저작자표시-비영리-변경금지 2.0 대한민국 이용자는 아래의 조건을 따르는 경우에 한하여 자유롭게 l 이 저작물을 복제, 배포, 전송, 전시, 공연 및 방송할 수 있습니다. 다음과 같은 조건을 따라야 합니다: l 귀하는, 이 저작물의 재이용이나 배포의 경우, 이 저작물에 적용된 이용허락조건 을 명확하게 나타내어야 합니다. l 저작권자로부터 별도의 허가를 받으면 이러한 조건들은 적용되지 않습니다. 저작권법에 따른 이용자의 권리는 위의 내용에 의하여 영향을 받지 않습니다. 이것은 이용허락규약(Legal Code)을 이해하기 쉽게 요약한 것입니다. Disclaimer 저작자표시. 귀하는 원저작자를 표시하여야 합니다. 비영리. 귀하는 이 저작물을 영리 목적으로 이용할 수 없습니다. 변경금지. 귀하는 이 저작물을 개작, 변형 또는 가공할 수 없습니다.
Cardiac autonomic and vascular endothelial
functions in Parkinson’s disease
By
Jung Han Yoon
Department of Medical Sciences
The Graduate School, Ajou University
Cardiac autonomic and vascular endothelial
functions in Parkinson’s disease
By
Jung Han Yoon
I submit this thesis as the
Doctoral thesis in Medical Sciences
February 2019
Supervised by
Ji Man Hong, M.D., Ph.D.
Department of Medical Sciences
The Graduate School, Ajou University
i
-Abstract-
Cardiac autonomic and vascular endothelial functions in
Parkinson’s disease
Cardiac autonomic function, assessed using heart rate variability (HRV) and cardiac iodine-123-meta-iodobenzylguanidine (MIBG), is altered in Parkinson’s disease (PD) patients. In addition, vascular endothelial function, as measured by flow-mediated dilation (FMD), might play a role in the pathogenesis and progression of neurodegenerative disease. However, little is known about whether cardiac autonomic function might be used in the early diagnosis of Parkinson’s disease (PD), and the extent to which such alterations contribute to the neurodegenerative process is unclear. Further, the involvement of vascular endothelial function in PD remains to be clarified. The clinical significance of cardiac autonomic function in the diagnosis and prognosis of PD and the involvement of vascular endothelial function were investigated in this study. HRV was significantly lower in early PD. Higher HRV was associated with better cognitive function. A reduction in cardiac MIBG uptake was associated with subsequent increased risk of dementia. In addition, FMD was significantly lower in PD patients, and was negatively associated with levodopa treatment. Surgical deep brain stimulation reduced levodopa administration and improved motor disability and FMD. In conclusion, cardiac autonomic dysfunction occurs early in PD and is associated with subsequent risk of developing PD-associated dementia. Vascular endothelial function is also altered in PD and appears to be affected by chronic levodopa treatment.
Keywords: Parkinson’s disease, heart rate variability, cardiac MIBG, flow-mediated dilation, cardiac autonomic function
ii
Table of Contents
Abstract………i Table of contents………ii List of Figures………iv List of Tables………..v Abbreviation………..vi I. INTRODUCTION………1 1.1. Classical pathogenesis of PD………..11.2. New Concept of Neurovascular networks in PD……….1
1.3. Cardiovascular autonomic system………1
1.4. Vascular endothelial system………..2
1.5. Aim of the study………3
II. Materials and Method………..………….4
2.1. Patients……….4
2.2. Heart rate variability (HRV)……….4
2.3. Cardiac iodine- 123-meta-iodobenzylguanidine (MIBG)……….5
2.4. Flow mediated dilation (FMD)……….5
2.5. Statistical analysis……….6
III. Results………7
3.1 Heart rate variability to differentiate PD from essential tremor (ET)…………..7
3.2 Heart rate variability in PD with and without REM sleep behavior disorder….11 3.3 Cardiac MIBG and risk of dementia PD………..14
iii
3.4. Effect of heart rate variability on cognition in PD………..20
3.5. Flow-mediated dilation in PD……….22
3.6. Endothelial dysfunction and hyperhomocysteinemia in PD………..…….24
3.7. Effect of levodopa on FMD in PD: Serial follow up study……….29
3.8. Effect of FMD on cognition in PD………31
3.9. Effect of deep brain stimulation (DBS) on FMD and HRV………...33
IV. Discussion……….36
V. Conclusion………..39
References………41
iv
List of Figures
Figure 1. Receiver operating characteristic (ROC) curves for HRV in differentiating PD from ET……….10 Figure 2. Distribution of delayed heart-to-mediastinum ratio in patients with PD………….18 Figure 3. Cumulative dementia-free survival based on delayed heart-to-mediastinum ratio..19 Figure 4. FMD in patients with PD and controls……….26 Figure 5. Relationship between FMD and homocysteine in PD ……….27 Figure 6. Correlations of FMD and cognition in PD……….32 Figure 7. Difference of HRV parameters before and after 1 year of DBS surgery……….….35 Figure 8. Proposed mechanism of cardiac autonomic and vascular endothelial dysfunction in PD……….40
v
List of Tables
Table 1. Basic demographics between PD and ET……….8
Table 2. Comparison of HRV between PD and ET ……….……….9
Table 3. Demographics between PD with and without RBD………....12
Table 4. HRV during supine and standing between PD with and without RBD………13
Table 5. Demographics of PD grouped by the delayed MIBG ratio………...15
Table 6. Baseline characteristics of non-converters and converters to dementia ….…….….16
Table 7. Progression rates to dementia by years of follow-up……….………..………..17
Table 8. Cox proportional hazards models for prediction of development of dementia.…….17
Table 9. Correlations between HRV and neurocognitive domain in PD………..…21
Table 11. Demographic characteristics of PD and controls………25
Table 12. Multivariate-adjusted odds ratios of variables associated with the lowest tertile of FMD………28
Table 13. Change of FMD and homocysteine after levodopa and dopamine agonist treatment.30 Table 14. Change of FMD and homocysteine after DBS………….………...34
vi
Abbreviation
IPD: Idiopathic Parkinson’s disease
TDPD: Tremor dominant Parkinson’s disease LBD: Lewy body disorder
RBD: Rapid eye movement (REM) sleep behavior disorder HRV: Heart rate variability
Cardiac MIBG: Cardiac Iodine- 123-meta-iodobenzylguanidine FMD: Flow mediated dilation
STN: Subthalamic nucleus DBS: Deep brain stimulation A-Syn: Alpha-synuclein
1
I. Introduction
1.1 Classical pathogenesis of PD
Idiopathic Parkinson’s disease (PD) is the second most common neurodegenerative disorder, and no effective disease-modifying or neuroprotective agents have been developed. What drives selective and progressive neuronal dysfunction and loss, the hallmark of neurodegeneration, remains unclear. Neurodegeneration does not occur in isolation, but is believed to result from various chronic insults such as exposure to neurotoxic materials, dysfunction of mitochondria, astrocytes and microglia, and accumulation of abnormal proteins [1-3]. The modification of any of these factors could be a viable therapeutic target in the treatment of PD.
