant colony dispersion of the FaDu cells. In EGF treated groups, the FaDu cells dissociated 24 hours after treatment (Fig. 5). After 6 hours, the formation of actin microspikes (filopodia) and membrane ruffling (lamellipodia) were observed, and cell shape changed to the spindle-like features (Fig. 4). This result suggests that EGF may be associated with scattering. Although we did not measure the objective scattering effect according to the concentration of EGF, 30 ng/㎖ seemed to produce a more potent scattering effect than 10 ng/㎖ 24 hours after EGF stimulation.
Fig. 5. Scatter activity of EGF. FaDu cells were cultured (A) without treatment (control),
(B) with EGF 10 ng/㎖, or (C) EGF 30 ng/㎖ for 24 hours (Original magnification, 150x). In control group, significant colony dispersion of FaDu cells didn’t happen. In EGF treated groups, EGF significantly increased dispersion of FaDu cells. EGF 30 ng/㎖ seemed to be more potent scattering effect than EGF 10 ng/㎖ at 24 hours after EGF stimulation.
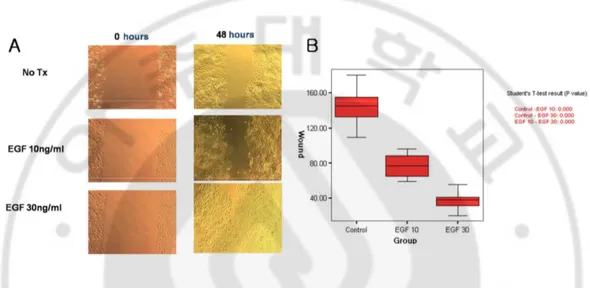
E. Effect of EGF on Wound Healing assay
In order to assess the contributions of EGF to both migratory and proliferative activities, we performed the in vitro wound healing assay of FaDu cells with EGF(0, 10ng/㎖, 30ng/㎖). Exogenous EGF significantly enhanced the migration and proliferation of FaDu in dose dependant manner (Fig. 6). EGF 10 ng/㎖ led to a mean 1.65±0.93-fold increase in cell migration (p < 0.05 versus control), and EGF 30 ng/㎖ led to a mean 4.42±2.59-fold increase in cell migration (p < 0.05 versus control) . EGF 30 ng/㎖ led to a mean 2.67±1.22-fold increase in cell migration (p < 0.05 versus EGF 10 ng/㎖).
Fig. 6. Wound healing assay of EGF. Wound healing assay of FaDu cells after treatment
of EGF. Exogenous EGF enhanced the migration and proliferation of FaDu in dose-dependant manner (p<0.05. calculated by one-way ANOVA). A: microscopic findings, B: graph
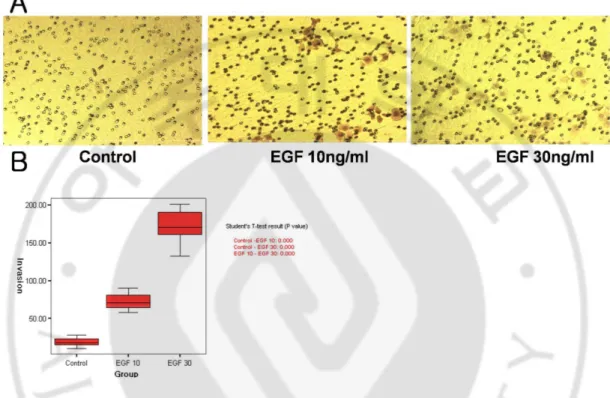
F. Effect of EGFR on Cell Invasion
The effect of EGF on FaDu cell invasion was evaluated using a Type 1 collagen-coated Transwell invasion assay. EGF at 10 ng/㎖ led to a mean 4±1.5-fold increase in cell invasion (p < 0.05 versus control), and EGF at 30 ng/㎖ led to a mean 8.5±2-fold increase in cell invasion (p < 0.05 versus control) (Fig. 7). EGF 30 ng/㎖ led to a mean 2.5±0.5-fold increase in cell invasion (p < 0.05 versus EGF 10 ng/㎖).
