서론
급성부비동염은 코와 부비동 점막에 발생하는 염증을 말 한다. 주요 증상은 발열, 화농성 콧물, 안면통증 등이며, 이들 증상은 2주까지도 지속될 수 있다. 급성부비동염은 연령에 따른 발생빈도에 차이가 있는데, 6-35개월 연령의 어린 영 아는 바이러스로 인한 상기도 감염이 1년에 6회 이상 발생 한다[1]. 선행하는 바이러스 감염 후 2차적인 세균성 감염은 소아의 5-9%로 추정된다[2,3]. 한편 급성부비동염 중 세균 감염으로 인한 경우는 약 2-10%, 바이러스는 90-98%이나 [2], 소아에서 질환별 항생제 처방률에 대한 조사에서 부비 동염 진단 하에 항생제를 처방 받는 경우가 88.8%로 보고되 었다[4]. 이와 같이 임상적으로 바이러스와 세균으로 인한 경 우를 구분하기 어려운 경우가 많으나, 급성세균성부비동염 을 잘 진단하고 항생제를 적절하게 사용하는 것이 중요하다. 국내 소아 급성상기도감염의 항생제 사용지침이 2016년 에 발표되었다[5]. 질병관리본부 정책연구용역사업으로 항소아 급성부비동염의 진단과 치료
이 현 주 | 서울대학교 의과대학 분당서울대학교병원 소아청소년과Diagnosis and treatment of acute rhinosinusitis in
children
Hyunju Lee, MD
Department of Pediatrics, Seoul National University Bundang Hospital, Seoul National University College of Medicine, Seongnam, Korea
Received: January 1, 2018 Accepted: January 15, 2018 Corresponding author: Hyunju Lee
E-mail: hyunjulee@snu.ac.kr © Korean Medical Association
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons. org/licenses/by-nc/3.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Acute rhinosinusitis is a common entity in children, most are due to viral infections, however up to over 80% children with rhinosinusitis are prescribed with antibiotics. Acute bacterial sinusitis should be diagnosed in when a child has 1) a severe onset with a fever over 39℃, purulent nasal discharge or facial pain for 3 to 4 days; 2) persistent illness with rhinorrhea, daytime cough or both for over 10 days with no clinical improvement; or 3) worsening course with symptoms aggravating or new onset symptoms including fever, headache, cough or rhinorrhea after clinical improvement. Radiographic imaging is not recommended for differentiation of viral and bacterial rhinosinusitis, however a contrast-enhanced computed tomography or magnetic resonance imaging may be done in cases with orbital or central nervous system complications. Antibiotics may be prescribed in cases with severe onset or worsening course. Antibiotics may be prescribed after additional observation for 3 days in children with persistent illness. Amoxicillin-clavulanate (amoxicillin 40 to 50 mg/kg/day, every 12 hours) is recommended for initial treatment and high dose amoxicillin-clavulanate (amoxicillin 90 mg/kg/day every 12 hours) may be considered in cases with severe infection, children in day care center, under 2 years of age, recent admission history, previous antibiotics within 1 month and immunocompromised children. Clinical response should be reassessed in cases of worsening or failure to improve within 72 hours of treatment.
생제 사용지침 개발위원회를 중심으로 진행되었으며, 8개 이상 전문가단체로부터 자문을 받아 개발되었다. 본 논문에 서는 국내 소아 급성상기도감염의 항생제 사용지침을 중심 으로 국내 소아의 급성부비동염의 원인, 진단 및 치료에 대 해 소개하고자 한다.
