저작자표시-비영리-변경금지 2.0 대한민국 이용자는 아래의 조건을 따르는 경우에 한하여 자유롭게 l 이 저작물을 복제, 배포, 전송, 전시, 공연 및 방송할 수 있습니다. 다음과 같은 조건을 따라야 합니다: l 귀하는, 이 저작물의 재이용이나 배포의 경우, 이 저작물에 적용된 이용허락조건 을 명확하게 나타내어야 합니다. l 저작권자로부터 별도의 허가를 받으면 이러한 조건들은 적용되지 않습니다. 저작권법에 따른 이용자의 권리는 위의 내용에 의하여 영향을 받지 않습니다. 이것은 이용허락규약(Legal Code)을 이해하기 쉽게 요약한 것입니다. Disclaimer 저작자표시. 귀하는 원저작자를 표시하여야 합니다. 비영리. 귀하는 이 저작물을 영리 목적으로 이용할 수 없습니다. 변경금지. 귀하는 이 저작물을 개작, 변형 또는 가공할 수 없습니다.
Sectioned images and surface models of a cadaver
for understanding
the deep circumflex iliac artery flap
by
Bong Chul Kim
Major in Medicine
Department of Medicine
Sectioned images and surface models of a cadaver
for understanding
the deep circumflex iliac artery flap
by
Bong Chul Kim
A Dissertation Submitted to The Graduate School of
Ajou University in Partial Fulfillment of the Requirements for
The Degree of Ph.D. of Medicine
Supervised by
Min Suk Chung, M.D., Ph.D.
Major in Medicine
Department of Medicine
The Graduate School, Ajou University
February, 2016
i - ABSTRACT -
Sectioned images and surface models of a cadaver
for understanding the deep circumflex iliac artery flap
The aim of this study was to describe the deep circumflex iliac artery (DCIA) flap from sectioned images and stereoscopic anatomic models using Visible Korean, for the benefit of medical education and clinical training in the field of oromandibular reconstructive surgery. Serially sectioned images of the pelvic area were obtained from a cadaver. Outlines of significant structures in the sectioned images were drawn and stacked to build surface models. The PDF (portable document format) file (size, 30 MB) of the constructed models is available for free download on the Web site of the Department of Anatomy at Ajou University School of Medicine (http://anatomy.co.kr). In the PDF file, the relevant structures of the DCIA flap can be seen in the sectioned images. All surface models and stereoscopic structures associated with the DCIA flap are displayed in real time. We hope that these state-of-the-art sectioned images, outlined images, and surface models will help students and trainees better understand the anatomy associated with DCIA flap.
Key Words: Cross-sectional anatomy, three-dimensional imaging, deep circumflex iliac artery, vascularized osseous free flap, mandibular reconstruction
ii
Contents
ABSTRACT ··· ⅰ Contents ··· ⅱ Figure legends ··· ⅲ Table legend ··· ⅳ . Ⅰ Introduction ··· 1 . Ⅱ Materials and Methods ··· 2A. Outlining of the Images ··· 2