Fig. 7. Invasion assay of EGF. A,B: Invasion assay of FaDu cells using a Transwell
chamber after treatment with EGF. FaDu cells seeded on the upper membrane in the presence (10, 30 ng/㎖) or absence of recombinant EGF in the lower compartment. After a 48-hour incubation, plugged cells in the 8-µm pore or cells attached to the undersurface or the membrane were counted. The bars show the SD of triplicate samples. Data are representative of 3 separate experiments with similar results. EGF significantly promoted the invasion ability of FaDu cells in a dose-dependent manner. *p < 0.05 versus untreated cells. ** p < 0.05 versus cells treated with 10. ng/㎖
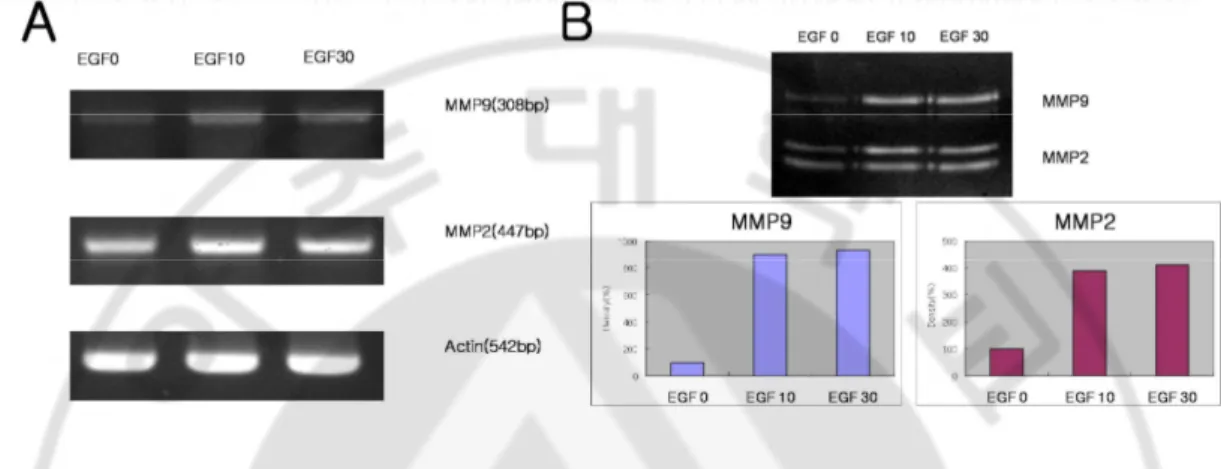
G. RT-PCR of MMP-2 and MMP-9
RT-PCR of FaDu cells after EGF treatment for 24 hours showed a marked increase in MMP-2. There was no significant difference between EGF at 10 ng/㎖ and EGF at 30 ng/
㎖. In the case of MMP-9 in FaDu cells after EGF treatment, RT-PCR showed a slight
increase in the level of MMP-9 for the EGF treatment group as compared to the control group (Fig. 8A).
Fig. 8. Induction of MMP-2 and MMP-9 activities by EGF. A: RT-PCR of MMP-2 and MMP-9 in FaDu cells. Detection of expression of MMP-2 and MMP-9 in FaDu cells
treated for 24 hours with 0, 10, and 30 ng/㎖ EGF. Exogenous EGF slightly enhanced MMP-2 and MMP-9 expression. B: Zymography. FaDu cells were serum-deprived for 48 hours, and then incubated with fresh medium that contained EGF (10 or 30 ng/㎖). The conditioned media were collected after 24 and 48 hours. The samples were fractionated on a polyacrylamide gel that contained 0.1% gelatin, and a zymogram was developed as described in the Materials and Methods section. The 92- and 72-kDa gelatinase activity bands, as determined relative to the molecular weight standards, are indicated by the solid arrows. The level of MMP-2 and MMP-9 activity was increased after EGF treatment for 24 hours as compared to the control group. However, there was no significant difference between the 10 and 30 ng/㎖ EGF treatment groups.
H. Zymography of MMP-2 and MMP-9
MMP-2 activity was slightly increased after 24 hours in the EGF treatment group as compared to the control group. There was no significant difference between EGF at 10 ng/
㎖ and EGF at 30 ng/㎖. MMP-9 activity after EGF treatment was increased at 24 hours,
although there was no significant difference between EGF at 10 ng/㎖ and EGF at 30 ng/㎖. (Fig. 8B).
IV.
