저작자표시-비영리-변경금지 2.0 대한민국 이용자는 아래의 조건을 따르는 경우에 한하여 자유롭게 l 이 저작물을 복제, 배포, 전송, 전시, 공연 및 방송할 수 있습니다. 다음과 같은 조건을 따라야 합니다: l 귀하는, 이 저작물의 재이용이나 배포의 경우, 이 저작물에 적용된 이용허락조건 을 명확하게 나타내어야 합니다. l 저작권자로부터 별도의 허가를 받으면 이러한 조건들은 적용되지 않습니다. 저작권법에 따른 이용자의 권리는 위의 내용에 의하여 영향을 받지 않습니다. 이것은 이용허락규약(Legal Code)을 이해하기 쉽게 요약한 것입니다. Disclaimer 저작자표시. 귀하는 원저작자를 표시하여야 합니다. 비영리. 귀하는 이 저작물을 영리 목적으로 이용할 수 없습니다. 변경금지. 귀하는 이 저작물을 개작, 변형 또는 가공할 수 없습니다.
Effect of ratio of residual alveolar bone to
graft material in contact with fixture
surface on marginal bone loss of implants
in augmented maxillary sinuses: A 1-year
retrospective study
Chan-Ho Park
Department of Dental science
The Graduate School, Yonsei University
Effect of ratio of residual alveolar bone to
graft material in contact with fixture
surface on marginal bone loss of implants
in augmented maxillary sinuses: A 1-year
retrospective study
Directed by Professor Ik-Sang Moon
The Doctoral Dissertation
submitted to the Department of Dentistry,
the Graduate School of Yonsei University
in partial fulfillment of the requirements for the degree of
Doctor of Philosophy
This certifies that the Doctoral Dissertation
of Chan-Ho Park is approved.
The Graduate School
Yonsei University
감사의 글
박사 과정을 마치며 도와주신 모든 분들께 깊은 감사 인사를 드립니다. 먼저, 이 논문이 완성되기까지 끊임없이 지도해주시고 연구에 매진할 수 있도록 격려해주신 문익상 지도 교수님, 이동원 교수님께 진심으로 감사 드립니다. 또한 바쁘신 와중에도 심사를 맡아주시고 조언을 아끼지 않으신 김기덕 교수님, 허종기 교수님, 윤정호 교수님께도 감사 드립니다. 아울러 수련기간을 함께했던 해석이 형과 심사가 무사히 진행되고 완료될 수 있도록 도움을 준 재용이 형, 그리고 치주과의 모든 의국원들에게도 고마움을 전합니다. 마지막으로 세상 그 누구보다 소중한 저희 가족에게 고마움을 전합니다. 언제나 저를 믿음으로 지켜봐 주시고 무한한 격려와 지지를 보내주시는 사랑하는 부모님과 항상 저에게 응원을 보내주는 누나, 매형에게 고마움을 전합니다. 2017년 6월 저자 씀
TABLE OF CONTENTS
LEGENDS OF FIGURES, TABLES
··· iABSTRACT (ENGLISH)
··· iv
I. INTRODUCTION
··· 1
II. MATERIALS AND METHODS
··· 4
1. Patient selection
··· 4
2. Implant design
··· 5
3. Surgical procedure
··· 6
4. Radiographic examination and evaluation
··· 7
5. Statistical analysis
··· 11
III. RESULTS
··· 13
IV. DISCUSSION
··· 15
V. CONCLUSION
··· 18
VI. REFERENCE
··· 19
ABSTRACT (KOREAN)
··· 28
LEGEND OF FIGURES
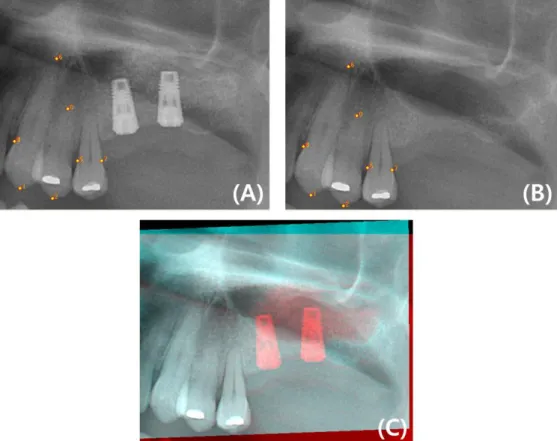
Figure 1. Process of image registration and mosaicing. (A), Registered
radiograph taken immediately after implant placement; (B),
Registered radiograph taken before sinus augmentation; (C),
Mosaicing of 2 registered images ··· 8
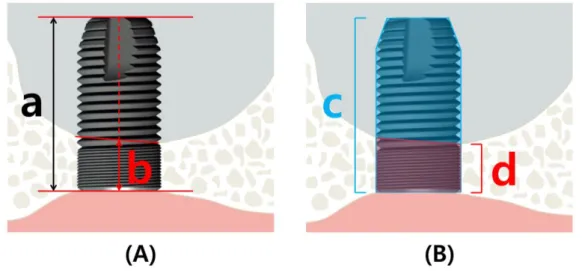
Figure 2.