B. Reconstruction of Surface Models ··· 3
C. Virtual Harvesting of the DCIA Flap··· 4
D. PDF File of Surface Models ··· 7
. Ⅲ Results ··· 7 . Ⅳ Discussion ··· 8 . Ⅴ Conclusion ··· 10 References ··· 10
iii
Figure legends
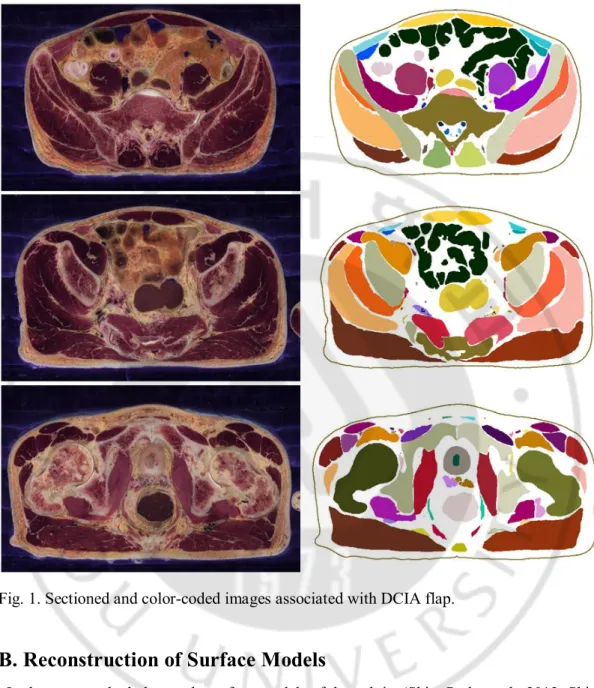
Fig. 1. Sectioned and color-coded images associated with DCIA flap. ··· 3
Fig. 2. Stereolithography files for making surface models of the virtual harvesting of the DCIA flap on Maya software. Myo-osseous free flap (indicated as wire frame) including the internal abdominal oblique muscle, transversus abdominis muscle, iliac bone, DCIA, ascending branch of DCIA, and DCIV was described. ··· 5
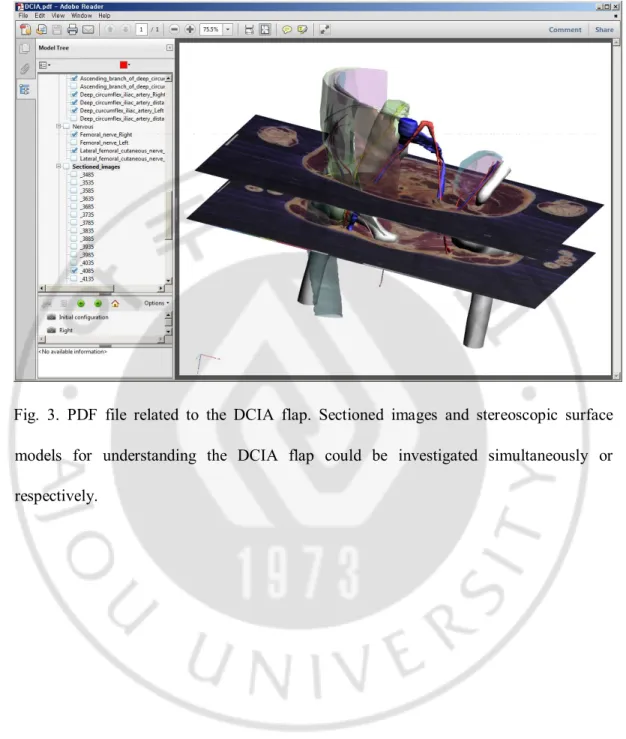
Fig. 3. PDF file related to the DCIA flap. Sectioned images and stereoscopic surface models for understanding the DCIA flap could be investigated simultaneously or respectively. ··· 6
iv
Table legend
Table 1. Fifty-nine surface models, categorized according to the systems and subsequent groups ··· 4
1
-I. Introduction
The aim of oromandibular reconstruction is the restoration of both form and function, for which appearance, mastication, speech, deglutition, and oral competence all should be considered. (Kim et al., 2012) The positioning of the oromandibular area makes it a highly visible one, and therefore, during reconstruction and tissue coverage, much emphasis is placed on imitating the resected native tissue to gain superior aesthetic and functional results. (Kim et al., 2012) At present, vascularized osseous free flaps are the most feasible option for reconstruction of oromandibular defects, especially those greater than 5 cm in diameter. (Foster et al., 1999; Kim B. C. et al., 2013)
The deep circumflex iliac artery (DCIA) flap is a useful option for the reconstruction of the mandible. (Taylor et al., 1979c, 1979a; Kang et al., 2008) In this procedure, a strong, thick, and tall bone of proper stock and sufficient length is used to support an osteointegrated implant, so as to reasonably match the contour and shape of the mandible. (Kim H. S. et al., 2013) However, because of its anatomical approach being considerably more difficult than that for other flaps, and the high risk of donor-site morbidity, (ie, abdominal hernia) the DCIA flap is a less popular choice for composite mandibular reconstructions, (Kim et al., 2012; Kim H. S. et al., 2013) Therefore, it is helpful to understand the anatomy associated with the DCIA flap.