1.2. New concept: neurovascular networks in PD
Recently, there has been increased interest in neurovascular networks, which are likely to interact with the neurodegenerative process in PD [4-9]. Neurovascular factors can be divided into (1) the cardiovascular autonomic system, which plays an important role in modulating systemic blood flow to the brain, and (2) vascular endothelial function, which is crucial in the regulation of cerebral blood flow.
1.3. Cardiovascular autonomic system
Cardiac autonomic dysfunction occurs early in Lewy body disorders (LBD) including PD, dementia with Lewy bodies (DLB), and REM sleep behavior disorder (RBD; a well-known precursor to LBD), reflecting the early accumulation of lewy bodies in cardiac sympathetic postganglionic nerves [10].
Heart rate variability (HRV), as determined by electrocardiography (ECG), is a simple and noninvasive method used to investigate cardiac autonomic abnormalities [11]. More sophisticated HRV analyses, including time, frequency domain and nonlinear analyses, have been shown to detect early autonomic involvement in several neurological disorders.
2
HRV is reduced in PD and DLB [12-14], and is associated with RBD. It can predict diagnosis of PD in the elderly [15-17], suggesting that cardiac autonomic dysfunction occurs during the pre-motor symptom stage of PD.
In addition, there is increasing awareness regarding the association between cognitive decline and HRV [18]. Impaired HRV could lead to blood pressure dysregulation or orthostatic hypotension, causing cerebral hypoperfusion that contributes to cognitive decline [19-21]. Vice versa, neurodegenerative processes itself could affect cardiac autonomic dysfunction [22].
Cardiac iodine-123-meta-iodobenzylguanidine (MIBG) uptake can reveal postganglionic
presynaptic cardiac sympathetic denervation caused by Lewy bodies [23], and reduced uptake of MIBG may be associated with various non-motor symptoms of PD including cognition, orthostatic hypotension, hyposmia, and RBD [24-27].In addition, impaired cardiac sympathetic innervation could be related to orthostatic hypotension in PD, which may also affect cognition [28-30].
1.4 The vascular endothelial system
The ‘vascular hypothesis' of PD proposes a key role of neurovascular changes in neuronal dysfunction and loss [31] and has recently gained much momentum. Several clinical studies have identified conventional vascular factors (e.g.; white matter lesions, stroke, diabetes mellitus, arterial stiffness) as contributors to neurodegenerative processes such as AD and PD [32-37]. However, these factors may be less sensitive to subtle neurovascular alterations.
As such, vascular endothelial function may play a role in the pathogenesis and progression of neurodegenerative diseases such as AD and PD. [4,6,31,38,39]. Vascular endothelial dysfunction is known to be one of the earliest pathological changes observed in atherosclerosis. In addition, endothelial cells have an important role in the selective permeability of molecules entering the brain from the bloodstream. This selectivity is essential to the protection and optimal performance of the brain in normal physiological conditions [6]. Endothelial dysfunction and blood-brain barrier breakdown have previously been reported in PD [40-45].
3
represents endothelium-dependent relaxation of the brachial artery in response to reactive hyperemia [46]. FMD reflects overall endothelial function throughout the vasculature [47] and has been associated with cognitive function, task-related brain activation and white matter changes [48-50]. In addition, nitric oxide, which regulates endothelial dilation in FMD, plays an important role in the regulation of cerebral circulation. Inhibition of nitric oxide release has been associated with reduced basal cerebral blood flow in humans [51].
However, little is known about whether cardiac autonomic function might be advantageous in the early diagnosis of PD, and the extent to which such alterations might contribute to the neurodegenerative process is unclear. Further, the degree and mechanism of vascular endothelial dysfunction remains to be clarified in PD. Therefore, the clinical significance of cardiac autonomic function in early diagnosis and prognosis of PD, and the involvement of vascular endothelial function were investigated in this study.
1.5 Study aims
This study investigated (1) HRV in patients with early PD, focusing on early differentiation from other similar conditions; (2) HRV in patients with PD; (3) the prognostic role of cardiac MIBG uptake in predicting dementia in de novo PD; (4) FMD in early PD and its association with levodopa treatment; (5) the effects of HRV and FMD on cognition and motor symptoms; and (6) the effect of deep brain stimulation on HRV and FMD in PD.
4
II. Materials and Method
2.1. Patients
PD was diagnosed according to the UK Brain Bank Criteria. Parkinsonian motor symptoms were assessed using the Unified PD Rating Scale Part III (UPDRS-III) while patients were in the ‘‘on’’ state. Healthy elderly volunteers who had no active neurological disorders were recruited from among the participants of our previous study or were healthy relatives of patients with movement disorders or dementia. Data on age and sex, medication history (antihypertensive agents, anti-hypoglycemic agents, antiplatelet agents, and statins), smoking history, lipid profiles, body mass index (BMI, kg/m2), homocysteine and high-sensitivity C-reactive protein levels were obtained for all participants. The exclusion criteria were as follows: (1) vascular parkinsonism, parkinsonian plus syndromes, and presentation of PD dementia; (2) medical conditions known to affect HRV, MIBG, and/or FMD, including renal insufficiency and symptomatic vascular diseases such as stroke and myocardial infarction. A battery of clinical scales was administered, including the Montreal Cognitive Assessment and the Seoul Neuropsychological Screening Battery (SNSB) [52].
2.2. Heart rate variability (HRV)
All subjects were informed to avoid alcohol or caffeine after 10 p.m. (22:00) on the night before the HRV. HRV was measured between 8 a.m. and noon using the SA-2000E model (Medicore, Seoul, Korea) [53]. Each patient or control was supine,During the 5 min measurement, the subject was asked to breathe at their usual rate. TP is the variance of the normal-to-normal interval (NN) over a temporal segment. The LF/HF ratio reflects sympatho-vagal balance or sympathetic modulation. The standard deviation of the normal-to-normal interval (SDNN), used to estimate the long-term components of the HRV, was calculated by statistical time domain measurements. The root mean square difference of successive RR intervals (RMSSD) was also calculated based on statistical time domain measurements. Power distribution across frequencies in the RR interval signal was obtained using power spectral density. Frequency domain analysis of HRV was performed with a nonparametric fast Fourier transforms technique, a commonly used mathematical approach for transforming time-dependent signals (e.g.; RR intervals) to the frequency domain. Powers in the 3 frequency bands of
5
HRV, very low frequency (VLF: 0–0.04 Hz), low frequency (LF: 0.04– 0.15 Hz), and high frequency (HF: 0.15–0.4 Hz), and total spectral power were obtained. This software has been acknowledged as the first developer of eastern reference for HRV in the world. Clinical HRV data were collected from 3,600 people from 8 university hospitals in Korea. HRV oriental reference was patented by the Korean Industrial Property Office in 2005.
