한국응급구조학회지 제 25 권 제 1 호, 243 ~ 249 (2021. 04) Korean J Emerg Med Ser Vol. 25, No. 1, 243 ~ 249 (2021. 04) The Korean Journal of Emergency Medical Services
ISSN 1738-1606 (Print) ISSN 2384-2091 (Online) https://doi.org/10.14408/KJEMS.2021.25.1.243
병원 전 12-Lead ECG 측정을 통해 진단된 이형성 협심증 1례
김지원
1,3·기은영
2* 1단국대학교 대학원 의학과
2서정대학교 응급구조과
3대한응급의료종사자 교육연구회
Variant angina diagnosed on pre-hospital 12-lead
electrocardiogram: A case report
Ji-Won Kim
1,3·Eunyoung Ki
2*1
Department of Medicine, Graduate school, Dankook University
2Department of Emergency Medical Service, Seojeong University
3
Korea Paramedic Education Research Society
=Abstract =
A decrease in coronary blood flow leads to an imbalance between the supply of oxygen to the myocardium and its demand, and reversible or irreversible damage to the myocardium could occur depending on the severity of the resultant ischemia and the duration of the imbalance. This imbalance results in a cascade of ischemic reactions in the following order: metabolic abnormalities, diastolic dysfunction, systolic dysfunction, and electrocardiogram changes. Variant angina is caused by the closure of the coronary artery due to reversible coronary artery spasm, resulting in myocardial ischemia and subsequent chest pain as a clinical symptom. Variant angina may be observed as ST segment elevation in electrocardiogram measured when present in chest pain. However, 12-lead electrocardiogram performed after the patient's chest pain resolves does not help in the diagnosis. Since the duration of chest pain appears to be <15 minutes, it is important to perform the 12-lead electrocardiogram when clinical symptoms are present. If nitroglycerin is administered without performing 12-lead electrocardiogram by 119 pre-hospital paramedics, the chest pain would be resolved, making it
Received February 18, 2021 Revised March 28, 2021 Accepted April 20, 2021 *Correspondence to Eunyoung Ki
Department of Emergency Medical Service, Seojeong University, 27, Seojeong-ro, Eunhyeon-myeon, Yangju, Gyeonggi-do, 11429, Republic of Korea
244
impossible to identify changes in the ST segment. Before administration of nitroglycerin, changes in the ST segment must be recorded by performing 12-lead electrocardiogram.
Keywords: Chest pain, Variant angina pectoris, Electrocardiogram(ECG), Paramedic, ST segment elevation
Ⅰ. 서 론
급성관상동맥증후군은 12유도 심전도 측정 결과에 ST분절 상승과 비ST분절 상승 급성관상 동맥질환증후군으로 분류할 수 있으며, 가역적 인 관상동맥 연축(coronary artery spasm)으로 인해 관상동맥 폐쇄 및 심근허혈이 발생하는 이 형성 협심증(variant angina)을 포함한다. 급성 관상동맥증후군에서 12유도 심전도는 초기치료 를 결정하는데 있어서 중요한 역할을 한다[1, 2]. 이형성 협심증은 휴식 중 발생하는 흉통과 심전도의 ST분절 상승(ST segment elevation) 을 동반하는 관상동맥질환으로 흉통 및 부정맥 에서 심인성 급사까지도 발생 가능한 것으로 알 려져 있다. 이형성 협심증은 흉통을 동반되었을 때 측정한 심전도에서 ST분절 상승을 관찰될 수 있지만, 환자의 흉통이 사라진 후 측정한 12유 도 심전도(12-lead electrocardiogram, 12-lead ECG)는 진단에 도움이 되지 못한다[3, 4]. 이러 한 이형성 협심증의 허혈성 흉통 증상은 15분 이내[5]로 지속되다 소실을 보이며 초기 증상 발생 후 병원을 방문할 때까지 걸리는 시간에 따라 증상이 호전을 보일 수 있어, 병원에 내원 후 측정한 심전도에서는 ST분절의 상승 관찰이 어렵다. 이에 무엇보다 임상 증상(clinical symptom)이 존재할 때 12-lead ECG를 측정하 는 것이 이형성 협심증 진단에 있어 매우 중요 하다. 이러한 중요성에도 불구하고 관상동맥질 환이 의심되는 흉통 환자에서 현장 119구급대 원이 12-lead ECG 측정하는 것은 무면허의료행 위 및 업무 범위 제한으로 허용되지 않았다. 하 지만 2019년 9월부터 119특별구급대를 시범적 으로 운영하면서 현장 구급대원이 흉통환자의 12-lead ECG 측정이 가능해졌다. 이에 병원 전 단계에서 119구급대원이 측정한 12-lead ECG 를 통해 이형성 협심증을 진단할 수 있었던 1례 를 보고하는 바이다.