급성부비동염의 원인
급성부비동염의 원인은 다양하며, 여러 알레르기 항원, 환 경 자극 그리고 바이러스, 세균, 진균을 포함한 감염에 의해 발생할 수 있으며, 그 중 바이러스 감염으로 인한 경우가 가 장 흔하다. 바이러스 감염 중에서도 rhinovirus, influenza virus, parainfluenza가 대표적이며 그 밖에 다른 호흡기 바 이러스도 급성부비동염을 일으킬 수 있다[6]. 소아에서 급성세균성부비동염의 원인은 과거 소아 환자를 대상으로 시행한 부비동 천자액 배양을 통해 처음 밝혀졌으 며, 당시 Streptococcus pneumoniae가 약 30%, 비피막형Haemophilus influenzae와 Moraxella catarrhalis가 각각 20%이었으며, 약 25-30%는 균이 분리되지 않았다[7,8]. 그 러나 부비동 천자술은 침습적인 검사로 잘 시행되지 않고 있 으며, 급성부비동염의 원인은 중이염과 유사한 것으로 알려져 있어 중이염 환자에서 분리된 원인균 및 항생제 감수성 결과 를 참고한다[9]. 7가 폐구균 단백결합백신 및 최근 10가, 13가 폐구균 단백결합백신 도입 이후 소아 중이염 환자들에서 S. pneumoniae가 감소하였으며, 상대적으로 H. influenzae가 증가한 것으로 보고되었다[10]. 그리하여 최근 분포를 보면, 가장 흔한 원인균에는 변화는 없지만, S. pneumoniae와 H. influenzae는 소아에서 급성세균성부비동염의 약 30%, M. catarrhalis가 약 10%를 차지할 것으로 추정된다[11]. 항생제 감수성 변화는 지역에 따라 달라 지역사회 내 항 생제 내성률을 아는 것이 중요하다. 국내 중이에서 분리된 균주의 항생제 감수성 결과에 대한 보고는 제한적이나, 소 아에서 비인두 집락된 균의 항생제 내성률을 보면 도움이 된다. 2014년 어린이집에 다니는 소아를 대상으로 비인두 에 집락된 S. pneumoniae 중 23%가 penicillin에 비감수성 이었으며, 15%가 cefotaxime, 90.4%가 erythromycin에 비감수성이었다[5,12]. 2014년 급성호흡기감염으로 국내 단일 기관에 방문한 소아에서 비인두 집락된 비피막형 H. influenzae에 대한 항생제 감수성 분석 결과, 항생제별 내 성률은 ampicillin 83%, cefaclor 81% 그리고 cefuroxime 77.4%로 보고되었다[5].
급성세균성부비동염의 진단
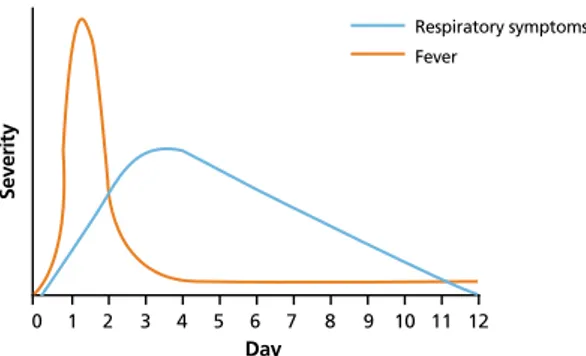
급성세균성부비동염은 부비동 천자액에서 세균이 ≥104 CFU/mL 분리될 때 진단할 수 있다[13]. 그러나 부비동 에서 천자액을 얻는 것은 침습적인 시술일 뿐 아니라 채취과 정에서 집락균의 오염이 있을 수 있으며, 검체 확보가 어려우 므로 임상적으로 적용하기 어렵다. 이와 같이 급성부비동염은 주로 임상증상 및 영상의학검사를 이용하여 진단하게 된다. 그러나 이러한 방법도 세균과 바이러스 감염을 구분하는데 제 한이 있다. 급성세균성부비동염을 진단하기 위해서 바이러스로 인 한 상기도감염증의 자연경과를 이해하는 것이 중요하다. 바이러스 감염 시 콧물, 코막힘, 기침이 동반되고 목이 간 질간질한 증상이 동반될 수 있다. 대개 분비물은 처음에 맑 고 흐르는 양상이나, 점차 화농성, 점액성으로 바뀌고, 시 간이 지나면 항생제 치료 없이도 분비물은 자연스럽게 다 시 맑아지고 양이 줄면서 호전된다. 발열이 항상 있는 것 은 아니나, 발열이 나타나면 초기에 두통, 근육통 등과 같 은 전신증상과 동반되기도 한다. 