2.3. Cardiac iodine- 123-meta-iodobenzylguanidine (MIBG)
123I-MIBG (111 mBq) was injected intravenously and cardiac uptake was imaged for 30 min (early) and 3 h (late) using a dual-head Camera system (MultiSPECT III, Siemens Medical Systems, Inc., Iselin, NJ, USA). MIBG uptake was assessed using the ratio of uptake in the heart and the mediastinum (H/M).
2.4. Flow mediated dilation (FMD)
Endothelial function was evaluated by the measurement of FMD at the brachial artery in response to hyperemia. All imaging was performed by an experienced sonographer. Brachial artery ultrasound imaging was performed with a 10- to 12-MHz broadband linear-array transducer and a Logiq S6 ultrasonographic system (GE Healthcare, Waukesha, WI, USA). A blood pressure cuff was placed on the forearm. Occlusion was created by inflating the cuff to at least 50 mmHg above the subject’s systolic pressure for 5 min. The pressure was then released quickly to induce hand and forearm hyperemia and subsequent brachial artery reactive vasodilation. The procedure was performed twice within a 30 min interval, while the brachial artery was scanned in cross-section. M-mode tracings from 10 sec before the inflation of the pressure cuff to 90 sec after cuff deflation were recorded. An independent observer measured the minimum (systolic) and maximum (diastolic) diameter of the brachial artery by visually identifying arterial walls in the M-mode and B mode images acquired 10 sec before the inflation and every 10 sec until recording was complete. Individual images were presented to this observer in random order without any indication of patient or timing. FMD was defined as the maximum percent change in brachial artery diameter after reactive hyperemia compared to baseline.
6
2.5 Statistical analysis
Mann–Whitney and Fisher’s exact tests were used to compare categorical and continuous variables between groups. Kruskal–Wallis tests were used to compare continuous variables among groups, followed by Mann–Whitney tests in the case of significance. To determine whether there was a relationship between HRV, FMD and variables pertaining to demographic characteristics, Spearman’s correlation coefficients were obtained. Independent t-tests or one-way analyses of variance (ANOVA) followed by post-hoc Bonferroni comparisons were used to compare groups, and Pearson’s v2 test was used to compare the frequency of categorical variables. A univariate analysis of covariance (ANCOVA), with age, gender, and education considered as covariates, was performed to compare neuropsychological scores. Main effects and interactions were tested at a critical level of a=0.05. Partial correlations between HRV parameters and neurocognitive test scores were examined using age, gender, and education as confounders. To avoid an inflated likelihood of error from multiple comparisons in correlation analyses, p-values were adjusted accordingly. Statistical analyses were performed using commercially available software (SPSS, ver. 18.0); p-values < 0.05 were considered statistically significant.
7
III. Results
3.1. Heart rate variability to differentiate essential tremor from early-stage
tremor-dominant Parkinson's disease
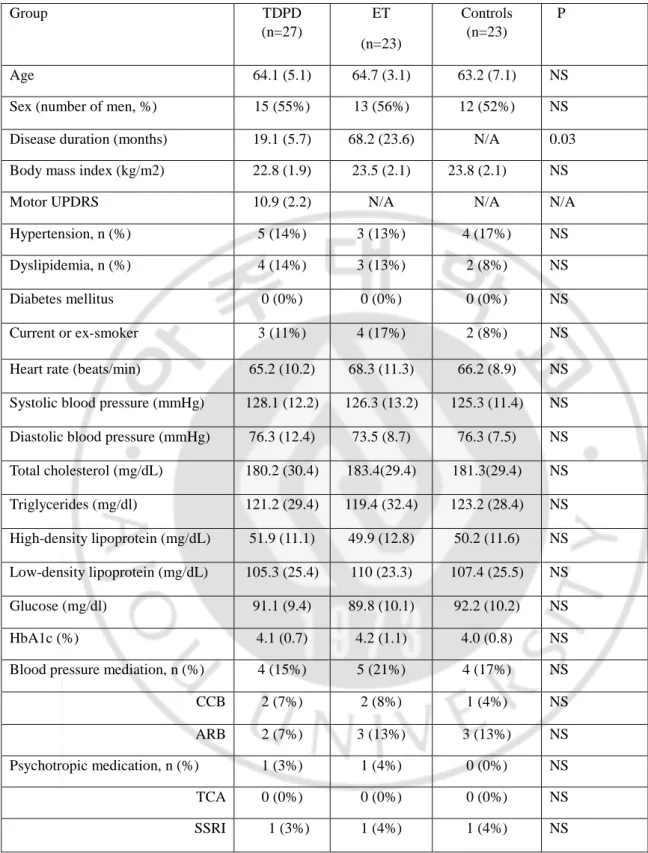
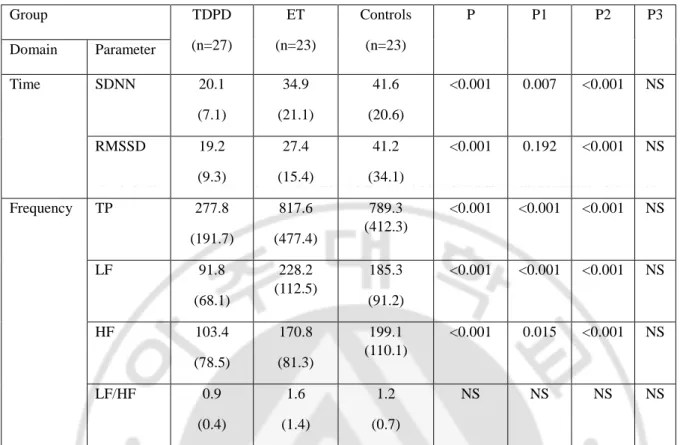
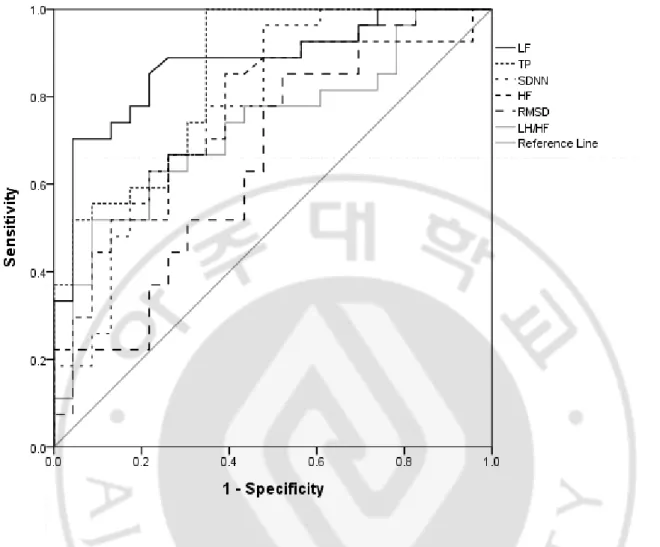
Twenty-three patients with essential tremor (ET), 27 patients with tremor-dominant PD (TDPD), and 23 healthy controls were enrolled. The demographic data and clinical characteristics of participants are summarized in Table 1. There were no differences among the groups with respect to age, sex, or past medical history. A comparison of the HRV data of patients is presented in Table 2. After adjusting for age and sex, the TDPD group showed significant and severe reductions in all time and frequency domain parameters compared to the ET group, except for in RMSSD and the LF/HF ratio. The differences were especially evident in the SDNN and the TP, LF components (Table 2). By contrast, there were no significant differences between the ET and control groups. HRV parameters did not correlate with age or disease duration in any group. Comparative receiver operating characteristic (ROC) curves for HRV parameters differentiating the TDPD group from the ET group are presented in Figure 1. ROC area under the curve (AUC) analysis revealed that LF was the best diagnostic marker (AUC=0.87) compared to TP (0.85), SDNN (0.78), HF (0.75), LF/HF ratio (0.72), and RMSSD (0.65).