Not only have we already developed sectioned images and surface models of cadaver pelvis, (Shin, Park, et al., 2012; Shin et al., 2013) but we have also introduced a browsing software that an ordinary user can use to search for sectional images tagged by their name. (Shin et al., 2011; Shin, Jang, et al., 2012) Moreover, we have enabled surface models to be viewed in a portable document format (PDF) file in the free software package Adobe Reader, Windows version 9 (Adobe Systems, Inc, San Jose, CA). (Shin, Chung, et al., 2012; Shin, Jang, et al., 2012) The Visible Korean images were obtained from thin-slice (interval, 0.1 mm) cross-sectional human data sets, and their color is similar to that the actual structures shown in the images.
However, the pelvic data obtained to date have proven to be insufficient to effectively illustrate the DCIA flap. Therefore, the purpose of this study was to present sectioned images and stereoscopic anatomic models of the DCIA flap, which may be beneficial to medical education and clinical training in the field of oromandibular reconstructive surgery. We aim for the data to be accessible to maxillofacial surgeons who may want to gain a better
2
-understanding of the anatomy associated with the DCIA flap, eventually improving the surgical outcomes of their procedures. Comprehensive anatomical knowledge maximizes surgical predictability and allows surgeons to avoid unfavorable complications. Moreover, the DCIA flap can be virtually harvested using the PDF file from this study.
II. Materials and Methods
A. Outlining of the Images
In our previous studies, we had presented an advanced, progressive outlining technique. (Shin, Park, et al., 2012; Shin et al., 2013) We had developed sectioned and outlined images (interval, 0.1 mm; pixel size, 0.1 mm; color depth, 48-bit color; file format, tagged image file format [TIFF]) of a male cadaver. (Shin, Park, et al., 2012) From these sectioned and outlined images of the whole body, only the images pertaining to the pelvic region, relevant to the DCIA flap, were chosen.
In addition, we prepared outlined images of the structures associated with the DCIA flap (eg, DCIA) manually on Mimics, version 16.0 (Materialise, Inc, Leuven, Belgium) at 1.0-mm intervals with a 0.2-1.0-mm pixel size (Fig. 1). (Cho et al., 2013) The outlines of each of the structures were filled with a specific color, either semiautomatically or manually (Fig. 1). (Shin, Chung, et al., 2012; Shin, Jang, et al., 2012; Shin, Park, et al., 2012)
3
-Fig. 1. Sectioned and color-coded images associated with DCIA flap.
B. Reconstruction of Surface Models
In the past, we had also made surface models of the pelvis. (Shin, Park, et al., 2012; Shin et al., 2013) For this study, we constructed additional surface models that were specifically associated with the DCIA flap. Outlined images, made during the previous step, were also surface reconstructed for the purpose of oromandibular reconstructive surgery.