Ⅱ.
증 례
• 환자 : 김OO, 남자, 65세 • 주소 : 내원일 아침 09시경 TV 시청 중 조이 는 양상의 흉통으로 119 신고하여, 구급차를 통해 09시 24분에 본원으로 내원하였다. • 현병력 : 이형협심증 의증, 심방세동, 당뇨, 고혈압으로 경구약 복용하고 있다. • 과거력 및 사회력 : 07년도 흉통으로 인해 측정한 12-lead ECG에서 흉부유도 V1~4까 지의 biphasic T wave inversion 소견이 관찰 되어 wellen’s syndrome type A로<Fig. 1> 관 상동맥조영술(coronary angiography, CAG) 을 시행하여 좌전하행지 근위부(proximal left anterior descending, p-LAD) stent 삽입 술을 시행하였다. • 신체검사 소견 : 내원 당시 혈압은 141/100 mmHg, 심박수는 83회/min, 호흡수는 24 회/min, 체온은 36.5℃였으며 의식은 명료 하였다. 흉통과 발한(sweating)이 있었으 며, 방사통(radiation pain)은 없었다. • 심전도 소견 : 119구급대가 환자와 접촉하 여 측정한 12-lead ECG에서 심방세동Fig. 1. Electrocardiogram measured in 2007. A biphasic T wave inversion is showed from precordial lead V1 to 4.
(atrial fibrillation)의 리듬과 전흉부유도 및 사지유도 II, III, aVF에서 ST분절 상승 이 관찰되어 ST분절 상승 심근경색(ST elevation myocardial infarction)을 의심할 수 있었다<Fig. 2>. 이후 증상은 호전된 상 태로 본원 응급실 내원하였으며, 내원하여 측정한 12-lead ECG에서 빠른심실반응의 심방세동(atrial fibrillation with rapid ventricular response) 리듬을 보였고, 이전 관찰된 ST분절 상승은 모두 정상화된 소견 을 보였다<Fig. 3>.
• 심초음파 소견 : 내원하여 시행한 심초음 파에서 국소벽운동장애(regional wall mo-tion abnormality)의 모습은 관찰되지 않았 고, 심초음파 관찰 중 흉통은 존재하지 않 았다. • 혈액 검사 소견 : Troponin T는 0.007 ng/mL, CK 73 ng/mL, CK-MB 2.82 g/mL 로 모두 정상범주 내로 나타났다. • 방사선 소견 : 내원 시 흉부 방사선에서는 특이 소견이 발견되지 않았다. • 치료 및 임상경과 : 심장혈관내과로 입원 하여 이틀 후 CAG를 시행하였다. 검사에 과거 시행한 p-LAD에 stent의 55% 정도의 협착이 관찰되었다<Fig. 4>.
Ⅲ.