8
Table 1. Basic demographics
Group TDPD (n=27) ET (n=23) Controls (n=23) P Age 64.1 (5.1) 64.7 (3.1) 63.2 (7.1) NS
Sex (number of men, %) 15 (55%) 13 (56%) 12 (52%) NS
Disease duration (months) 19.1 (5.7) 68.2 (23.6) N/A 0.03 Body mass index (kg/m2) 22.8 (1.9) 23.5 (2.1) 23.8 (2.1) NS
Motor UPDRS 10.9 (2.2) N/A N/A N/A
Hypertension, n (%) 5 (14%) 3 (13%) 4 (17%) NS
Dyslipidemia, n (%) 4 (14%) 3 (13%) 2 (8%) NS
Diabetes mellitus 0 (0%) 0 (0%) 0 (0%) NS
Current or ex-smoker 3 (11%) 4 (17%) 2 (8%) NS
Heart rate (beats/min) 65.2 (10.2) 68.3 (11.3) 66.2 (8.9) NS Systolic blood pressure (mmHg) 128.1 (12.2) 126.3 (13.2) 125.3 (11.4) NS Diastolic blood pressure (mmHg) 76.3 (12.4) 73.5 (8.7) 76.3 (7.5) NS Total cholesterol (mg/dL) 180.2 (30.4) 183.4(29.4) 181.3(29.4) NS Triglycerides (mg/dl) 121.2 (29.4) 119.4 (32.4) 123.2 (28.4) NS High-density lipoprotein (mg/dL) 51.9 (11.1) 49.9 (12.8) 50.2 (11.6) NS Low-density lipoprotein (mg/dL) 105.3 (25.4) 110 (23.3) 107.4 (25.5) NS Glucose (mg/dl) 91.1 (9.4) 89.8 (10.1) 92.2 (10.2) NS HbA1c (%) 4.1 (0.7) 4.2 (1.1) 4.0 (0.8) NS
Blood pressure mediation, n (%) 4 (15%) 5 (21%) 4 (17%) NS
CCB 2 (7%) 2 (8%) 1 (4%) NS
ARB 2 (7%) 3 (13%) 3 (13%) NS
Psychotropic medication, n (%) 1 (3%) 1 (4%) 0 (0%) NS
TCA 0 (0%) 0 (0%) 0 (0%) NS
SSRI 1 (3%) 1 (4%) 1 (4%) NS
Values are expressed as mean (SD). UPDRS, Unified Parkinson’s disease rating scale; CCB, Calcium channel blocker; ARB, angiotensin II receptor blocker; TCA, tricyclic antidepressant; SSRI, selective serotonin reuptake inhibitor.
9
Table 2. Parameters of heart rate variability between groups
Values are expressed as mean (SD). P, comparison among three groups; P1, comparison between TDPD and ET; P2, comparison between TDPD and controls; P3, comparison between ET and controls. SDNN, standard deviation of the normal-to-normal RR interval; RMSSD, root mean square difference between successive RR intervals; TP, total spectral power; LF, low frequency; HF, high frequency.
Group TDPD (n=27) ET (n=23) Controls (n=23) P P1 P2 P3 Domain Parameter Time SDNN 20.1 (7.1) 34.9 (21.1) 41.6 (20.6) <0.001 0.007 <0.001 NS RMSSD 19.2 (9.3) 27.4 (15.4) 41.2 (34.1) <0.001 0.192 <0.001 NS Frequency TP 277.8 (191.7) 817.6 (477.4) 789.3 (412.3) <0.001 <0.001 <0.001 NS LF 91.8 (68.1) 228.2 (112.5) 185.3 (91.2) <0.001 <0.001 <0.001 NS HF 103.4 (78.5) 170.8 (81.3) 199.1 (110.1) <0.001 0.015 <0.001 NS LF/HF 0.9 (0.4) 1.6 (1.4) 1.2 (0.7) NS NS NS NS
10
Figure 1. Comparison of receiver operating characteristic (ROC) curves for HRV parameters differentiating
the TDPD group from the ET group. ROC area under the curve (AUC) analysis revealed that LF was the best potential diagnostic marker (AUC = 0.87), compared to TP (0.85), SDNN (0.78), HF (0.75), LF/HF ratio (0.72), and RMSSD (0.65). SDNN, standard deviation of the normal-to-normal RR interval; RMSSD, root mean square difference between successive RR intervals; TP, total spectral power; LF, low frequency; HF, high frequency.