일반적으로 발열과 전신 증상은 24-48시간 내 호전을 보이고, 호흡기증상은 수일 에 걸쳐 점차 진행하다가 5-10일 내 점차 호전을 보인다 (Figure 1) [11,14]. 바이러스 상기도감염의 자연경과와 다른 경과를 보일 때 세 균감염을 의심할 수 있는데, 다음 3가지 중 최소 한가지 이상 에 해당될 때 급성세균성부비동염을 의심할 수 있다[5]. 1) 심 한 발병으로서 발병 당시 심한 증상 또는 39℃ 이상의 발열과 화농성 콧물이나 안면 통증이 최소 3-4일 연속으로 나타나는 경우; 2) 지속적인 증상으로서 콧물, 낮시간의 기침 또는 두증상 모두 10일 이상 지속되면서 임상적으로 호전을 보이지 않는 경우; 3) 악화되는 경과로서 증상들이 더욱 악화되거나 초기에 보였던 전형적인 바이러스 상기도 감염 증상들이 5- 6일 지속되다 호전 추세를 보이던 중 새로 발병되는 발열, 두 통, 기침 또는 콧물 시 의심한다. 다만, 이 경우 환자의 증상이 처음과 다른 바이러스로 인한 2차 감염인지를 감별하는 것이 중요하며, 또한 알레르기비염이 있는 환자의 경우 기저질환으 로 인해 증상이 오래 지속될 수 있어 이전 알레르기 병력(습 진, 아토피피부염, 천식, 알레르기결막염) 및 코와 눈의 가려 움과 같은 동반증상 여부를 함께 평가하여야 한다[11]. 단순 급성세균성부비동염의 진단을 목적으로 방사선촬영 을 하는 것은 권장되지 않는다[5]. Kovatch 등[15]은 바이러 스 감염이 의심되는 소아에게 방사선촬영검사 결과, 절반 이 상에서 상악동에 비정상적 소견을 보인다고 하였으며, 반대 로 증상이 없는 건강한 아이들에서 비정상적인 영상 소견이 발견되기도 하였다[16,17]. 그 밖에도 Kristo 등[18]과 Kristo 등[19]은 자기공명영상촬영에서 급성호흡기감염증이 있는 아 이들의 68%, 그리고 건강한 학동기 연령(8-9세) 아이들의 42%가 부비동에 비정상 소견이 발견 된다고 하였다. 이와 같 이 영상검사는 바이러스와 세균성 부비동염을 구분하지 못 하며, 부비동이 정상인 경우 급성세균성부비동염의 가능성 이 낮지만, 영상검사에서 비정상적인 소견을 보인다고 세균 성 부비동염을 진단하지 못한다. 또한 건강한 사람에서도 비 정상적인 영상 소견을 보일 수 있어 급성세균성부비동염 배 제 목적으로 영상검사를 하는 것도 추천되지 않는다. 그러나 급성세균성부비동염으로 인한 안와 또는 중추신경 계의 합병증이 의심되는 경우 조영증강 부비동 컴퓨터단층 촬영 또는 자기공명영상촬영을 하는 것이 추천된다[5]. 급성 세균성부비동염에서 화농성 합병증이 드물어 소아 부비동염 입원환자의 약 3.7-11%에서 보고되었으며, 대부분 안와 봉 와직염 및 중추신경계 감염인 것으로 보고되었다[20].
치료
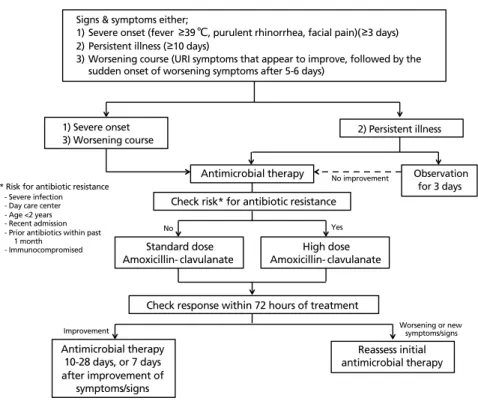
급성세균성부비동염으로 진단한 경우, 심한 발병 또는 악 화되는 경과를 보인다면 항생제 처방이 추천된다[5]. 지속되 는 증상을 보이면서 호전되지 않는다면 항생제 처방을 하거 나 3일 동안 외래에서 항생제 없이 경과 관찰할 수 있다[5]. 항생제 사용 없이 관찰하는 것은 일부 아이들에게서 자연호 전을 기대할 수 있고, 화농성 합병증의 발생 빈도가 낮으며, 지속되는 증상들이 가벼워서 대부분 삶의 질에 영향을 크게 미치지 않기 때문이다[5,11]. 또한 불필요한 항생제는 항생제 로 인한 부작용, 즉, 설사, 발진 등을 유발할 수 있으며 관찰 후 항생제 사용을 고려할 수 있다. 급성세균성부비동염 항생제 선택 시 주요 원인균주의 항생 제 감수성 패턴 및 내성 기전을 이해하는 것이 중요하다. S. pneumoniae 내성은 페니실린 결합 단백의 변이에 의하며, H. influenzae는 페니실린 결합 단백의 변이 및 β-lactamase 생성, M. catarrhalis는 β-lactamase 생성에 기인한다. 