고 찰
관상동맥 혈류량의 감소는 심근으로의 산소 공급과 수요의 불균형이 초래되고 허혈의 심각 도와 불균형의 지속시간에 따라 심근의 가역적 또는 비가역적 손상이 발생하게 된다. 공급과 수요 불균형으로 인한 허혈성 반응은 대사이상, 이완장애(diastolic dysfunction), 수축장애 (systolic dysfunction), 심전도 변화를 거쳐 임 상 증상 발현 순으로 허혈 연쇄 반응(ischemic cascade) 과정을 보인다[6]. 협심증과 이형성 협심증은 관상동맥 관류량이 감소하여 발생하 는 공통점을 갖는다. 하지만 협심증은 동맥경화 로 혈관 내경(lumen)이 좁아지는 것에 기인하246
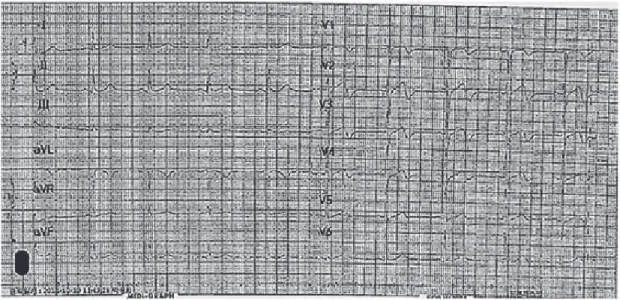
Fig. 2. 12 Lead ECG measurements taken at pre-hospital: lead precordial, II, III, aVF of ST segment elevation are shown.
Fig. 3. Initial electrocardiography in hospital showed atrial fibrillation with rapid ventricular response rhythm and disappeared ST segment elevation.
Fig. 4. Coronary angiography. a) right coronary artery b) left coronary artery. 며, 이형성 협심증은 관상동맥 연축(coronary artery spasm)으로 인해 발생하는 것으로 알려 져 있다. 이형성 협심증 특징에는 1) 운동이나 정서적 흥분과 같은 심근 산소 요구량 증가와 관련 없는 가슴 통증의 발생, 2) 심야 또는 이 른 아침에 발생하는 흉통, 3) 흉통과 함께 심전 도에서 ST분절 상승 관찰 등이 있다[2, 7]. 국 내 119구급대 신고 후 구급대원이 환자를 접촉 까지 6분, 이송시간은 9분 정도로 총 이송시간 은 15분 정도 소요되며[8]. 이형성 협심증의 흉 통 지속시간을 고려해 볼 때 구급차를 이용하 여 환자를 이송 후 병원 내에서 ST분절의 상승 을 관찰하는 것은 어렵다. 본 증례의 환자는 아 침 휴식 중에 발생한 흉통으로 119에 신고 후 구급대원이 심전도를 측정하여 사지유도 II, III, aVF와 전흉부유도에서 ST분절 상승 심근경색 의 소견을 확인하였으며, 내원하여 흉통 소실 과 함께 측정한 심전도에서 ST분절의 상승소견 은 확인되지 않았다. 환자는 병원 내원 중에 증 상이 호전되면서 구급대원의 측정된 심전도 기 록을 통해 ST분절 변화를 확인하여 이형성 협 심증을 진단할 수 있었다. 선행연구에 따르면, 미국심장학회(American Heart Association)는 심근경색증 환자가 발생 한 경우 증상이 시작되고 나서 8분 이내에 응 급의료종사자가 현장에 도착하여 병원 도착 전 12-lead ECG를 시행하고, 체크리스트를 확인 후 현장 도착 30분 이내 투약 가능하다면, 현장 처치로서 병원 도착 전에 혈전용해제를 투여하 는 것을 권고하고 있다[9]. 그러나 국내는 아직 현장 구급대원이 12-lead ECG를 측정하는 것 마저 시범적으로 일부 구급대원에 한하여 시행 하도록 하고 있다. 허혈 연쇄 반응을 고려할 때 이전 119구급대원의 12-lead ECG 측정이 불가 능한 제도적 상황에서 12-lead ECG 측정 하지 않고 표준지침에 따라 니트로글리세린을 투여 하는 것은 통증을 경감시켜 ST분절의 변화를 기록할 수 없게 만든다. 니트로글리세린을 투여 하기 전 반드시 12-lead ECG를 측정하여 ST분 절의 변화를 기록해야 한다.