(A) Linear measurements, and (B) 2-dimensional measurements that
were obtained between landmarks.
a, Length of implant:
perpendicular distance from the implant shoulder to the most apical
part of the fixture; b, Residual bone height: perpendicular distance
from the implant shoulder to the sinus floor; c, Area of implant:
two-dimensional area of the outermost layer of the fixture in grafted area;
d, Residual bone area: 2-dimensional area of the outermost layer of
the fixture in native bone ··· 9
Figure 3. Intraoral radiographs with a 5.5-mm spherical metal bearing taken
(A) immediately after and (B) 1 year after prosthesis delivery ···· 10
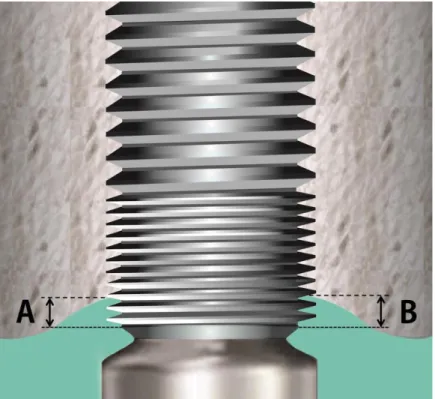
Figure 4. Schematic illustration of the site and reference point measurements.
A and B, distance from the reference point to the marginal bone at
the mesial and distal parts of the implant, respectively ··· 11
LEGEND OF TABLES
Table 1. Pearson’s correlation analysis between the marginal bone loss and the
following parameters; residual bone/implant length ratio, residual
bone/implant area ratio (N = 46) ··· 14
Table 2. Comparison of each peri-implant marginal bone loss in both implant
groups at 1 year after functional loading ··· 14
ABSTRACT
Effect of ratio of residual alveolar bone to graft material in contact with
fixture surface on marginal bone loss of implants in augmented maxillary
sinuses: A 1-year retrospective study
Chan-Ho Park, D.D.S.
Department of Dental Science
The Graduate School, Yonsei University
(Directed by Professor Ik-Sang Moon, D.D.S., M.S.D., Ph.D.)
The purpose of this retrospective study was to evaluate the influences of height or area ratio of residual alveolar bone to graft material on marginal bone loss around implants in the augmented maxillary sinuses with delayed implant placement. In this study,42 patients with Astra implants in sinuses that had been augmented with alloplasts and allografts or xenografts (alveolar bone height ≤ 5 mm) were selected. Marginal bone level surrounding 1 implant per sinus was assessed by radiographic imaging at the time of final restoration delivery and 12 months after functional loading. To evaluate the marginal bone level alterations using clinical and radiographic data, Pearson’s correlation analysis and Mann-Whitney test were performed.
Forty-six implants were included in this study. The residual bone/implant length ratio and the residual bone/implant area ratio were not associated with marginal bone loss at 1 year after functional loading (P > .05). And, marginal bone loss did not differ significantly between 2 types of graft materials during the observation period (P > .05).
The residual bone/implant length ratio and residual bone/implant area ratio were not associated with marginal bone loss around implants placed in augmented sinuses during 1 year of functional loading.
Effect of ratio of residual alveolar bone to graft material in contact with
fixture surface on marginal bone loss of implants in augmented maxillary
sinuses: A 1-year retrospective study
Chan-Ho Park, D.D.S.
Department of Dental Science
The Graduate School, Yonsei University
(Directed by Professor Ik-Sang Moon, D.D.S., M.S.D., Ph.D.)
I. INTRODUCTION
Dental implants are a predictable treatment for edentulism, with very well-documented long-term results (Adell et al., 1990; Albrektsson et al., 1986; Esposito et al., 2005).
Inserting implants into the posterior maxilla may be difficult because atrophy following loss of dentition or the presence of the maxillary sinus can result in a volume of bone insufficient for endosseous implants of adequate length (Sharan and Madjar, 2008; Wehrbein and Diedrich, 1992). In posterior areas, marginal bone loss can be more progressive because implants in these areas are strongly supported by thin cortical bone
around the most coronal part of the implant. The apical portion of the implant is poorly supported by loose trabecular bone, unless the implant is located to involve the cortical bone in the posterior maxilla (Jacobs, 2003; Miyamoto et al., 2005). Accordingly, the quality and quantity of the residual original bone play crucial indicators in the sequence of sinus augmentation and implant placement (ie, simultaneous vs delayed placement) (Fugazzotto, 2003; Wang and Katranji, 2008). In the less dense bone of the maxilla, because not only stability of implant, but also blood supply of contact area of fixture during regenerative phase play is important, the relationship between residual original bone height and length of fixture also seems to be intimate (Fugazzotto, 2003).
The maxillary sinus augmentation technique, first reported by Boyne and James (1980) allows for functional dental rehabilitation of partially or completely edentulous patients with insufficient bone volume or who require an implant close to the maxillary sinus. This procedure has subsequently been developed and modified by other clinicians (Del Fabbro et al., 2004; Pjetursson et al., 2008; Wallace and Froum, 2003).
Considering differences in properties between native bones and grafting materials, the presence of high-level strain increases with lower stiffness of graft placed in maxillary sinus, affecting marginal bone loss (MBL) around implants (Inglam et al., 2010). Implants placed in sinuses grafted with autogenous bone or anorganic bovine bone resulted in more MBL than did implants placed in pristine maxillary bone (Galindo-Moreno et al., 2014; Johansson et al., 1999). Because the marginal bone around implants must be able to withstand occlusal forces, maintaining the marginal bone level is key to dental implant success (Isidor, 1996, 2006). Close observation of the peri-implant marginal bone level is very important, especially in areas of the posterior maxilla that
have insufficient residual bone volume.