항생 제 내성을 보이는 경우 감수성 있는 항생제로 변경하는 것 이 일반적이나, S. pneumoniae에 대한 약동학적 연구를 바 탕으로 고용량 amoxicillin이 가장 좋은 반응을 보였으며, 일 부 페니실린 결합 단백 변이를 보이면서 β-lactamase 생성 하지 않은 H. influenzae에서도 좋은 결과를 보였다[21]. 이 때문에 S. pneumoniae 및 일부 H. influenzae로 인한 급성세 균성부비동염 치료 시 고용량 amoxicillin이 가장 효과가 좋 으며, β-lactamase 생성H. influenzae와 M. catarrhalis 은 β-lactamase 억제제인 clavulanate가 부착된 항생제를 사용 하는 것이 효과적이다[11].급성세균성부비동염에 항생제 치료 시, 1차 선택약제로 표 준 용량의 amoxicillin-clavulanate(경구 amoxicillin 40- 50 mg/kg/day, 12시간마다)가 추천된다(Figure 2) [5]. 대
Figure 1. Natural course of uncomplicated viral upper respiratory tract
infection. Reproduced from Wald ER, et al. Pediatrics 2013;132:e262-e280, according to the Creative Commons license [11].
0 1 2 3 4 5 6 7 8 9 10 11 12
Day
Severity
Respiratory symptoms Fever
체로 amoxicillin 단독요법보다 amoxicillin-clavulanate 요 법이 추천된다. 심한 감염(39℃ 이상의 발열과 화농성 합병증의 위험이 있 는 경우), 어린이집에 다니는 경우, 2세 미만, 최근에 입원한 병력, 최근 1개월 이내에 항생제 사용력이 있는 경우, 면역 저 하자에 해당되는 경우는 고용량의 amoxicillin-clavulanate (경구 amoxicillin 90 mg/kg/day, 12시간마다)를 추천한다 (Figure 2) [5]. Macrolide계(clarithromycin, azithromycin) 은 S. pneumoniae의 내성률은 약 30%로 보고되어 초기 치 료로 추천되지 않는다. Trimethoprim-sulfamethoxazole 은 S. pneumoniae 및 H. influenzae에서 내성률이 높아 (약 30-40%) 1차 약제로 추천되지 않는다. 2세대 혹은 3세대 경 구용 cephalosporin (cefpodoxime, cefdinir, 또는 cefditoren) 은 S. pneumoniae에 대한 내성률이 다양하여 1차 선택 약제 로 추천되지 않으나, 페니실린 대체약제로 페니실린에 대한 알레르기(type 1 과민반응 포함)의 병력이 있는 소아의 급성세 균성부비동염의 치료에 고려할 수 있다[5]. 항생제 치료기간은 10일에서 28일을 유지하며, 다른 대안 으로 증상 및 징후 호전 후 7일간 항생 제를 유지하는 것을 고려할 수 있다[5]. 치료 시작 72시간 이내에 증상의 악화 나 새로운 증상 혹은 징후가 나타나는 경 우, 또는 호전이 되지 않는 경우 초기 치 료를 다시 평가하도록 한다. 이 때, 내성 균을 고려하여 1차 약제를 변경하거나, 해부학적 이상 등과 같은 비감염성 원인 에 대한 평가를 하는 것이 필요하다. 그 밖에 국소 혹은 경구 충혈제거제 혹은 항 히스타민제는 추천되지 않는다[14].