Discussion
EGFR is a glycoprotein of 170 kDa, encoded by a gene located on chromosome 7p12 (Davies, et al,1980). The EGFR is a member of the erbB family of receptor tyrosine kinase proteins, which also includes HER2/neu (erbB2), HER3 (erbB3), and HER4 (erbB4). These receptors are composed of an extracellular ligand-binding domain, a transmembrane lipophilic domain, and an intracellular tyrosine kinase domain and, with the exception of HER2, all bind to receptor-specific ligands. Phosphorylation of the tyrosine kinase domain followed by homodimerization or heterodimerization between different receptors of the same family leads to protein activation(Lemmon and Schlessinger,1994). Receptor dimerization is promoted by ligand binding, high receptor density from over-expression, and mutations in the kinase domain. Protein activation on the cell surface of cancer cells is believed to promote signaling cascades, cell growth, differentiation, cell survival (apoptosis), drug and radiation sensitivity, cell cycle progression, and angiogenesis(Ono and Kuwano,2006).
In resting, nontransformed cells, EGFR signaling is tightly controlled. However, oncogenic activation of this pathway occurs as a result of EGFR mutation, overexpression, structural rearrangements, and/or relief of its normal autoinhibitory and regulatory constraints(Arteaga,2001). The evidence to support a role for the EGFR proto-oncogene in transformation was provided by the demonstration that the EGFR is the cellular homolog (proto-oncogene) of the avian erythroblastosis virus v-erbB oncogene (AEV). AEV encodes a C-terminus truncated form of erbB1 (v-erbB) that lacks the EC domain and exhibits several intracellular mutations, resulting in ligand-independent dimerization and phosphorylation(Downward, et al,1984). Binding of EGF-superfamily growth factors to EGF-R activates four major pathways, that is, the phosphatidylinositol-3 kinase (PI-3 kinase), signal transducer and activator of transcription (STAT), phospholipase C-protein kinase C (PLC-PKC), and Ras-mitogen-activated protein kinase (Ras-MAPK) pathways(Prenzel, et al,2001;Yarden and Sliwkowski,2001). All these pathways have been implicated in growth control and survival. In addition, EGF-R-mediated activation of PLC and MAPKs have been linked to migration and invasion (Chen, et al,1994;Cheresh, et al,1999;Glading, et al,2000;Xie, et al,1998).
Several other human cancers, including cancers of colon, pancreas, breast, ovary, bladder, kidney, and gliomas, display EGFR RNA and/or protein overexpression. This occurs with or without EGFR gene amplification and often is associated with increased expression of TGF or amphiregulin(Ekstrand, et al,1991;Hirai, et al,1998;Klijn, et al,1992;Rubin Grandis, et al,1998;Rusch, et al,1993;Salomon, et al,1995;Tateishi, et al,1990;Yamanaka, et al,1993;Yonemura, et al,1992). In some of these studies, EGFR-positive tumors that coexpressed receptor ligands exhibited higher proliferation and tumor grade and a worse survival than EGFR-expressing tumors without coexpression of receptor ligands(Hirai, et al,1998;Tateishi, et al,1990;Yonemura, et al,1992).
Growth and differentiation of HNSCC are regulated by several growth factors and their surface receptors. EGFR is up-regulated in several carcinomas. It is a transmembrane glycoprotein encoded by c-erb-B2 proto-oncogene. This protein is expressed at a low level in many normal human tissues, but activation of the c-erb-B2 oncogene results in its over-expression, seen in many human cancers. The density of EGFR varies from none on lymphoid cells to a high of 250 000/cell on keratinocytes(Cowley, et al,1984;Cowley, et al,1986;Gusterson, et al,1985). In HNSCC, EGFR is not only an independent prognostic factor of outcome in multivariate analysis, but also a first choice therapeutic target. The recent demonstration of a significant survival benefit when combining cetuximab with external radiation therapy is a major breakthrough in the management of HNSCC, establishing a new treatment option for locally advanced HNSCC. This trial provided also an important proof of principle that targeting a pertinent signaling pathway can enhance the radiation response of tumors. However, the improvement in the loco-regional control rate has been modest (within the range achieved with concurrent radiotherapy and chemotherapy) and more than half of patients receiving radiotherapy plus cetuximab still experienced local-regional relapse (Bonner, et al,2006). Therefore, there is a need to further improve outcome. Ongoing clinical efforts are devoted to address whether the addition of cetuximab to concurrent chemoradiation can yield a better outcome (i.e., RTOG study 0522). At this point, it has to be reminded that cancer cells rely on several, sometimes, redundant activation pathways; EGFR is only one of them. The risk of treatment failure is real, if only one receptor is targeted, hence the interest in combining broader range tyrosine