The aim of this study was to evaluate the influences of height or area ratio of residual alveolar bone to graft material in contact with implant surface on MBL around dental implants in the augmented maxillary sinuses with delayed implant placement.
II. MATERIALS AND METHODS
1. Patient selection
This retrospective study included data from patients who had maxillary unilateral and bilateral edentulism in the posterior maxillary area. The patients were selected using the following inclusion criteria:
(a) All surgical and restorative treatments were performed by experienced periodontists at the Department of Periodontology, Gangnam Severance Dental Hospital.
(b) Patients with a residual sinus floor of 5 mm or less, which generally allows for maxillary sinus augmentation with delayed implant placement (Wang and Katranji, 2008).
(c) Patients received sinus augmentation procedure with 1 of the 2 types of graft material: microporous and macroporous biphasic calcium phosphate (MBCP, Biomatlante Sarl, Nantes, France) in combination with frozen irradiated allogenic cancellous bone and marrow (ICB, Rocky Mountain Tissue Bank, Aurora, CO, USA) in a 1:1 ratio or deproteinized and sterilized bovine bone (Bio-Oss, Geistlich, Wolhusen, Switzerland).
(d) Patients received at least 1 implant treatment in the augmented sinus area (17-15, 25-27)
(e) Patients received at least 1 year of implant follow-up after functional loading and underwent standardized periapical radiography at the time of final restoration delivery (baseline) and at 12months after functional loading.
(f) Patients were able to understand and achieve oral hygiene maintenance procedures. (g) Patients were in good general health.
(h) Patients were at least 20 years of age.
Exclusion criteria included untreated active periodontitis, an American Society of Anesthesiologists score of 3 or greater (Smeets et al., 1998), bruxism/parafunction, heavy smoking (>10 cigarettes per day) (Galindo-Moreno et al., 2005), poor oral hygiene (modified plaque index greater than 2) (Mombelli et al., 1987), a history of taking medications associated with bone metabolism (e.g., bisphosphonates), sinus pathology (such as osteomas, carcinomas, and other cancers), postoperative complications, uncontrolled compromised systemic disease, and radiographs of unsuitable head positions or unapparent images.
This study was approved by the Institutional Review Board of Yonsei University (#3-2014-0236) for retrospective chart review and data collection.
2. Implant design
OsseoSpeed™ (Astra Tech, Mölndal, Sweden) implant system was used in this study. OsseoSpeed had a fluoride-modified TiO2-blasted surface, a microthreaded cervical neck,
implants included 22 implants with a straight-shaped configuration (diameter: 4.0 or 5.0mm) and 24 implants with a conical neck-shaped configuration (diameter: 5.0mm). The implant length varied between 8 and 13mm.
3. Surgical procedure
All surgical procedures were conducted under local anesthesia (2% lidocaine, 1:100,000 epinephrine, Yuhan Corp., Seoul, Korea). Sinus augmentation procedures were performed using the lateral window approach (Vercellotti et al., 2001). The mucoperiosteal flap was raised and an osteotomy was performed on the lateral wall of the maxillary sinus to prepare a bony window using a piezoelectric instrument (Piezosurgery, Mectron Medical Technology, Carasco, Italy) cooled with sterile saline solution. The sinus membrane was carefully dissected and elevated using mucosal sinus elevators. All sinus cavities were grafted using MBCP in combination with ICB in a 1:1 ratio or Bio-Oss. A variable mass of bone grafting material, ranging from 0.5 to 1 g, was used in each sinus. The bony wall was gently positioned to cover the lateral window, and a resorbable collagen membrane (Bio-Arm, ACE Surgical Supply Company, Inc., Brockton, MA, USA) was trimmed and adapted over the lateral aspect of the bony window. The mucoperiosteal flaps were sutured. Primary wound closure was achieved in all cases, and implant placement was performed after a healing period of 6 months following sinus augmentation. Sutures were removed 10 days after sinus surgery and implant surgery. The second operation was performed 6 months after the first operation for maxillary implants.
Prostheses were delivered 3 weeks after the second operation. Patients were recalled every 6 months for plaque control and oral hygiene evaluation.
4. Radiographic examination and evaluation
Panoramic radiographs (Promax, Planmeca, Helsinki, Finland) were taken before sinus augmentation procedure and immediately after fixture implantation. The original sinus floor and implant body were traced digitally using Photoshop (Adobe Systems, San Jose, CA) by a single investigator. For accurate identification of the original sinus floors in panoramic radiographs, image reconstruction and mosaicing were performed using the Regeemy Image Registration and Mosaicing (versio.2.43-RCB, DPI-INPE, São José dos Campos, São Paulo, Brazil) (Figure 1). Differences in projection geometry can be minimized by these registration procedures of images when using non-standardized panoramic radiographs (Geraets et al., 2012; Sunku et al., 2011).
Figure 1. Process of image registration and mosaicing. (A), Registered radiograph taken
immediately after implant placement; (B), Registered radiograph taken before sinus augmentation; (C), Mosaicing of 2 registered images.