11
3.2. Heart rate variability in PD with and without RBD
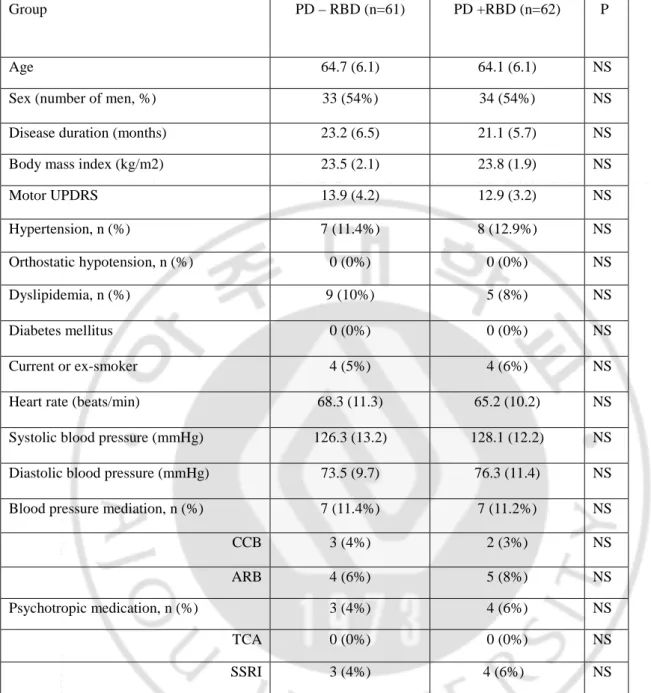
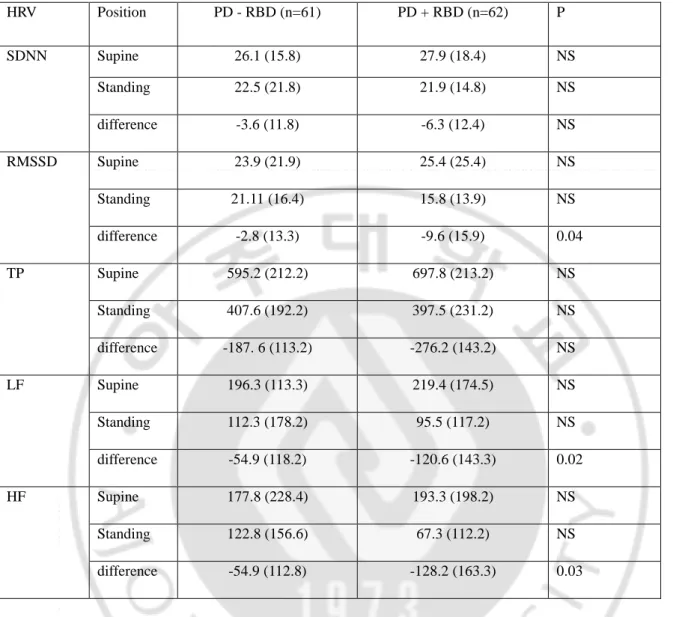
Sixty-one PD patients with RBD (PD+RBD), and an equal number of age and sex-matched PD patients without RBD (PD-RBD), were included in the analysis (Table 3). HRV responses at supine rest and during head up tilt (HUT) in the time and frequency domains were analyzed. PD+RBD patient showed no difference in all HRV parameters at supine rest compared to PD-RBD. In response to HUT, PD+RBD patients showed a blunted response in the low-frequency (LF; -120.6 vs. -84.6, p < 0.05) and high-frequency (HF; -128.3 vs. -54.9, p < 0.05) components compared to PD-RBD patients (Table 4).
12
Table 3. Basic demographics between PD with and without RBD
Group PD – RBD (n=61) PD +RBD (n=62) P
Age 64.7 (6.1) 64.1 (6.1) NS
Sex (number of men, %) 33 (54%) 34 (54%) NS
Disease duration (months) 23.2 (6.5) 21.1 (5.7) NS
Body mass index (kg/m2) 23.5 (2.1) 23.8 (1.9) NS
Motor UPDRS 13.9 (4.2) 12.9 (3.2) NS Hypertension, n (%) 7 (11.4%) 8 (12.9%) NS Orthostatic hypotension, n (%) 0 (0%) 0 (0%) NS Dyslipidemia, n (%) 9 (10%) 5 (8%) NS Diabetes mellitus 0 (0%) 0 (0%) NS Current or ex-smoker 4 (5%) 4 (6%) NS
Heart rate (beats/min) 68.3 (11.3) 65.2 (10.2) NS
Systolic blood pressure (mmHg) 126.3 (13.2) 128.1 (12.2) NS
Diastolic blood pressure (mmHg) 73.5 (9.7) 76.3 (11.4) NS
Blood pressure mediation, n (%) 7 (11.4%) 7 (11.2%) NS
CCB 3 (4%) 2 (3%) NS
ARB 4 (6%) 5 (8%) NS
Psychotropic medication, n (%) 3 (4%) 4 (6%) NS
TCA 0 (0%) 0 (0%) NS
SSRI 3 (4%) 4 (6%) NS
Values are expressed as mean (SD). UPDRS, Unified Parkinson’s disease rating scale; CCB, Calcium channel blocker, ARBs, angiotensin II receptor blockers; TCA, tricyclic antidepressant; SSRIs, selective serotonin reuptake inhibitors.
13
Table 4. Heart rate variability during supine and standing in PD patients with and without RBD
.
SDNN, standard deviation of the normal-to-normal RR interval; RMSSD, root mean square difference between successive RR intervals; TP, total spectral power; LF, low frequency; HF, high frequency.
HRV Position PD - RBD (n=61) PD + RBD (n=62) P SDNN Supine 26.1 (15.8) 27.9 (18.4) NS Standing 22.5 (21.8) 21.9 (14.8) NS difference -3.6 (11.8) -6.3 (12.4) NS RMSSD Supine 23.9 (21.9) 25.4 (25.4) NS Standing 21.11 (16.4) 15.8 (13.9) NS difference -2.8 (13.3) -9.6 (15.9) 0.04 TP Supine 595.2 (212.2) 697.8 (213.2) NS Standing 407.6 (192.2) 397.5 (231.2) NS difference -187. 6 (113.2) -276.2 (143.2) NS LF Supine 196.3 (113.3) 219.4 (174.5) NS Standing 112.3 (178.2) 95.5 (117.2) NS difference -54.9 (118.2) -120.6 (143.3) 0.02 HF Supine 177.8 (228.4) 193.3 (198.2) NS Standing 122.8 (156.6) 67.3 (112.2) NS difference -54.9 (112.8) -128.2 (163.3) 0.03
14
3.3 Cardiac MIBG and risk of dementia in PD
A total ninety-three drug-naive patients with de novo PD who underwent cardiac MIBG scanning on baseline evaluation. Patients were stratified to low MIBG (L-MIBG) and high MIBG (H-MIBG) uptake groups using the distribution of delayed H/M ratios (cutoff, 1.35, median value; Figure 2)
The patients visited our outpatient clinic every 2–6 months and were followed-up for a minimum of 4 years from the time they began taking dopaminergic medication. The predictive powers of cardiac MIBG value regarding the risk of development of dementia were assessed using Cox's proportional hazard models.