kinase inhibitors such as CI-1033, which targets all four members of the Erb family (pan ErbB)(Zimmermann, et al,2006). In head and neck cancer patients receiving 5-fluorouracil it was known that EGFR remains the tumor parameter with the highest prognostic impact(Etienne, et al,1999). The relationship between EGFR over-expression, increased tumour size and/or local extent of primary tumors (T classification) has been described in previous studies(Putti, et al,2002). And in other study multivalate analysis showed that N status was the most powerful clinical prognostic factor and the EGFR level of expression appears to be a major prognostic factor in the population of patients with an resectable larynx and hypopharynx cancer treated by induction chemotherapy and radiotherapy. In several studies it was suggested that EGFR expression correlates with prognosis in advanced laryngeal carcinoma (stage III and IV)(Smith, et al,2001). On the other hand, several other studies also showed no significant correlation between EGFR expression and tumour prognosis in HNSCC(Kusukawa, et al,1996). Logically, it is justified to target the cellular factor linked with the unfavorable tumor outcome at a selected group of patients. Currently, two options are under clinical development using specific inhibitors of the EGFR tyrosine kinase enzyme and monoclonal antibodies directed at the external domain of the EGFR. The inhibitors of the EGFR tyrosine kinase stop the autophosphorylation of the EGFR, and block the mitotic signal driven by EGFR activation. Among them, ZD1839 (Iressa™) and OSI774 (tarceva™) have demonstrated activity alone and in combination with cytotoxic drugs in a variety of cell lines and xenograft tumors and promising results have been obtained in early clinical studies(Ciardiello, et al,2000;LoRusso, et al,2003;Magne, et al,2003;Magne, et al,2002;Magne, et al,2002;Magne, et al,2003;Soulieres, et al,2004). Monoclonal antibodies targeting EGFR are available (C225, Cetuximab™) and have demonstrated their effectiveness against a human tumor xenograft in animal models. Early clinical trials have shown significant clinical activity in combination with cisplatin or with radiotherapy in head and neck cancer patients(Baselga, et al,2000;Herbst and Hong,2002;Robert, et al,2001;Shin, et al,2001).
In this study, immunohistochemical staining was performed on 57 cases of hypopharynx cancer to analyze the expression of EGFR. Overexpression of EGFR was noted in 63.2% of the cases. EGFR expression was significantly increased in the cases of advanced stage
tumors. Furthermore, in cases of overexpression of EGFR, rate of distant metastasis seemed to increase, and we believe that a statistically significant correlation may exist with a larger study population. From the fact that EGFR was more strongly expressed in the cancer cells, it is thought that EGFR activation is associated with the progression of cancer. In this study, even in the cases where EGFR expression was not observed, it is surmised that though EGFR were present, but could not be observed because it was too small of an amount in the paraffin embedded tissue to be immunohistochemically stained. Therefore, instead of using only immunohistochemical staining, further studies measuring the concentration of EGFR in the tissue or using Western blotting to determine the relationship between the concentration of EGF and EGFR, and their expression are warranted. Although there was no statistical significance between the expression of EGFR and the survival rate in this study, as the p-value was 0.053, it is believed that correlation may be confirmed by using a larger study population.
Degradation of ECM, which is a necessary step in tissue remodeling processes, such as wound healing and embryonal development has been attributed to proteolytic activity of MMPs. The role of EGF-R-mediated signals in regulating matrix degradation has not been completely unraveled. EGF-R inactivation has been shown to impair MMP activity during pancreatic and craniofacial development. Wound healing is another remodeling process, in which properly controlled stromal-epithelial interactions are crucial for outcome. In EGF-R null mice, early proliferation and migration of keratinocytes are impaired resulting in delayed wound healing. These article provide insight in the mode of action of EGFR in tissue remodeling processes(Kajanne, et al,2007). In this study, RT-PCR after EGF treatment for 24 and 48 hours revealed a marked increase in the level of 2 and MMP-9 in EGF treatment group. In addition, we confirmed by zymography that the activities of MMP-2 and MMP-9 were increased in the EGF treatment group as compared to the control group. These results suggest that exogenous EGF enhances the expression of MMP-2 and MMP-9 and the induction of MMP-2 and MMP-9 activities.