Figure 2 shows the linear measurements and the 2-dimensional measurements that were obtained between landmarks.
Figure 2. (A) Linear measurements, and (B) 2-dimensional measurements that were
obtained between landmarks.
a, Length of implant: perpendicular distance from the implant shoulder to the most apical part of the fixture; b, Residual bone height: perpendicular distance from the implant shoulder to the sinus floor; c, Area of implant: 2-dimensional area of the outermost layer of the fixture in grafted area; d, Residual bone area: 2-dimensional area of the outermost layer of the fixture in native bone.
Periapical radiographs (Kodak Insight, film speed F, Rochester, NY, USA) were taken at the time of final restoration delivery (baseline) and at 12 months after functional loading (Figure 3). Radiographs were obtained (70 kV, 8 mA, 0.250 s) with an extension cone paralleling device (Extension Cone Paralleling Kit, Rinn, Elgin, IL, USA). A
5.5-mm spherical metal bearing was positioned to assist length measurement. All films were developed with the same automatic processor (Periomat, Durr Dental, Bietigheim-Bissingen, Germany), according to the manufacturer's instructions. Films were digitized with a digital scanner (EPSON GT-12000, EPSON, Nagano, Japan) at an input resolution of 2400 dpi with 256 gray scale. Measurement was taken to the nearest 0.1 mm with the Image J 1.43u software package (Wayne Rasband, National Institutes of Health, USA). To avoid the influence of dependency and to enhance the statistical accuracy, only 1 randomized implant per maxillary sinus was analyzed, regardless of the number of implants placed (Herrmann et al., 2003). The reference point was defined as the border between the polished surface and the rough surface of the fixture.
A B
Figure 3. Intraoral radiographs with a 5.5-mm spherical metal bearing taken (A)
The marginal bone levels were evaluated by measuring the distance between the reference point and the most apical point of the bone level at the mesial and distal implant surfaces (Figure 4); these values were then averaged.
Figure 4. Schematic illustration of the site and reference point measurements. A and B,
distance from the reference point to the marginal bone at the mesial and distal parts of the implant, respectively.
5. Statistical analysis
Pearson’s correlation analysis was used to test the relationship between the residual bone/implant length (RIL) ratio and MBL, and the residual bone/implant area (RIA) ratio
and MBL. The effect of type of bone (MBCP/ICB vs Bio-Oss) relative to MBL was analyzed using the Mann-Whitney test. Statistical software (SPSS for Windows, version 20.0, SPSS Inc., Chicago, IL, USA) was used to process all data. The values were considered statistically significant if the P value was less than 0.05.
We tested 2 hypotheses in our study: (1) RIL ratio and RIA ratio do not affect MBL. (2) There is no difference between the 2 groups in MBL.
III. RESULT
Between May 2010 and January 2012, 42 participants (20 men, 22 women) with a mean ± standard deviation (SD) age of 58.9 ± 9.6 years (range, 31–80 years) were selected in this 1-year retrospective study. A total of 46 implants were placed in the augmented maxillary sinuses. All patients fulfilled the follow-up criteria. None of the 42 patients experienced complications (e.g., sinus membrane perforation, infection, maxillary sinusitis, or poor wound healing). A total of 32 fixtures were placed into posterior maxillary areas augmented with MBCP combined with ICB (Group I), and 14 fixtures were placed into posterior maxillary areas augmented with Bio-Oss (Group II).
Radiography revealed that MBL varied from 0 mm to 0.43 mm after 1 year of functional loading. The mean ± SD MBL from the time of prosthesis delivery to 1 year after functional loading was 0.05 ± 0.1 mm in present study. As it is shown in Table 1, Pearson’s correlation analysis revealed that RIL ratio and RIA ratio were not associated with peri-implant MBL at 1 year after functional loading (P > .05).
Table 2 shows that implants placed in maxillary sinuses augmented with Bio-Oss resulted in slightly more MBL when compared with those placed in augmented sinuses with MBCP/ICB. However, the difference was not statistically significant (P > .05).
Table 1. Pearson’s correlation analysis between the marginal bone loss and the following
parameters; residual bone/implant length ratio, residual bone/implant area ratio (N = 46) RIL ratio RIA ratio
MBL r = 0.21, P >.05 r = 0.09, P >.05
MBL = marginal bone loss; RIL ratio = residual bone/implant length ratio; RIA ratio = residual bone/implant area ratio.
Table 2. Comparison of each peri-implant marginal bone loss in both implant groups at 1
year after functional loading
Group Number (total = 46) Mean±SD (in mm)
I 32 0.04±0.08
II 14 0.07±0.14
P-value 0.45
IV. DISCUSSION
In the present study, we investigated the influence of RIL ratio and RIA ratio on the clinical conditions of dental implants placed in augmented sinuses.