However, it was not possible to make outlined images of very small or thin structures (ie, distal part of the lateral femoral cutaneous nerve). In such cases, we directly drew these structures on Maya, version 2013 (Autodesk, Inc, San Rafael, CA) with reference adjacent structures and an atlas. (Shin, Park, et al., 2012; Urken et al., 2012; Shin et al., 2013) For example, to make the distal parts of lateral femoral cutaneous nerve, the curves of the
4
-structures were drawn using a ‘‘curve’’ tool, and the surfaces were made from these curves using an ‘‘extrude’’ tool. (Palamar, 2013)
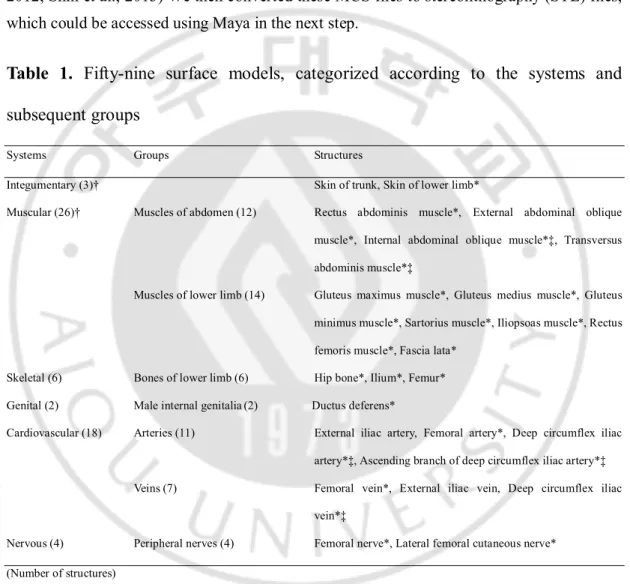
A total of 59 structures have been surface reconstructed (Table 1). These surface models were then categorized and saved as Mimics (MCS) files. An article published previously describes the method of reconstruction for surface models using Mimics. (Shin, Park, et al., 2012; Shin et al., 2013) We then converted these MCS files to stereolithography (STL) files, which could be accessed using Maya in the next step.
Table 1. Fifty-nine surface models, categorized according to the systems and
subsequent groups
Systems Groups Structures
Integumentary (3)† Skin of trunk, Skin of lower limb*
Muscular (26)† Muscles of abdomen (12) Rectus abdominis muscle*, External abdominal oblique muscle*, Internal abdominal oblique muscle*‡, Transversus abdominis muscle*‡
Muscles of lower limb (14) Gluteus maximus muscle*, Gluteus medius muscle*, Gluteus minimus muscle*, Sartorius muscle*, Iliopsoas muscle*, Rectus femoris muscle*, Fascia lata*
Skeletal (6) Bones of lower limb (6) Hip bone*, Ilium*, Femur* Genital (2) Male internal genitalia(2) Ductus deferens*
Cardiovascular (18) Arteries (11) External iliac artery, Femoral artery*, Deep circumflex iliac artery*‡, Ascending branch of deep circumflex iliac artery*‡ Veins (7) Femoral vein*, External iliac vein, Deep circumflex iliac
vein*‡
Nervous (4) Peripheral nerves (4) Femoral nerve*, Lateral femoral cutaneous nerve* (Number of structures)
*Bilateral structures are surface reconstructed. †Surface is made semitransparent.
‡Segmented surface models to describe myo-osseous deep circumflex iliac artery flap.
C. Virtual Harvesting of the DCIA Flap
5
-combined structures (Table 1). The color of skin and muscle was made semitransparent so as to reveal the inner structures (Fig. 3). If any surface models had been inadequately outlined, a maxillofacial surgeon and an anatomist corrected them. (Shin et al., 2011)
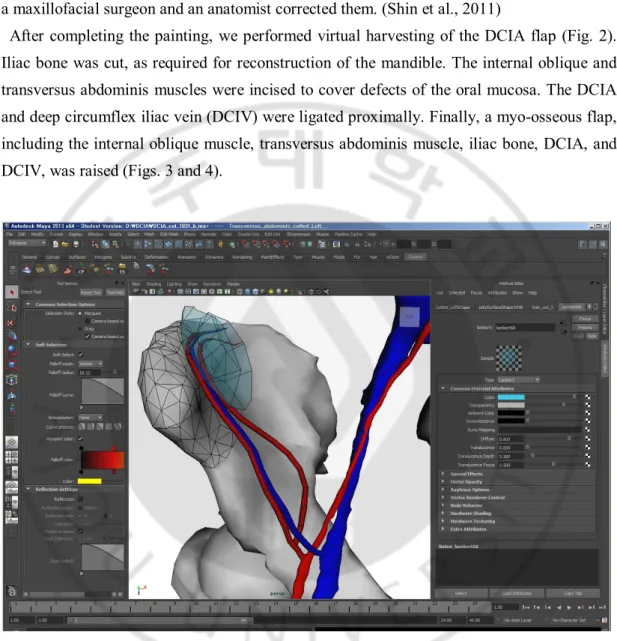
After completing the painting, we performed virtual harvesting of the DCIA flap (Fig. 2). Iliac bone was cut, as required for reconstruction of the mandible. The internal oblique and transversus abdominis muscles were incised to cover defects of the oral mucosa. The DCIA and deep circumflex iliac vein (DCIV) were ligated proximally. Finally, a myo-osseous flap, including the internal oblique muscle, transversus abdominis muscle, iliac bone, DCIA, and DCIV, was raised (Figs. 3 and 4).