V. Conclusion
In summary, immunohistochemical staining of hypopharyngeal cancer tissue showed high expression of EGFR, and the level of EGFR significantly increased in relation to pathologic stage of the tumor. Moreover, the expression of protein of EGFR was increased in hypopharyngeal cancer cells compared to normal cells. Exogenous EGF significantly enhanced the growth and the invasiveness of cancer cells in a Transwell invasion chamber in a dose-dependent manner. MMP expression was detected in the hypopharyngeal cancer cells, and exogenous EGF enhanced the expression and its activity in the RT-PCR and zymogram analysis.
Through this study, we determined that the expression of EGFR was associated with tumor progression and prognosis of patients with hypopharyngeal cancer. Further research regarding the effect of EGF/EGFR on hypopharynx cancer performed with a larger study population will aid in the diagnosis and management of hypopharyngeal cancer.
REFERENCE
1. Arteaga C. Targeting HER1/EGFR: a molecular approach to cancer therapy.
Seminars in oncology. Jun;30(3 Suppl 7):3-14, 2003
2. Arteaga CL. The epidermal growth factor receptor: from mutant oncogene in nonhuman cancers to therapeutic target in human neoplasia. J Clin Oncol. Sep 15;19(18 Suppl):32S-40S, 2001
3. Baselga J. Targeting the epidermal growth factor receptor: a clinical reality. J Clin
Oncol. Sep 15;19(18 Suppl):41S-44S, 2001
4. Baselga J, Pfister D, Cooper MR, Cohen R, Burtness B, Bos M, D'Andrea G, Seidman A, Norton L, Gunnett K, Falcey J, Anderson V, Waksal H and Mendelsohn J. Phase I studies of anti-epidermal growth factor receptor chimeric antibody C225 alone and in combination with cisplatin. J Clin Oncol. Feb;18(4):904-914, 2000
5. Bonner JA, Harari PM, Giralt J, Azarnia N, Shin DM, Cohen RB, Jones CU, Sur R, Raben D, Jassem J, Ove R, Kies MS, Baselga J, Youssoufian H, Amellal N, Rowinsky EK and Ang KK. Radiotherapy plus cetuximab for squamous-cell carcinoma of the head and neck. The New England journal of medicine. Feb 9;354(6):567-578, 2006
6. Carpenter G and Cohen S. Epidermal growth factor. Annual review of
biochemistry.48:193-216, 1979
7. Chen P, Xie H, Sekar MC, Gupta K and Wells A. Epidermal growth factor receptor-mediated cell motility: phospholipase C activity is required, but mitogen-activated protein kinase activity is not sufficient for induced cell movement. The
8. Cheresh DA, Leng J and Klemke RL. Regulation of cell contraction and membrane ruffling by distinct signals in migratory cells. The Journal of cell biology. Sep 6;146(5):1107-1116, 1999
9. Ciardiello F, Caputo R, Bianco R, Damiano V, Pomatico G, De Placido S, Bianco AR and Tortora G. Antitumor effect and potentiation of cytotoxic drugs activity in human cancer cells by ZD-1839 (Iressa), an epidermal growth factor receptor-selective tyrosine kinase inhibitor. Clin Cancer Res. May;6(5):2053-2063, 2000 10. Cowley G, Smith J, Gusterson B, Hendler F and Ozanne B. The amount of EGF
receptor is elevated on squamous cell carcinoma. Cancer cells
Cold Spring Harbor Laboratory.5-10, 1984
11. Cowley GP, Smith JA and Gusterson BA. Increased EGF receptors on human squamous carcinoma cell lines. British journal of cancer. Feb;53(2):223-229, 1986
12. Davies RL, Grosse VA, Kucherlapati R and Bothwell M. Genetic analysis of epidermal growth factor action: assignment of human epidermal growth factor receptor gene to chromosome 7. Proceedings of the National Academy of Sciences
of the United States of America. Jul;77(7):4188-4192, 1980
13. Downward J, Yarden Y, Mayes E, Scrace G, Totty N, Stockwell P, Ullrich A, Schlessinger J and Waterfield MD. Close similarity of epidermal growth factor receptor and v-erb-B oncogene protein sequences. Nature. Feb 9-15;307(5951):521-527, 1984
14. Ekstrand AJ, James CD, Cavenee WK, Seliger B, Pettersson RF and Collins VP. Genes for epidermal growth factor receptor, transforming growth factor alpha, and
epidermal growth factor and their expression in human gliomas in vivo. Cancer
research. Apr 15;51(8):2164-2172, 1991
15. Etienne MC, Pivot X, Formento JL, Bensadoun RJ, Formento P, Dassonville O, Francoual M, Poissonnet G, Fontana X, Schneider M, Demard F and Milano G. A multifactorial approach including tumoural epidermal growth factor receptor, p53, thymidylate synthase and dihydropyrimidine dehydrogenase to predict treatment outcome in head and neck cancer patients receiving 5-fluorouracil. British journal
of cancer. Apr;79(11-12):1864-1869, 1999
16. Glading A, Chang P, Lauffenburger DA and Wells A. Epidermal growth factor receptor activation of calpain is required for fibroblast motility and occurs via an ERK/MAP kinase signaling pathway. The Journal of biological chemistry. Jan 28;275(4):2390-2398, 2000
17. Grandis JR and Tweardy DJ. Elevated levels of transforming growth factor alpha and epidermal growth factor receptor messenger RNA are early markers of carcinogenesis in head and neck cancer. Cancer research. Aug 1;53(15):3579-3584, 1993