There are various opinions regarding the ideal selection of implant size (length, diameter) for functional dental rehabilitation in the posterior maxillary area with poor bone quality. Currently, due to developments of implant design and surface preparation of fixtures, small implants can be used successfully in patients with minimal bone height (Jaffin and Berman, 1991; Quirynen et al., 1992). Sinus augmentation with bone graft material makes the implant able to fixation in the severely atrophic maxilla, with the occurrence of strains in the sinus floor area (Cehreli et al., 2007). The apical portion of implant placed in augmented maxillary sinus contacts with grafted bone, and the coronal portion of implant contacts with native bone (cortical, cancellous). Consider that high-level strain occurs, which is associated with MBL, when the stiffness of grafted bone is less than that of native bone (Inglam et al., 2010), the association between the length of implant and initial native bone height seems to be significant (Fugazzotto, 2003). However, our Pearson’s correlation analysis showed that no relationship was found between RIL ratio and MBL, and RIA ratio and MBL. In this study, a xenograft (Bio-Oss) or a mixture of an allograft with an alloplastic material (MBCP/ICB) was used for maxillary sinus augmentation. In terms of histological and biological properties, these graft materials have the resorptive feature accompanied by newly formed bone (Lee et al., 2008; Valentini et al., 2000). Through these progresses, high-quality of grafted bone
improves the biomechanical function of implants as crestal bone resorption progresses (Inglam et al., 2010). In this study, the treatment of sinus augmentation with delayed implant placement that functional loading occurs at least 12 months after bone graft, may provide improvements in maturation and consolidation of the grafted area was improved. This is supported by a 3-dimensional finite element analysis that the existence of grafted bone with greater stiffness reduced the stresses in native bone (Huang et al., 2009). That analysis found that the length of the implant in grafted bone did not affect the stress in native bone, but it did affect the stress in grafted bone.
Alloplasts, allografts, and xenografts can be successfully used, either alone or mixed with other materials, to avoid the disadvantages inherent in harvesting autogenous bone (Lindgren et al., 2012; Sbordone et al., 2011; Schlegel et al., 2003; Wallace and Froum, 2003). In this study, there was no significant difference in MBL between implants placed in sinuses with MBCP/ICB grafts and those placed in sinuses with Bio-Oss grafts. This result accords with studies that have shown favorable clinical results in sinus augmentation and implant survival using alloplasts that included hydroxyapatite (HA) and beta-tricalcium phosphate (β-TCP), or deproteinized bovine bone (Cordaro et al., 2008; Lindgren et al., 2012; Nkenke and Stelzle, 2009). HA provides a scaffold on which new bone can grow, and β-TCP provides bioactivity for bone remodeling (Daculsi et al., 1989; Daculsi et al., 1990; Gauthier et al., 1998; Karabuda et al., 2001). MBCP is composed of 60% HA and 40% β-TCP (Nery et al., 1992; Yamada et al., 1997); its porosity and form allow bone to grow into the scaffold and mineralize. ICB has osteoconductive and osteoinductive properties. Because of these properties and the natural osteogenic capacity of the sinus walls, grafts containing MBCP and ICB allow
implants to be fixed into posterior maxillae that would otherwise have insufficient vertical bone height for implants (Butz and Huys, 2005; Fugazzotto and Pikos, 2001; Maiorana et al., 2005; Tadjoedin et al., 2000; Tong et al., 1998). Furthermore, Bio-Oss has been shown to have the osteoconductive property and to be highly biocompatible with oral hard tissues (Berglundh and Lindhe, 1997; Pinholt et al., 1991). By various researchers, Bio-Oss has been widely and successfully used for the treatment of osseous defects and maxillary sinus augmentation (Piattelli et al., 1999; Rodriguez et al., 2003; Yildirim et al., 2000).
All implants used in this study had a fluoride-modified TiO2-blasted surface, a
microthreaded cervical neck with internal conical seal implant-abutment connections. These elements reportedly support the preservation of marginal bone (Engquist et al., 2002; Hansson, 2000; Norton, 1998; van Steenberghe et al., 2000). Implants in our study differed in fixture design only. The fixture design was unlikely to affect our results; a recent study showed that peri-implant bone loss after 1 year of loading was no different between implants with conical and straight neck designs (Kim et al., 2010).
Ongoing MBL over time compromises the success of dental implant treatment (Quirynen et al., 1992). However, even when substantial MBL has occurred, an implant may not be lost if the bone loss does not progress. In this study, the overall amount of MBL was very small and fell within the currently accepted criteria for successful implantation: bone loss of 1 mm during the first year and not exceeding 0.2 mm annually (Albrektsson et al., 1986; Albrektsson and Zarb, 1993; Laurell and Lundgren, 2011; Roos et al., 1997).
patients and implants were unequally distributed between the 2 groups. In addition, analysis of small peri-implant marginal bone level changes and the positioning of landmarks on 2-dimensional radiographs may introduce false diagnoses (Bragger et al., 1998; Fredholm et al., 1993). These disadvantages may limit the conclusions that can be drawn from the statistical analyses. Besides, the distribution of RIL and RIA ratio was narrow in this study. Further controlled studies with larger sample sizes and longer follow-up periods after prosthesis delivery should be conducted.
V. CONCLUSION
Within the limitations of this study, our study shows that the height or area ratio of residual alveolar bone to graft material in contact with implant surface were not associated with peri-implant marginal bone loss at 1 year after functional loading in the augmented maxillary sinuses.
VI. REFERENCES
1. Adell R, Eriksson B, Lekholm U, Branemark PI, Jemt T (1990). Long-term follow-up study of osseointegrated implants in the treatment of totally edentulous jaws. Int J Oral Maxillofac Implants 5(4): 347-359.
2. Albrektsson T, Zarb G, Worthington P, Eriksson AR (1986). The long-term efficacy of currently used dental implants: a review and proposed criteria of success. Int J Oral Maxillofac Implants 1(1): 11-25.