Fig. 2. Stereolithography files for making surface models of the virtual harvesting of the DCIA flap on Maya software. Myo-osseous free flap (indicated as wire frame) including the internal abdominal oblique muscle, transversus abdominis muscle, iliac bone, DCIA, ascending branch of DCIA, and DCIV was described.
6
-Fig. 3. PDF file related to the DCIA flap. Sectioned images and stereoscopic surface models for understanding the DCIA flap could be investigated simultaneously or respectively.
7
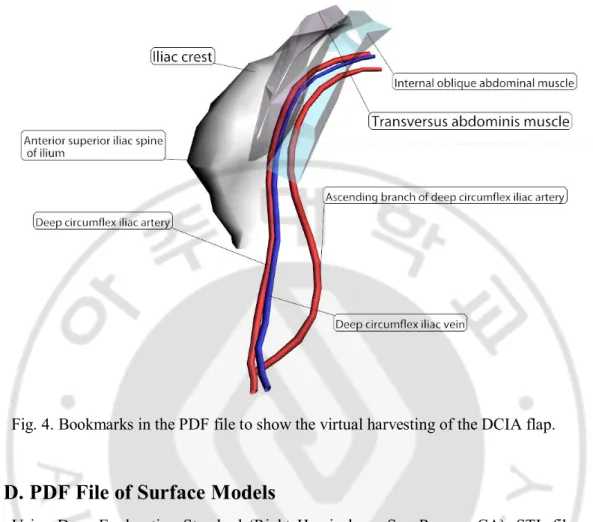
-Fig. 4. Bookmarks in the PDF file to show the virtual harvesting of the DCIA flap.
D. PDF File of Surface Models
Using Deep Exploration Standard (Right Hemisphere, San Ramon, CA), STL files were classified based on structures, and the surface models were organized according to their official anatomical names. All the models in the STL files were assembled and saved as DCIA.pdf using 3D Reviewer, a software package accompanying Acrobat 9.0 Pro Extended (Adobe Systems, Inc). (Shin, Chung, et al., 2012; Shin, Jang, et al., 2012; Shin et al., 2013) Because the PDF file was accessed in Adobe Reader, the anatomical names of the parts and virtual harvesting of the DCIA flap were presented in the model tree window.
In Acrobat, we assembled bookmarks for the PDF files as follows: all structures, skin removed, muscles removed, bones removed, blood vessels removed, nerve removed, and DCIA flap (Figs. 3 and 4).
III. Results
8
-Anatomy at Ajou University School of Medicine (http://anatomy.co.kr). In the sectioned images, structures associated with flap harvesting can be seen and are verified as anatomically correct.