18. Greenlee RT, Hill-Harmon MB, Murray T and Thun M. Cancer statistics, 2001.
CA: a cancer journal for clinicians. Jan-Feb;51(1):15-36, 2001
19. Gusterson B, Cowley G, McIlhinney J, Ozanne B, Fisher C and Reeves B. Evidence for increased epidermal growth factor receptors in human sarcomas.
International journal of cancer. Dec 15;36(6):689-693, 1985
20. Herbst RS and Hong WK. IMC-C225, an anti-epidermal growth factor receptor monoclonal antibody for treatment of head and neck cancer. Seminars in oncology. Oct;29(5 Suppl 14):18-30, 2002
21. Hirai T, Kuwahara M, Yoshida K, Kagawa Y, Hihara J, Yamashita Y and Toge T. Clinical results of transhiatal esophagectomy for carcinoma of the lower thoracic esophagus according to biological markers. Dis Esophagus. Oct;11(4):221-225, 1998
22. Kajanne R, Miettinen P, Mehlem A, Leivonen S-K, Birrer M, Foschi M, Kähäri V-M and Leppä S. EGF-R regulates V-MV-MP function in fibroblasts through V-MAPK and AP-1 pathways. Journal of Cellular Physiology. 2007
23. Klijn JG, Berns PM, Schmitz PI and Foekens JA. The clinical significance of epidermal growth factor receptor (EGF-R) in human breast cancer: a review on 5232 patients. Endocrine reviews. Feb;13(1):3-17, 1992
24. Kusukawa J, Harada H, Shima I, Sasaguri Y, Kameyama T and Morimatsu M. The significance of epidermal growth factor receptor and matrix metalloproteinase-3 in squamous cell carcinoma of the oral cavity. European journal of cancer. Jul;32B(4):217-221, 1996
25. Lemmon MA and Schlessinger J. Regulation of signal transduction and signal diversity by receptor oligomerization. Trends in biochemical sciences. Nov;19(11):459-463, 1994
26. LoRusso PM, Herbst RS, Rischin D, Ranson M, Calvert H, Raymond E, Kieback D, Kaye S, Gianni L, Harris A, Bjork T, Maddox AM, Rothenberg ML, Small EJ, Rubin EH, Feyereislova A, Heyes A, Averbuch SD, Ochs J and Baselga J. Improvements in quality of life and disease-related symptoms in phase I trials of the selective oral epidermal growth factor receptor tyrosine kinase inhibitor ZD1839 in non-small cell lung cancer and other solid tumors. Clin Cancer Res. Jun;9(6):2040-2048, 2003
27. Magne N, Fischel JL, Dubreuil A, Formento P, Ciccolini J, Formento JL, Tiffon C, Renee N, Marchetti S, Etienne MC and Milano G. ZD1839 (Iressa) modifies the activity of key enzymes linked to fluoropyrimidine activity: rational basis for a new combination therapy with capecitabine. Clin Cancer Res. Oct 15;9(13):4735-4742, 2003
28. Magne N, Fischel JL, Dubreuil A, Formento P, Marcie S, Lagrange JL and Milano G. Sequence-dependent effects of ZD1839 ('Iressa') in combination with cytotoxic treatment in human head and neck cancer. British journal of cancer. Mar 4;86(5):819-827, 2002
29. Magne N, Fischel JL, Dubreuil A, Formento P, Poupon MF, Laurent-Puig P and Milano G. Influence of epidermal growth factor receptor (EGFR), p53 and intrinsic MAP kinase pathway status of tumour cells on the antiproliferative effect of ZD1839 ("Iressa"). British journal of cancer. May 6;86(9):1518-1523, 2002 30. Magne N, Fischel JL, Tiffon C, Formento P, Dubreuil A, Renee N, Formento JL,
Francoual M, Ciccolini J, Etienne MC and Milano G. Molecular mechanisms underlying the interaction between ZD1839 ('Iressa') and cisplatin/5-fluorouracil.