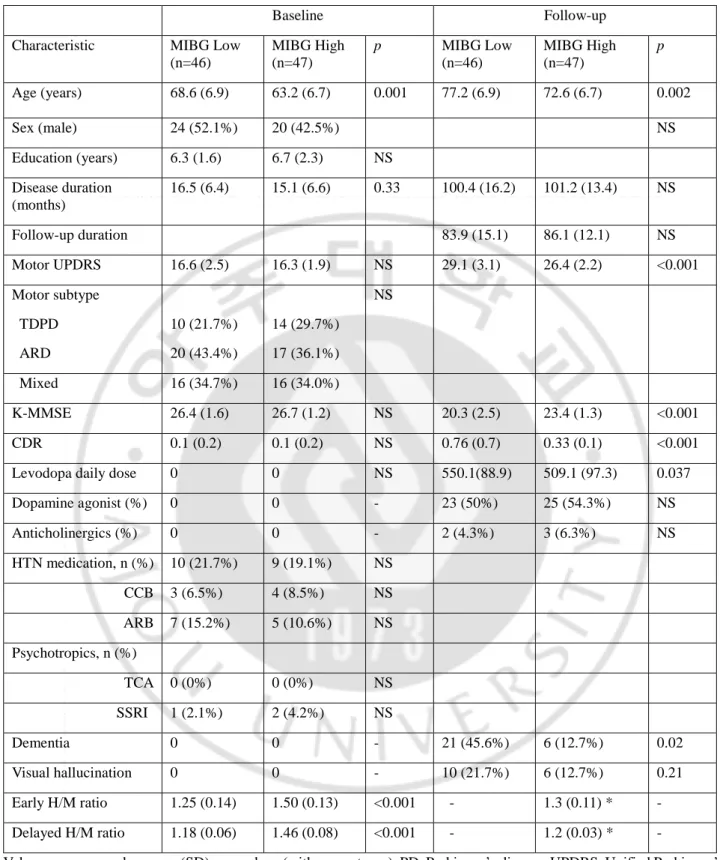
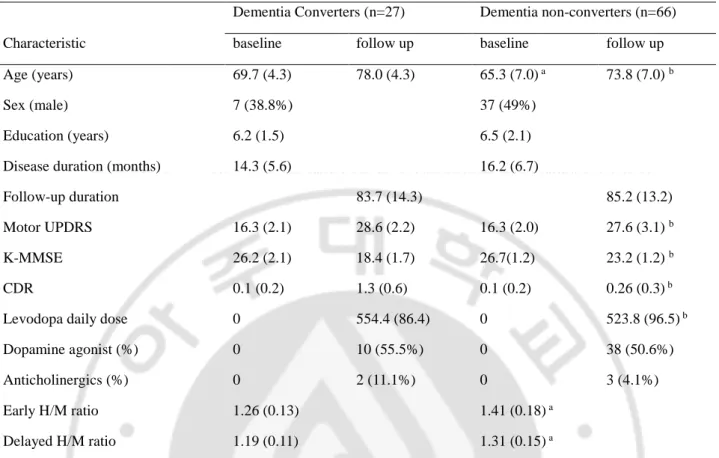
The baseline characteristics of patients at baseline and on follow-up are provided in Table 5. At baseline, there was no significant difference in regarding to gender, PD severity (UPDRS), general cognition test (Mini-mental status exam (MMSE), Clinical dementia rating (CDR)) between patients with MIBG and H-MIBG. As expected, mean patient age was lower in the H-MIBG than in the L-MIBG group. Tremor dominant PD patients exhibited a slightly higher L-MIBG uptake (1.37 ± 0.14) than akinetic rigid (1.30 ± 0.15) or mixed type patients (1.31 ± 0.16), although there was no significant difference between groups (p=0.236). On follow-up, the L-MIBG group exhibited faster motor and cognition progression and a higher levodopa equivalent dose requirement than the H-MIBG group (Table 5). Dementia (45.6% vs 12.7%, p=0.02) and visual hallucinations (21.7% vs 12.7%, p=0.21) were more frequent in the L-MIBG than in the H-MIBG group (Table 5). During a mean follow-up time of 6.7 years, 27 of 93 patients with PD (29.0%) developed dementia. Such patients were older (69.7 vs. 65.3 years) and had lower MIBG uptakes (1.19 vs 1.31) than those without dementia (Table 6).
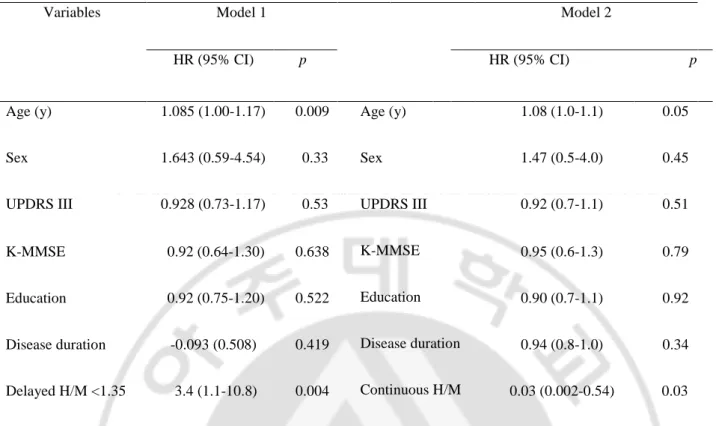
Cox’s proportional hazard modeling demonstrated that low MIBG uptake (H/M ratio<1.35) (hazard ratio [HR] 3.40; p=0.004) and age (HR 1.083, p=0.009) were strong predictors of risk for development of dementia (Model 1, Table 8). In model 2, higher MIBG uptake (controlled for age, gender and UPDRS III) was associated with a lower risk of developing dementia (HR 0.03; 95% CI; 0.002-0.54 p=0.03; Table 8).
In 10 patients who underwent serial MIBG scanning (mean scan interval, 44.9 ± 5.5 months), delayed MIBG declined from 1.51 ± 0.10 to 1.23 ± 0.03. The mean decline in the delayed H/M ratio was 0.28 (± 0.09), which was statistically significant.
15
Table 5. Demographic characteristics of PD patients grouped by delayed MIBG ratio (cutoff = 1.35).