3. Albrektsson T, Zarb GA (1993). Current interpretations of the osseointegrated response: clinical significance. Int J Prosthodont 6(2): 95-105.
4. Berglundh T, Lindhe J (1997). Healing around implants placed in bone defects treated with Bio-Oss. An experimental study in the dog. Clin Oral Implants Res 8(2): 117-124.
5. Boyne PJ, James RA (1980). Grafting of the maxillary sinus floor with autogenous marrow and bone. J Oral Surg 38(8): 613-616.
6. Bragger U, Hafeli U, Huber B, Hammerle CH, Lang NP (1998). Evaluation of postsurgical crestal bone levels adjacent to non-submerged dental implants. Clin Oral Implants Res 9(4): 218-224.
7. Butz SJ, Huys LW (2005). Long-term success of sinus augmentation using a synthetic alloplast: a 20 patients, 7 years clinical report. Implant Dent 14(1): 36-42.
8. Cehreli MC, Akkocaoglu M, Comert A, Tekdemir I, Akca K (2007). Bone strains around apically free versus grafted implants in the posterior maxilla of human cadavers. Med Biol Eng Comput 45(4): 395-402.
9. Cordaro L, Bosshardt DD, Palattella P, Rao W, Serino G, Chiapasco M (2008). Maxillary sinus grafting with Bio-Oss or Straumann Bone Ceramic: histomorphometric results from a randomized controlled multicenter clinical trial. Clin Oral Implants Res 19(8): 796-803.
10. Daculsi G, LeGeros RZ, Nery E, Lynch K, Kerebel B (1989). Transformation of biphasic calcium phosphate ceramics in vivo: ultrastructural and physicochemical characterization. J Biomed Mater Res 23(8): 883-894.
11. Daculsi G, Passuti N, Martin S, Deudon C, Legeros RZ, Raher S (1990). Macroporous calcium phosphate ceramic for long bone surgery in humans and dogs. Clinical and histological study. J Biomed Mater Res 24(3): 379-396.
12. Del Fabbro M, Testori T, Francetti L, Weinstein R (2004). Systematic review of survival rates for implants placed in the grafted maxillary sinus. Int J Periodontics Restorative Dent 24(6): 565-577.
13. Engquist B, Astrand P, Dahlgren S, Engquist E, Feldmann H, Grondahl K (2002). Marginal bone reaction to oral implants: a prospective comparative study of Astra Tech and Branemark System implants. Clin Oral Implants Res 13(1): 30-37.
14. Esposito M, Grusovin MG, Coulthard P, Thomsen P, Worthington HV (2005). A 5-year follow-up comparative analysis of the efficacy of various osseointegrated dental implant systems: a systematic review of randomized controlled clinical trials. Int J Oral Maxillofac Implants 20(4): 557-568.
15. Fredholm U, Bolin A, Andersson L (1993). Preimplant radiographic assessment of available maxillary bone support. Comparison of tomographic and panoramic technique. Swed Dent J 17(3): 103-109.
16. Fugazzotto PA (2003). Augmentation of the posterior maxilla: a proposed hierarchy of treatment selection. J Periodontol 74(11): 1682-1691.
17. Fugazzotto PA, Pikos MA (2001). Guided bone regeneration and sinus augmentation in the absence of autogenous bone grafting. Implant Dent 10(3): 158-161.
18. Galindo-Moreno P, Fauri M, Avila-Ortiz G, Fernandez-Barbero JE, Cabrera-Leon A, Sanchez-Fernandez E (2005). Influence of alcohol and tobacco habits on peri-implant marginal bone loss: a prospective study. Clin Oral Implants Res 16(5): 579-586.
19. Galindo-Moreno P, Fernandez-Jimenez A, Avila-Ortiz G, Silvestre FJ, Hernandez-Cortes P, Wang HL (2014). Marginal bone loss around implants placed in maxillary native bone or grafted sinuses: a retrospective cohort study. Clin Oral Implants Res 25(3): 378-384.
20. Gauthier O, Bouler JM, Aguado E, Pilet P, Daculsi G (1998). Macroporous biphasic calcium phosphate ceramics: influence of macropore diameter and macroporosity percentage on bone ingrowth. Biomaterials 19(1-3): 133-139.
21. Geraets WG, Verheij HG, Wismeijer D, van der Stelt PF (2012). Detecting bone loss along dental implants by subtraction of panoramic radiographs. Clin Oral Implants Res 23(7): 861-865.
22. Hansson S (2000). Implant-abutment interface: biomechanical study of flat top versus conical. Clin Implant Dent Relat Res 2(1): 33-41.
23. Herrmann I, Lekholm U, Holm S (2003). Statistical outcome of random versus selected withdrawal of dental implants. Int J Prosthodont 16(1): 25-30.
24. Huang HL, Fuh LJ, Ko CC, Hsu JT, Chen CC (2009). Biomechanical effects of a maxillary implant in the augmented sinus: a three-dimensional finite element analysis. Int J Oral Maxillofac Implants 24(3): 455-462.
25. Inglam S, Suebnukarn S, Tharanon W, Apatananon T, Sitthiseripratip K (2010). Influence of graft quality and marginal bone loss on implants placed in maxillary grafted sinus: a finite element study. Med Biol Eng Comput 48(7): 681-689.