British journal of cancer. Aug 4;89(3):585-592, 2003
31. Miyaguchi M, Olofsson J and Hellquist HB. Expression of epidermal growth factor receptor in glottic carcinoma and its relation to recurrence after radiotherapy.
Clinical otolaryngology and allied sciences. Oct;16(5):466-469, 1991
32. Ono M and Kuwano M. Molecular mechanisms of epidermal growth factor receptor (EGFR) activation and response to gefitinib and other EGFR-targeting drugs. Clin
33. Prenzel N, Fischer OM, Streit S, Hart S and Ullrich A. The epidermal growth factor receptor family as a central element for cellular signal transduction and diversification. Endocrine-related cancer. Mar;8(1):11-31, 2001
34. Putti TC, To KF, Hsu HC, Chan AT, Lai GM, Tse G, Lee YS, Whang-Peng J, Millward M, Lin L, Lin X and Lee CS. Expression of epidermal growth factor receptor in head and neck cancers correlates with clinical progression: a multicentre immunohistochemical study in the Asia-Pacific region. Histopathology. Aug;41(2):144-151, 2002
35. Robert F, Ezekiel MP, Spencer SA, Meredith RF, Bonner JA, Khazaeli MB, Saleh MN, Carey D, LoBuglio AF, Wheeler RH, Cooper MR and Waksal HW. Phase I study of anti--epidermal growth factor receptor antibody cetuximab in combination with radiation therapy in patients with advanced head and neck cancer. J Clin
Oncol. Jul 1;19(13):3234-3243, 2001
36. Rubin Grandis J, Melhem MF, Gooding WE, Day R, Holst VA, Wagener MM, Drenning SD and Tweardy DJ. Levels of TGF-alpha and EGFR protein in head and neck squamous cell carcinoma and patient survival. J Natl Cancer Inst. Jun 3;90(11):824-832, 1998
37. Rusch V, Baselga J, Cordon-Cardo C, Orazem J, Zaman M, Hoda S, McIntosh J, Kurie J and Dmitrovsky E. Differential expression of the epidermal growth factor receptor and its ligands in primary non-small cell lung cancers and adjacent benign lung. Cancer research. May 15;53(10 Suppl):2379-2385, 1993
38. Salomon DS, Brandt R, Ciardiello F and Normanno N. Epidermal growth factor-related peptides and their receptors in human malignancies. Critical reviews in
39. Shin DM, Donato NJ, Perez-Soler R, Shin HJ, Wu JY, Zhang P, Lawhorn K, Khuri FR, Glisson BS, Myers J, Clayman G, Pfister D, Falcey J, Waksal H, Mendelsohn J and Hong WK. Epidermal growth factor receptor-targeted therapy with C225 and cisplatin in patients with head and neck cancer. Clin Cancer Res. May;7(5):1204-1213, 2001
40. Smith BD, Smith GL, Carter D, DiGiovanna MP, Kasowitz KM, Sasaki CT and Haffty BG. Molecular marker expression in oral and oropharyngeal squamous cell carcinoma. Archives of otolaryngology--head & neck surgery. Jul;127(7):780-785, 2001
41. Soulieres D, Senzer NN, Vokes EE, Hidalgo M, Agarwala SS and Siu LL. Multicenter phase II study of erlotinib, an oral epidermal growth factor receptor tyrosine kinase inhibitor, in patients with recurrent or metastatic squamous cell cancer of the head and neck. J Clin Oncol. Jan 1;22(1):77-85, 2004
42. Tateishi M, Ishida T, Mitsudomi T, Kaneko S and Sugimachi K. Immunohistochemical evidence of autocrine growth factors in adenocarcinoma of the human lung. Cancer research. Nov 1;50(21):7077-7080, 1990
43. Xie H, Pallero MA, Gupta K, Chang P, Ware MF, Witke W, Kwiatkowski DJ, Lauffenburger DA, Murphy-Ullrich JE and Wells A. EGF receptor regulation of cell motility: EGF induces disassembly of focal adhesions independently of the motility-associated PLCgamma signaling pathway. Journal of cell science. Mar;111 ( Pt 5):615-624, 1998
44. Yamanaka Y, Friess H, Kobrin MS, Buchler M, Beger HG and Korc M. Coexpression of epidermal growth factor receptor and ligands in human pancreatic cancer is associated with enhanced tumor aggressiveness. Anticancer research. May-Jun;13(3):565-569, 1993
45. Yarden Y and Sliwkowski MX. Untangling the ErbB signalling network. Nature
reviews. Feb;2(2):127-137, 2001
46. Yonemura Y, Takamura H, Ninomiya I, Fushida S, Tsugawa K, Kaji M, Nakai Y, Ohoyama S, Yamaguchi A and Miyazaki I. Interrelationship between transforming growth factor-alpha and epidermal growth factor receptor in advanced gastric cancer. Oncology.49(2):157-161, 1992
47. Zimmermann M, Zouhair A, Azria D and Ozsahin M. The epidermal growth factor receptor (EGFR) in head and neck cancer: its role and treatment implications.