결론
소아에서 급성부비동염은 매우 흔한 질 환으로 대부분은 바이러스에 의해 발생하 며, 드물게 급성세균성부비동염이 발생할 수 있다. 바이러스감염의 자연경과에 대한 이해를 바탕으로 세 균감염을 감별하며, 환자의 임상경과에 대한 정확하고 자세한 검진을 통해 항생제 치료가 필요한 대상군을 잘 선정하는 것이 중요하다. 항생제 치료목표는 부비동 내 감염을 일으키는 균주 를 제거할 수 있을 정도의 적절한 시간 동안 약물농도를 유지 하는 것이며, 이를 위해서는 국내 역학을 고려한 항생제 선택 및 치료반응에 대한 적절한 평가가 수반되어야 한다. 찾아보기말: 부비동염; 항생제; 소아 ORCIDHyunju Lee, https://orcid.org/0000-0003-0107-0724
REFERENCES
1. Revai K, Dobbs LA, Nair S, Patel JA, Grady JJ, Chonmaitree T. Incidence of acute otitis media and sinusitis complicating upper respiratory tract infection: the effect of age. Pediatrics 2007;119:e1408-e1412.
Signs & symptoms either;
1) Severe onset (fever 39 , purulent rhinorrhea, facial pain)( 3 days)
2) Persistent illness ( 10 days)
3) Worsening course (URI symptoms that appear to improve, followed by the sudden onset of worsening symptoms after 5-6 days)
1) Severe onset
3) Worsening course 2) Persistent illness
Antimicrobial therapy Check risk* for antibiotic resistance
Observation for 3 days
No improvement * Risk for antibiotic resistance
- Severe infection - Day care center - Age <2 years - Recent admission - Prior antibiotics within past 1 month
- Immunocompromised
No Yes
Standard dose
Amoxicillin- clavulanate Amoxicillin- clavulanateHigh dose
Check response within 72 hours of treatment
Antimicrobial therapy 10-28 days, or 7 days after improvement of symptoms/signs Reassess initial antimicrobial therapy Worsening or new symptoms/signs Improvement
Figure 2. Algorithm for treatment of acute rhinosinusitis in children. URI, upper respiratory tract infection.
Reproduced from Korea Centers for Disease Control and Prevention. Guidelines for the antibiotic use in children with acute upper respiratory tract infections. Cheongju: Korea Centers for Disease Control and Prevention; 2016 [5].
2. Gwaltney JM Jr, Wiesinger BA, Patrie JT. Acute community-acquired bacterial sinusitis: the value of antimicrobial treat-ment and the natural history. Clin Infect Dis 2004;38:227-233. 3. DeMuri GP, Gern JE, Moyer SC, Lindstrom MJ, Lynch SV,
Wald ER. Clinical features, virus identification, and sinusitis as a complication of upper respiratory tract illness in children ages 4-7 years. J Pediatr 2016;171:133-139.
4. Kronman MP, Zhou C, Mangione-Smith R. Bacterial pre-valence and antimicrobial prescribing trends for acute respi-ratory tract infections. Pediatrics 2014;134:e956-e965. 5. Korea Centers for Disease Control and Prevention. Guidelines
for the antibiotic use in children with acute upper respiratory tract infections. Cheongju: Korea Centers for Disease Control and Prevention; 2016.
6. Gwaltney JM Jr. Acute community-acquired sinusitis. Clin Infect Dis 1996;23:1209-1223.
7. Wald ER, Milmoe GJ, Bowen A, Ledesma-Medina J, Salamon N, Bluestone CD. Acute maxillary sinusitis in children. N Engl J Med 1981;304:749-754.
8. Wald ER, Reilly JS, Casselbrant M, Ledesma-Medina J, Milmoe GJ, Bluestone CD, Chiponis D. Treatment of acute maxillary sinusitis in childhood: a comparative study of amo-xicillin and cefaclor. J Pediatr 1984;104:297-302.
9. Parsons DS, Wald ER. Otitis media and sinusitis: similar dis-eases. Otolaryngol Clin North Am 1996;29:11-25.
10. Casey JR, Adlowitz DG, Pichichero ME. New patterns in the otopathogens causing acute otitis media six to eight years after introduction of pneumococcal conjugate vaccine. Pediatr Infect Dis J 2010;29:304-309.
11. Wald ER, Applegate KE, Bordley C, Darrow DH, Glode MP, Marcy SM, Nelson CE, Rosenfeld RM, Shaikh N, Smith MJ, Williams PV, Weinberg ST; American Academy of Pediatrics. Clinical practice guideline for the diagnosis and management of acute bacterial sinusitis in children aged 1 to 18 years. Pediatrics 2013;132:e262-e280.