Moreover, the surface models and stereoscopic structures related with the DCIA flap were described in real time. The relevant anatomical structures concerning the DCIA flap can be easily identified in the sectional images and stereoscopic aspects of the PDF file; examples are as follows:
In the sectioned images, users can detect the diameter of the DCIA and the DCIV (Fig. 1). They can also observe the vertical relationship between the DCIA, the DCIV, and the abdominis muscle (Fig. 1). The DCIA and DCIV are positioned medially to the anterior superior iliac spine (Fig. 1). In addition, the vertical relationship of the lateral femoral cutaneous nerve and spermatic cord can be detected (Fig. 1). Considering all these factors, users can understand that the diameters of the DCIA and the DCIV are appropriate for microanastomosis with neck vessels (ie, facial artery and vein). Moreover, users can recognize that care is required when dissecting and sectioning the internal abdominal oblique and transversus abdominis muscles so as to avoid damage of the DCIA and the DCIV. On the stereoscopic surface models, the length of the DCIA and DCIV could be identified and proved suitable for reconstruction of the oromandibular defect (Fig. 3). The origins of the DCIA and DCIV were described relative to the level of the inguinal ligament. Thus, it was perceived that the DCIA and DCIV usually originate from the external iliac artery and vein, superior to the inguinal ligament (Fig. 3). In addition, the DCIV was not formed from the vena comitantes of the DCIA, but instead arose independently from the external iliac vein (Figs. 3 and 4). The user was also able to understand the distance between the DCIA and DCIV (Fig. 3). The ascending branch of the DCIA could be recognized too, and so the user could understand the branching point of the ascending branch of the DCIA (Figs. 3 and 4). The spermatic cord was located medially to the DCIA and DCIV in the male patient (Fig. 3). By these considerations, the user could be accustomed to the DCIA flap.
On the basis of this knowledge, virtual harvesting of the DCIA flap could be achieved in the PDF file (Fig. 4). Flap harvesting was performed with dissection of the DCIA, DCIV, and ascending branch of the DCIA. The iliac bone and the muscle cuff of the internal oblique abdominal and transversus abdominis muscles for the reconstruction of the defect were included along with the preservation of the DCIA (Fig. 4).
9
Unlike other surface models, such as Visiblebody or Zygotebody, ("http://www.visiblebody.com/index.html," ; "http://www.zygotebody.com,") our PDF files provide scientific data that can be manipulated offline. In particular, the surface models in this study are constructed on the basis of scientific data. They were created by outlining structures in serially sectioned images, stacking these outlines, and finally using a polygon-based surface reconstruction method. (Shin, Park, et al., 2012; Shin et al., 2013) The resultant models are thorough and differ from available surface models that are manually produced by artists with a knowledge of anatomy. The surface models in this study also provide the corresponding sectional images (Fig. 3).
The DCIA flap is a useful option for microsurgical oromandibular reconstruction. (Taylor et al., 1979c, 1979a) It provides sufficient length of a thick, strong, and tall bone, which is of adequate stock to support an osteointegrated dental implant, all the while maintaining the right shape for the hemimandible. (Kim et al., 2012) Despite these features, the flap remains an unpopular choice for the reconstruction of oromandibular defects, because of the higher risk of donor-site morbidity (ie, abdominal hernia) and the relatively difficult flap-harvesting technique. (Kim et al., 2012) For this reason, it is beneficial to accumulate a good foundation of anatomical knowledge related to the DCIA flap.
In our previous study, we have already described surface models of a cadaver pelvis, (Shin, Park, et al., 2012; Shin et al., 2013) and this was helpful in understanding the anatomical structures in the pelvic area. However, the previous study did not assess the vital structures for the DCIA flap (ie, the DCIA). Therefore, in the current study, we have added a series of structures relevant to the DCIA flap and reported the virtual operative procedure associated with harvesting the DCIA flap, all to improve surgical outcomes and reduce complications. The dissection of the DCIA flap begins with a skin incision along the iliac crest and inguinal ligament. In connection with the depth of the skin incision, sectional images of this study are helpful because the vertical relationships of the skin, external oblique abdominal muscle, and external iliac artery can all be appreciated. After the skin incision and dissection, the user is required to identify the external oblique abdominal muscle and the external iliac artery. On the basis of the stereoscopic structures in the PDF file in this study, the user confirms that there is a relatively avascular area under the cuff of the external oblique abdominal muscle. The incision is then performed through the external oblique abdominal muscle, adjacent to the iliac crest medially. It is elevated by a blunt and sharp dissection, and the internal oblique abdominal muscle is revealed.