-국문요약-
하인두암에서의
하인두암에서의
하인두암에서의
하인두암에서의 표피성장인자
표피성장인자
표피성장인자
표피성장인자 수용체
수용체
수용체
수용체(Epidermal Growth Factor
Receptor)의
의
의
의 발현과
발현과
발현과
발현과 하인두암의
하인두암의
하인두암의
하인두암의 진행에
진행에
진행에 있어서
진행에
있어서
있어서
있어서
표피성장인자
표피성장인자
표피성장인자
표피성장인자(Epidermal Growth Factor)의
의
의 영향
의
영향
영향
영향
아주대학교 대학원의학과 김 윤 태 (지도교수: 김 철 호) 배경 배경 배경배경 및및및및 목적목적목적목적: Epidermal growth factor receptor (EGFR)는 ErbB family 중의 하나로 발현율이 증가한 경우 두경부 편평세포암(HNSCC)에서 불량한 방사선 치료 반응과 나쁜 예후와 연관성이 있다고 알려져 있다. EGFR 은 tyrosine kinase
inhibitor 등을 포함해서 두경부 편평세포암의 새로운 치료 방법으로 각광 받고 있다. 따라서 본 저널은 하인두암조직에서의 EGFR 의 발현과 암의 진행에 있어서의 EGF 의 영향에 대해서 하인두세포주를 가지고 연구하고자 하였다. 재료 재료 재료 재료 및및및및 방법방법방법방법: 두경부 편평세포암 중에서 하인두암으로 진단 받은 57 명의 환자에서 얻은 정상 조직과 암조직을 EGFR Antibody 를 가지고 면역조직화학적 염색을 시행하였다. 세명의 환자에게서 얻은 정상과 암조직을 이용해서 Western
blot 을 시행하였고 하인두암 세포주인 FaDu cell 을 가지고 역전사 중합효소
연쇄반응(RT-PCR) 및 Western blot 을 시행하였다. EGF 의 농도에 따른(0, 10, 30
ng/㎖) FaDu cell 의 증식을 알기 위해 Haemocytometer 를 이용하여 세포수를
비교하였다. EGF 농도에 따른(0, 10, 30 ng/㎖) 분산을 사진을 통해 비교하였고,
Membrane invasion assay 를 통해 침입성(invasiveness)을 측정하였다. FaDu cell 을
가지고 EGF 와 MMP 의 관계와 MMP-2 와 MMP-9 의 역할을 알아 보고자 역전사 중합효소 연쇄반응(RT-PCR) 와 zymography 을 시행하였다.
결과 결과 결과 결과: 하인두암조직에서 EGFR 의 면역 조직화학적 염색의 양성 발현율은 63.2%이었으며 조직학적 병기와 유의미한 연관이 관찰되었고, Western blot 을 통해 EGFR 의 증가된 발현이 확인 되었다. 하인두암 세포주에서 EGFR
mRNA(RT-PCR)와 protein(Western blot)의 증가된 발현이 확인되었다. EGF 의
농도에 따라(0, 10, 30 ng/㎖) FaDu cell 의 증식과 침습이 유의미하게 증가되는 양상을 보였다. FaDu cell 에서 MMP 의 발현이 확인되었으며, EGF 의 농도에 따라 발현이 증가되었다.
결론 결론 결론
결론: EGF 는 하인두암의 진행에 있어서 중요한 역할을 할 거라 생각된다.
핵심어: EGF, EGFR, hypopharyngeal cancer, matrix metalloproteinase, proliferation,