12. Choe YJ, Lee HJ, Lee H, Oh CE, Cho EY, Choi JH, Kang HM, Yoon IA, Jung HJ, Choi EH. Emergence of antibiotic-resistant non-vaccine serotype pneumococci in nasopharyn-geal carriage in children after the use of extended-valency pneumococcal conjugate vaccines in Korea. Vaccine 2016;34: 4771-4776.
13. Meltzer EO, Hamilos DL, Hadley JA, Lanza DC, Marple BF, Nicklas RA, Bachert C, Baraniuk J, Baroody FM, Benninger MS, Brook I, Chowdhury BA, Druce HM, Durham S, Ferguson B, Gwaltney JM Jr, Kaliner M, Kennedy DW, Lund V, Naclerio R, Pawankar R, Piccirillo JF, Rohane P, Simon R, Slavin RG, Togias A, Wald ER, Zinreich SJ; American Academy of Allergy, Asthma and Immunology; American Academy of Otolaryngic Allergy; American Academy of Otolaryngology-Head and Neck Surgery; American College of Allergy, Asthma and Immunology; American Rhinologic Society. Rhinosinusitis: establishing definitions for clinical
research and patient care. Otolaryngol Head Neck Surg 2004;131(6 Suppl):S1-S62.
14. Chow AW, Benninger MS, Brook I, Brozek JL, Goldstein EJ, Hicks LA, Pankey GA, Seleznick M, Volturo G, Wald ER, File TM Jr; Infectious Diseases Society of America. IDSA clinical practice guideline for acute bacterial rhinosinusitis in children and adults. Clin Infect Dis 2012;54:e72-e112.
15. Kovatch AL, Wald ER, Ledesma-Medina J, Chiponis DM, Bedingfield B. Maxillary sinus radiographs in children with nonrespiratory complaints. Pediatrics 1984;73:306-308. 16. Shopfner CE, Rossi JO. Roentgen evaluation of the paranasal
sinuses in children. Am J Roentgenol Radium Ther Nucl Med 1973;118:176-186.
17. Diament MJ, Senac MO Jr, Gilsanz V, Baker S, Gillespie T, Larsson S. Prevalence of incidental paranasal sinuses opaci-fication in pediatric patients: a CT study. J Comput Assist Tomogr 1987;11:426-431.
18. Kristo A, Alho OP, Luotonen J, Koivunen P, Tervonen O, Uhari M. Cross-sectional survey of paranasal sinus magnetic resonance imaging findings in schoolchildren. Acta Paediatr 2003;92:34-36.
19. Kristo A, Uhari M, Luotonen J, Koivunen P, Ilkko E, Tapiainen T, Alho OP. Paranasal sinus findings in children during respi-ratory infection evaluated with magnetic resonance imaging. Pediatrics 2003;111(5 Pt 1):e586-e589.
20. Younis RT, Lazar RH, Anand VK. Intracranial complications of sinusitis: a 15-year review of 39 cases. Ear Nose Throat J 2002;81:636-638, 640-642, 644.
21. Fallon RM, Kuti JL, Doern GV, Girotto JE, Nicolau DP. Phar-macodynamic target attainment of oral beta-lactams for the empiric treatment of acute otitis media in children. Paediatr Drugs 2008;10:329-335.
Peer Reviewers’ Commentary
본 원고에서는 2016년에 질병관리본부 정책연구용역사업으로 발표된 “국내 소아 급성 상기도 감염의 항생제 사용 지침” 중 국 내 소아의 급성 부비동염의 원인, 진단 및 치료에 대해 소개하고 있다. 소아에서 급성 부비동염은 매우 흔한 질환으로 대부분은 바이러스에 의해 발생하나 임상적으로 세균성을 의심하여 항생 제를 불필요하게 쓰는 경우가 많다. 본 원고는 국내 소아에서 항 생제 치료가 필요한 급성 세균성 부비동염을 임상적으로 진단하 는 가이드를 제시하고 있으며, 여러 국내외 데이터를 기반으로 급성 세균 부비동염의 원인 및 균의 감수성 패턴과 기전에 대해 설명하였고 항생제 치료에 대한 가이드를 제시하여 일선 의료 현장에서 활용하는 데에 도움을 줄 것으로 생각된다. [정리: 편집위원회]