- 10 -
The stereoscopic structures in this study show that both the DCIA and DCIV are positioned between the internal oblique abdominal and transversus abdominis muscles, and therefore, meticulous incision and dissection are required to elevate them. These muscles are elevated only enough to cover the oromandibular defect. The stereoscopic structures in this study affirm that the DCIA, the DCIV, and area associated with the ascending branch of the DCIA are all maintained in the elevated muscles. Meanwhile, the dissection is followed inferiorly, at which stage the user finds that the DCIA and DCIV both originate from the external iliac artery and vein in the stereoscopic structure.
In addition, the sectioned images express the depth of the external iliac artery from the skin, as well as the diameter of the DCIA and DCIV. A sharp dissection along the lateral border of the iliac crest is done to expose the outer table of the ilium and perform the osteotomies. Finally, the DCIA and DCIV are dissected from the adjacent soft tissue and cut at their origin from the external iliac artery and vein. In this manner, the sectional and stereoscopic images in this study are profitable for the harvesting of the DCIA flap.
V. Conclusion
We hope that this study will contribute to a thorough understanding of the anatomy associated with the DCIA flap, ensuring better surgical outcomes of oromandibular reconstruction procedures that use the DCIA flap. It is aimed, in particular, at students and trainees in the field of maxillofacial reconstructive surgery to help them effectively grasp the principles underlying the use of the DCIA flap.
References
Cho SW, Jharia TK, Moon YL, Sim SW, Shin DS, Bigliani LU: Three-dimen
sional templating arthroplasty of the humeral head Surg Radiol Anat 3
5: 685-688, 2013
Foster RD, Anthony JP, Sharma A, Pogrel MA: Vascularized bone flaps versu
s nonvascularized bone grafts for mandibular reconstruction: an outcome
analysis of primary bony union and endosseous implant success Head
- 11 -
Neck 21: 66-71, 1999
http://www.visiblebody.com/index.html:
http://www.zygotebody.com:
Kang SH, Kim HJ, Cha IH, Nam W: Mandibular condyle and infratemporal f
ossa reconstruction using vascularised iliac crest and vascularised calvar
ial bone graft J Plast Reconstr Aesthet Surg 61: 1561-1562, 2008
Kim BC, Kim S, Nam W, Cha IH, Kim HJ: Mandibular reconstruction with v
ascularized osseous free flaps: a review of the literature Asian Pac J C
ancer Prev 13: 553-538, 2012
Kim BC, Yoon JH, Choi B, Lee J: Mandibular reconstruction with autologous
human bone marrow stem cells and autogenous bone graft in a patien
t with plexiform ameloblastoma J Craniofac Surg 24: e409-411, 2013
Kim HS, Kim BC, Kim HJ, Kim HJ: Anatomical basis of the deep circumfle
x iliac artery flap J Craniofac Surg 24: 605-609, 2013
Palamar T: Mastering Autodesk Maya 2013. Hoboken, NJ: Sybex, 2013
Shin DS, Chung MS, Park HS, Park JS, Hwang SB: Browsing software of th
e Visible Korean data used for teaching sectional anatomy Anat Sci Ed
uc 4: 327-332, 2011
Shin DS, Chung MS, Park JS: Systematized methods of surface reconstruction
from the serial sectioned images of a cadaver head J Craniofac Surg
23: 190-194, 2012
Shin DS, Jang HG, Hwang SB, Har DH, Moon YL, Chung MS: Two-dimensi
onal sectioned images and three-dimensional surface models for learning
the anatomy of the female pelvis Anat Sci Educ 6: 316-323, 2013
Shin DS, Jang HG, Park JS, Park HS, Lee S, Chung MS: Accessible and info
rmative sectioned images and surface models of a cadaver head J Cran
iofac Surg 23: 1176-1180, 2012
Shin DS, Park JS, Park HS, Hwang SB, Chung MS: Outlining of the detailed
structures in sectioned images from Visible Korean Surg Radiol Anat
34: 235-247, 2012
Taylor GI, Townsend P, Corlett R: Superiority of the deep circumflex iliac ves
sels as the supply for free groin flaps Plast Reconstr Surg 64: 595-604,
1979a
- 12 -