248
Ⅳ.
결 론
급성관상동맥증후군이 의심되는 흉통 환자 에서 현장 119구급대원이 12-lead ECG 측정으 로 ST분절 상승을 확인하여 이형성 협심증을 진단할 수 있었던 증례로, 출동한 119구급대원 이 흉통환자에 있어 12-lead ECG 측정의 필요 성과 진단적 가치가 있음을 확인할 수 있는 좋 은 예이다. 119구급대원이 현장에서 12-lead ECG 측정하는 것이 환자의 진단과 치료에 긍 정적인 영향을 줄 것으로 예측할 수 있으며, 119 특별구급대 시범사업이 궁극적으로 환자에 게 도움이 되었다는 것을 알 수 있었다. 지속적 인 연구를 통해 병원 전 단계의 12-lead ECG 측정의 효과를 입증한다면, 병원 전 단계의 급 성관상동맥증후군의 환자를 보다 빠르게 처치 할 수 있는 기초자료가 될 수 있을 것이다. 또 한 응급구조사 업무범위 확대에 따른 효과에 관한 연구가 활발히 이뤄져 효과가 입증됨을 통해 업무 범위를 확대하는 기초자료가 될 수 있을 것이다.ORCID ID
Ji-Won Kim : 주저자 0000-0003-2423-5499 Eunyoung Ki : 교신저자 0000-0003-2088-2488References
1. Jeon DS. Diagnosis and management of acute
cor-onary syndrome. J Korean Med Assoc 2017:60(7):568-76.
https://doi.org/10.5124/jkma.2017.60.7.568 2. Kusama Y, Kodani E, Nakagomi A, Otsuka T,
Atarashi H, Kishida H et al. Variant angina and coronary artery spasm: the clinical spectrum, pathophysiology, and management. J Nippon Med Sch 2011;78(1):4-12.
https://doi.org/10.1272/jnms.78.4
3. Kang JA, Lee YS, Jeong SH, Lee JW, Kim BY, Im DS, Seong IW. Clinical characteristics of pa-tients with variant angina. Korean J Med 2002;63(2):195-202.
4. Hung MJ, Cheng CW, Yang NI, Hung MY, Cherng WJ. Coronary vasospasm-induced acute coronary syndrome complicated bylife-threat-ening cardiac arrhythmias in patients without hemodynamically significant coronary artery disease. Int J Cardiol 2007;117:37-44. https://doi.org/10.1016/j.ijcard.2006.03.055 5. Cho JR. Differential diagnosis of chest pain.
Korean J Med 2017;(2):201-4.
6. Renker M, Baumann S, Rier J, Ebersberger U, Fuller SR, Batalis NI et al. Imaging coronary artery disease and the myocardial ischemic cas-cade: clinical principles and scope. Radiologic Clinics North Am 2015;53(2):261-9.
https://doi.org/10.1016/j.rcl.2014.11.010 7. Song JK. Coronary artery vasospasm. Korean
Circ J 2018;48(9):767-77.
https://doi.org/10.4070/kcj.2018.0251
8. Hong KH, Lee KJ, Kim JT, Lee DH. Severity-based analysis of prehospital transportation time using the geographic information system (GIS). J Korean Soc Emerg Med 2008;19(2):153-60. 9. American Heart Association. 2005 American
car-diopulmonary resuscitation (CPR) and emer-gency cardiovascular care (ECC) of pediatric and neonatal patients: pediatric advanced life
support. Pediatrics 2006;117(5):e1005-e1028. https://doi.org/10.1542/peds.2006-0346