Baseline Follow-up
Characteristic MIBG Low (n=46) MIBG High (n=47) p MIBG Low (n=46) MIBG High (n=47) p Age (years) 68.6 (6.9) 63.2 (6.7) 0.001 77.2 (6.9) 72.6 (6.7) 0.002 Sex (male) 24 (52.1%) 20 (42.5%) NS Education (years) 6.3 (1.6) 6.7 (2.3) NS Disease duration (months) 16.5 (6.4) 15.1 (6.6) 0.33 100.4 (16.2) 101.2 (13.4) NS Follow-up duration 83.9 (15.1) 86.1 (12.1) NS Motor UPDRS 16.6 (2.5) 16.3 (1.9) NS 29.1 (3.1) 26.4 (2.2) <0.001 Motor subtype TDPD ARD 10 (21.7%) 20 (43.4%) 14 (29.7%) 17 (36.1%) NS Mixed 16 (34.7%) 16 (34.0%) K-MMSE 26.4 (1.6) 26.7 (1.2) NS 20.3 (2.5) 23.4 (1.3) <0.001 CDR 0.1 (0.2) 0.1 (0.2) NS 0.76 (0.7) 0.33 (0.1) <0.001
Levodopa daily dose 0 0 NS 550.1(88.9) 509.1 (97.3) 0.037
Dopamine agonist (%) 0 0 - 23 (50%) 25 (54.3%) NS Anticholinergics (%) 0 0 - 2 (4.3%) 3 (6.3%) NS HTN medication, n (%) 10 (21.7%) 9 (19.1%) NS CCB 3 (6.5%) 4 (8.5%) NS ARB 7 (15.2%) 5 (10.6%) NS Psychotropics, n (%) TCA 0 (0%) 0 (0%) NS SSRI 1 (2.1%) 2 (4.2%) NS Dementia 0 0 - 21 (45.6%) 6 (12.7%) 0.02 Visual hallucination 0 0 - 10 (21.7%) 6 (12.7%) 0.21 Early H/M ratio 1.25 (0.14) 1.50 (0.13) <0.001 - 1.3 (0.11) * - Delayed H/M ratio 1.18 (0.06) 1.46 (0.08) <0.001 - 1.2 (0.03) * -
Values are expressed as mean (SD) or numbers (with percentages). PD, Parkinson’s disease; UPDRS, Unified Parkinson’s disease rating scale; TDPD, Tremor-dominant PD; ARD, akinetic-rigid dominant PD; K-MMSE, Korean Mini-Mental State Examination; CDR, Clinical dementia rating; HTN, Hypertension; CCB, Calcium channel blocker, ARB, angiotensin II receptor blocker; TCA, tricyclic antidepressant; SSRIs, selective serotonin reuptake inhibitors. *Follow-up MIBG data were available for 10/46 of the group with high MIBG.
16
Table 6. Baseline background characteristics of non-converters and converters to dementia associated with
Parkinson’s disease
Dementia Converters (n=27) Dementia non-converters (n=66)
Characteristic baseline follow up baseline follow up
Age (years) 69.7 (4.3) 78.0 (4.3) 65.3 (7.0) a 73.8 (7.0) b
Sex (male) 7 (38.8%) 37 (49%)
Education (years) 6.2 (1.5) 6.5 (2.1)
Disease duration (months) 14.3 (5.6) 16.2 (6.7)
Follow-up duration 83.7 (14.3) 85.2 (13.2)
Motor UPDRS 16.3 (2.1) 28.6 (2.2) 16.3 (2.0) 27.6 (3.1) b
K-MMSE 26.2 (2.1) 18.4 (1.7) 26.7(1.2) 23.2 (1.2) b
CDR 0.1 (0.2) 1.3 (0.6) 0.1 (0.2) 0.26 (0.3) b
Levodopa daily dose 0 554.4 (86.4) 0 523.8 (96.5) b
Dopamine agonist (%) 0 10 (55.5%) 0 38 (50.6%)
Anticholinergics (%) 0 2 (11.1%) 0 3 (4.1%)
Early H/M ratio 1.26 (0.13) 1.41 (0.18) a
Delayed H/M ratio 1.19 (0.11) 1.31 (0.15) a
Values are expressed as mean (SD) or numbers (with percentages). PD, Parkinson’s disease; UPDRS, Unified Parkinson’s Disease Rating Scale; MMSE, Mini-mental status exam; CDR, Clinical dementia rating. a Significant difference between
converters and non-converters at baseline at p< 0.05. b Significant difference between converters and non-converters at
17
Table 8. Cox proportional hazards models for prediction of the time to development of dementia
Variables Model 1 Model 2
HR (95% CI) p HR (95% CI) p
Age (y) 1.085 (1.00-1.17) 0.009 Age (y)
Sex UPDRS III K-MMSE Education Disease duration Continuous H/M 1.08 (1.0-1.1) 0.05 Sex 1.643 (0.59-4.54) 0.33 1.47 (0.5-4.0) 0.45 UPDRS III 0.928 (0.73-1.17) 0.53 0.92 (0.7-1.1) 0.51 K-MMSE 0.92 (0.64-1.30) 0.638 0.95 (0.6-1.3) 0.79 Education 0.92 (0.75-1.20) 0.522 0.90 (0.7-1.1) 0.92 Disease duration -0.093 (0.508) 0.419 0.94 (0.8-1.0) 0.34 Delayed H/M <1.35 3.4 (1.1-10.8) 0.004 0.03 (0.002-0.54) 0.03
UPDRS, unified Parkinson’s disease rating scale. K-MMSE, Korean mini mental state examination; H/M, heart-to-mediastinum ratio. aModel 1 was adjusted for age, sex, UPDRS III, K-MMSE, education, disease duration, delayed H/M
ratio<1.35. bModel 2 was adjusted for age, sex, UPDRS III, K-MMSE, education, disease duration, and continuous
18
Figure 2. Distribution of delayed heart-to-mediastinum ratio in patients with Parkinson's disease. Bars indicate cut-off values of delayed H/M ratio (1.35) based on the distribution of delayed heart-to-mediastinum ratios. Dark circles indicate those who progressed to dementia during follow-up.
19
20
3.4. Effect of heart rate variability on cognition in PD
A total of 91 dementia-free PD patients were enrolled. In HRV, some frontal domain scores were positively correlated with time and frequency domains. However, given the large number of comparisons (17 cognition battery * 6 HRV parameters = 102), the results did not survive multiple comparison corrections (a = 0.0004 [(0.05/ (17 * 6)]). Memory performance (verbal and visual) was not correlated with overall HRV parameters (Table 9).
21
Table 9. Correlations between HRV data and neurocognitive domain in PD.