26. Isidor F (1996). Loss of osseointegration caused by occlusal load of oral implants. A clinical and radiographic study in monkeys. Clin Oral Implants Res 7(2): 143-152.
27. Isidor F (2006). Influence of forces on peri-implant bone. Clin Oral Implants Res 17 Suppl 2: 8-18.
28. Jacobs R (2003). Preoperative radiologic planning of implant surgery in compromised patients. Periodontol 2000 33: 12-25.
29. Jaffin RA, Berman CL (1991). The excessive loss of Branemark fixtures in type IV bone: a 5-year analysis. J Periodontol 62(1): 2-4.
30. Johansson B, Wannfors K, Ekenback J, Smedberg JI, Hirsch J (1999). Implants and sinus-inlay bone grafts in a 1-stage procedure on severely atrophied maxillae: surgical aspects of a 3-year follow-up study. Int J Oral Maxillofac Implants 14(6): 811-818.
31. Karabuda C, Ozdemir O, Tosun T, Anil A, Olgac V (2001). Histological and clinical evaluation of 3 different grafting materials for sinus lifting procedure based on 8 cases. J Periodontol 72(10): 1436-1442.
32. Kim JJ, Lee DW, Kim CK, Park KH, Moon IS (2010). Effect of conical configuration of fixture on the maintenance of marginal bone level: preliminary results at 1 year of function. Clin Oral Implants Res 21(4): 439-444.
33. Laurell L, Lundgren D (2011). Marginal bone level changes at dental implants after 5 years in function: a meta-analysis. Clin Implant Dent Relat Res 13(1): 19-28.
34. Lee JH, Jung UW, Kim CS, Choi SH, Cho KS (2008). Histologic and clinical evaluation for maxillary sinus augmentation using macroporous biphasic calcium phosphate in human. Clin Oral Implants Res 19(8): 767-771.
35. Lindgren C, Mordenfeld A, Hallman M (2012). A prospective 1-year clinical and radiographic study of implants placed after maxillary sinus floor augmentation with synthetic biphasic calcium phosphate or deproteinized bovine bone. Clin Implant Dent Relat Res 14(1): 41-50.
36. Maiorana C, Sigurta D, Mirandola A, Garlini G, Santoro F (2005). Bone resorption around dental implants placed in grafted sinuses: clinical and radiologic follow-up after up to 4 years. Int J Oral Maxillofac Implants 20(2): 261-266.
37. Miyamoto I, Tsuboi Y, Wada E, Suwa H, Iizuka T (2005). Influence of cortical bone thickness and implant length on implant stability at the time of surgery--clinical, prospective, biomechanical, and imaging study. Bone 37(6): 776-780.
38. Mombelli A, van Oosten MA, Schurch E, Jr., Land NP (1987). The microbiota associated with successful or failing osseointegrated titanium implants. Oral Microbiol Immunol 2(4): 145-151.
39. Nery EB, LeGeros RZ, Lynch KL, Lee K (1992). Tissue response to biphasic calcium phosphate ceramic with different ratios of HA/βTCP in periodontal osseous defects. J Periodontol 63(9): 729-735.
40. Nkenke E, Stelzle F (2009). Clinical outcomes of sinus floor augmentation for implant placement using autogenous bone or bone substitutes: a systematic review. Clin Oral Implants Res 20 Suppl 4: 124-133.
41. Norton MR (1998). Marginal bone levels at single tooth implants with a conical fixture design. The influence of surface macro- and microstructure. Clin Oral Implants Res 9(2): 91-99.
42. Piattelli M, Favero GA, Scarano A, Orsini G, Piattelli A (1999). Bone reactions to anorganic bovine bone (Bio-Oss) used in sinus augmentation procedures: a histologic long-term report of 20 cases in humans. Int J Oral Maxillofac Implants 14(6): 835-840.
43. Pinholt EM, Bang G, Haanaes HR (1991). Alveolar ridge augmentation in rats by Bio-Oss. Scand J Dent Res 99(2): 154-161.
44. Pjetursson BE, Tan WC, Zwahlen M, Lang NP (2008). A systematic review of the success of sinus floor elevation and survival of implants inserted in combination with sinus floor elevation. J Clin Periodontol 35(8 Suppl): 216-240.
45. Quirynen M, Naert I, van Steenberghe D (1992). Fixture design and overload influence marginal bone loss and fixture success in the Branemark system. Clin Oral Implants Res 3(3): 104-111.
46. Rodriguez A, Anastassov GE, Lee H, Buchbinder D, Wettan H (2003). Maxillary sinus augmentation with deproteinated bovine bone and platelet rich plasma with simultaneous insertion of endosseous implants. J Oral Maxillofac Surg 61(2): 157-163.
47. Roos J, Sennerby L, Lekholm U, Jemt T, Grondahl K, Albrektsson T (1997). A qualitative and quantitative method for evaluating implant success: a 5-year retrospective analysis of the Branemark implant. Int J Oral Maxillofac Implants 12(4): 504-514.
48. Sbordone L, Levin L, Guidetti F, Sbordone C, Glikman A, Schwartz-Arad D (2011). Apical and marginal bone alterations around implants in maxillary sinus augmentation grafted with autogenous bone or bovine bone material and simultaneous or delayed dental implant positioning. Clin Oral Implants Res 22(5): 485-491.
49. Schlegel KA, Fichtner G, Schultze-Mosgau S, Wiltfang J (2003). Histologic findings in sinus augmentation with autogenous bone chips versus a bovine bone substitute. Int J Oral Maxillofac Implants 18(1): 53-58.
50. Sharan A, Madjar D (2008). Maxillary sinus pneumatization following extractions: a radiographic study. Int J Oral Maxillofac Implants 23(1): 48-56.
51. Smeets EC, de Jong KJ, Abraham-Inpijn L (1998). Detecting the medically compromised patient in dentistry by means of the medical risk-related history. A survey of 29,424 dental patients in The Netherlands. Prev Med 27(4): 530-535.
52. Sunku R, Roopesh R, Kancherla P, Perumalla KK, Yudhistar PV, Reddy VS (2011). Quantitative digital subtraction radiography in the assessment of external apical root resorption induced by orthodontic therapy: a retrospective study. J Contemp Dent Pract 12(6): 422-428.
53. Tadjoedin ES, de Lange GL, Holzmann PJ, Kulper L, Burger EH (2000). Histological observations on biopsies harvested following sinus floor elevation using a bioactive glass material of narrow size range. Clin Oral Implants Res 11(4): 334-344.
54. Tong DC, Rioux K, Drangsholt M, Beirne OR (1998). A review of survival rates for implants placed in grafted maxillary sinuses using meta-analysis. Int J Oral Maxillofac Implants 13(2): 175-182.
55. Valentini P, Abensur D, Wenz B, Peetz M, Schenk R (2000). Sinus grafting with porous bone mineral (Bio-Oss) for implant placement: a 5-year study on 15 patients. Int J Periodontics Restorative Dent 20(3): 245-253.
56. van Steenberghe D, De Mars G, Quirynen M, Jacobs R, Naert I (2000). A prospective split-mouth comparative study of two screw-shaped self-tapping pure titanium implant systems. Clin Oral Implants Res 11(3): 202-209.
57. Vercellotti T, De Paoli S, Nevins M (2001). The piezoelectric bony window osteotomy and sinus membrane elevation: introduction of a new technique for simplification of the sinus augmentation procedure. Int J Periodontics Restorative Dent 21(6): 561-567.
58. Wallace SS, Froum SJ (2003). Effect of maxillary sinus augmentation on the survival of endosseous dental implants. A systematic review. Ann Periodontol 8(1): 328-343.
59. Wang HL, Katranji A (2008). ABC sinus augmentation classification. Int J Periodontics Restorative Dent 28(4): 383-389.
60. Wehrbein H, Diedrich P (1992). Die fortschreitende Pneumatisation der basalen Kieferhöhle nach Extraktion und Lückenschluß. Fortschr Kieferorthop 53(2): 77-83.
61. Yamada S, Heymann D, Bouler JM, Daculsi G (1997). Osteoclastic resorption of calcium phosphate ceramics with different hydroxyapatite/beta-tricalcium phosphate ratios. Biomaterials 18(15): 1037-1041.
62. Yildirim M, Spiekermann H, Biesterfeld S, Edelhoff D (2000). Maxillary sinus augmentation using xenogenic bone substitute material Bio-Oss in combination with venous blood. A histologic and histomorphometric study in humans. Clin Oral Implants Res 11(3): 217-229.
국문요약
거상된 상악동 부위에 위치한 임플란트의 변연골 소실에 고정체 표면과
접촉한 잔존 치조골과 이식재의 비율이 미치는 영향: 1 년간 후향적
연구
<지도교수: 문 익 상, D.D.S., M.S.D., Ph.D.>
연세대학교 대학원 치의학과
박 찬 호, D.D.S
이 후향적 연구의 목적은 거상된 상악동에 지연식립된 임플란트 주위의 변연골 소실 에 잔존 치조골과 이식재의 높이 또는 면적의 비율이 미치는 영향을 알아보기 위함이 다. MBCP/ICB 또는 Bio-Oss로 이식된 상악동 부위에 식립된 Astra 임플란트를 가 진 42명의 환자가 선정되었다 (치조골 높이 ≤ 5 mm). 최종 보철물 장착시와 기능 적 부하 후 12개월째의 방사선 이미지를 통해 각 상악동당 1개의 임플란트에 대한 변연골 소실이 측정되었다. 임상 및 방사선학적 자료를 이용하여 변연골 변화를 분석 하기 위해 Pearson’s correlation analysis와 Mann-Whitney test가 시행되었다. 이 연구에는 총 46개의 임플란트가 포함되었다. 기능적 부하 후 1년째의 임플란트 주 위 변연골 소실과 residual bone/implant length ratio 및 the residual bone/implantarea ratio는 관련성을 보이지 않았다 (P > .05). 또한, 조사기간 동안 두 종류의 이 식재 내에 변연골 소실의 유의성 있는 차이는 없었다 (P > .05). 1년의 기능적 부하 기간 동안, residual bone/implant length ratio 및 the residual bone/implant area ratio는 거상된 상악동에 식립된 임플란트 주위의 변연골 소실에 영향을 미치지 않는 것으로 나타났다.
핵심 되는 말 : 상악동 거상술, 변연골 소실, 잔존골 대 임플란트 비율