SDNN RMSSD TP LF HF LF/HF
r r r r r r
Digit span, forward -0.044 -0.047 -0.078 0.027 -0.036 0.147
Digit span, backward 0.146 0.172 0.065 0.098 0.187 -0.076
K-BNT 0.119 0.064 0.058 0.116 0.016 0.116 Repetition 0.047 0.068 0.002 0.105 0.093 0.066 Calculation 0.148 0.150 -0.016 0.061 0.058 0.006 RCFT 0.146 0.148 0.154 0.175 0.161 0.050 SVLT, Free recall 0.013 -0.072 -0.009 0.177 -0.011 0.123 SVLT, Delayed recall 0.001 -0.145 -0.107 0.129 -0.097 0.196 SVLT, Recognition -0.120 -0.218 -0.083 0.139 -0.116 0.165 RCFT, Immediate recall 0.005 -0.016 -0.048 0.006 -0.016 -0.037 RCFT, Delayed recall -0.01 -0.048 0.006 -0.016 -0.037 -0.037 RCFT, Recognition 0.092 0.101 0.129 0.068 0.090 0.008
Phonemic generative naming 0.315 0.460 0.405 0.970 0.999 0.624
COWAT, animal 0.194 0.146 0.200 0.155 0.210 -0.065
COWAT, supermarket 0.409** 0.285** 0.208* 0.086 0.205 -0.101
Stroop Word test -0.013 -0.030 -0.019 0.120 0.026 0.088
Stroop Color test 0.226* 0.204* 0.192 0.154 0.196 -0.083
SDNN, standard deviation of the normal-to-normal RR interval; RMSSD, root mean square difference between successive RR intervals; TP, total spectral power; LF, low frequency; HF, high frequency; K-BNT, Korean version of boston naming test; RCFT, Rey Complex Figure Test; SVLT, Seoul Verbal Learning Test; COWAT, Controlled Oral Word Association Test; * p < 0.05; ** p < 0.01; Correlation did not survive multiple comparisons corrections (α = 0.0004 [(0.05/ (102]).
22
3.5. Flow-mediated dilation in PD
Eighty-one patients with early PD and 52 healthy controls were enrolled, and endothelial function was measured using FMD. The demographic characteristics of the PD patients and normal controls are summarized in Table 10. No significant differences in age, cardiovascular disease risk factors, smoking, or BMI were observed between the PD patients and controls. FMD was significantly lower in PD patients (7.1 ± 1.8%) compared with controls (8.1 ± 2.1%, p=0.02; Table 10).
23
Table 10. Demographic characteristics of patients with Parkinson’s disease and controls
Characteristic PD-patients (n=81) Controls (n=52) p
Age (y) 67.4 (8.1) 68.7 (6.7) NS
Sex (number of men, %) 38 (46.9%) 25 (48.1%) NS
Disease duration (mo) 33.9 (13.4)
UPDRS III 17.4 (4.6)
Body mass index (kg/m2) 23.8 (2.2) 23.5 (1.7) NS
Systolic blood pressure (mmHg) 133.5 (14.3) 134.5 (13.5) NS
Diastolic blood pressure (mmHg) 75.5 (11.2) 74.1 (10.1) NS
Smoking history 4 (10.0%) 3 (10.0%) NS Hypertension 20 (24.7%) 19 (36.5%) NS Diabetes mellitus 12 (14.8%) 10 (19.2%) NS Dyslipidemia 13 (16.0%) 9 (17.3%) NS C-reactive protein (mg/dl) 0.12 (0.19) 0.08 (0.11) NS Homocysteine (µmol/L) 12.6 (4.5) 11.9 (3.1) NS FMD (%) 7.1 (1.8) 8.1 (2.1) 0.02
Values are expressed as mean (SD) or numbers (%). UPDRS, unified Parkinson’s disease rating scale; FMD, flow-mediated dilation; NS, not significant.
24
3.6. Endothelial dysfunction and hyperhomocysteinemia
Forty PD patients treated with levodopa, 33 PD patients treated with levodopa/entacapone, 22 untreated PD patients, and 30 controls were enrolled, and FMD was compared between groups. The demographic characteristics of the groups are summarized in Table 11. No significant differences in age, sex, medication use, smoking, or BMI were found among groups. Among patients with PD, disease duration was significantly lower in the untreated group, and the daily levodopa dose was significantly higher in the levodopa treatment group.
FMD was significantly lower in PD patients with levodopa (6.0 ± 1.8%) compared to the levodopa/entacapone treatment group (7.2 ± 1.4%, p=0.03), the untreated group (7.8 ± 1.2%, p<0.05) and controls (8.5 ± 2.9%, p<0.05).
FMD in the levodopa/entacapone treatment group was intermediate between the levodopa group and the untreated group or controls (Figure 8). Mean time to maximal diameter in FMD was not significantly different between groups (48.8 ± 8.9 sec in the levodopa treatment group, 49.7 ± 9.0 sec in the levodopa/entacapone treatment group, 48.2 ± 9.2 sec in the untreated group and 49.2 ± 9.4 sec in controls). The level of homocysteine was significantly higher in the levodopa treatment group compared to the other groups. Among the FMD tertile subgroups, homocysteine level was significantly lower in the highest tertile compared to the lowest (Figure 8). Correlation analysis showed that the level of homocysteine was negatively correlated with FMD (r=-0.271, p=0.002; Figure 9). This association remained significant after adjusting for age (r=-0.398, p=0.001) because age was partially associated with homocysteine levels (r=0.176, p=0.077). In addition, the level of homocysteine showed a positive correlation with levodopa dose (r=0.369, p<0.001) and a negative correlation with vitamin B12 level (r=-0.198, p=0.045).
In multivariate logistic regression model adjusting for age, sex, duration of levodopa treatment, UPDRS III, hypertension, diabetes mellitus, dyslipidemia, and BMI, the uppermost homocysteine quartiles (odds ratio, 5.70; 95% confidence interval, 1.60-20.27; p=0.007) and age (odds ratio, 1.09; 95% confidence interval, 1.02-1.17; p=0.009) were independent predictors of the lowest tertile of FMD (Table 12).
25
Table 11. Demographic characteristics of patients with Parkinson’s disease and controls
Characteristic PD-L (n=40) PD-L/E (n=33) PD-N (n=22) Controls (n=30) p
Age (y) 70.1 (6.4) 68.1 (9.3) 70.9 (3.7) 67.2 (6.1) NS
Sex (number of men, %) 7 (35.0%) 20 (43.5%) 10 (45%) 10 (33.3%) NS
Disease duration (mo) 46.2 (16.6)a 43.8 (11.2)a 17.7 (3.4) <0.0
5
UPDRS III 18.6 (5.8) 17.9 (4.3) 15.8 (3.6) 0.06
5 Mini-Mental State Examination 26.6 (2.7) 26.3 (2.7) 25.7 (2.8) 26.4 (2.9) NS
Levodopa therapy duration (mo) 36.7 (10.7) 34.73 (10.3) NS
Entacapone therapy duration (mo) 18.75 (6.9)
Levodopa (mg/day) 400.1 (123.8) 343.2 (127.3) 0.04
Entacapone (mg/day) 0 (0) 600.0 (0.0) NS
Levodopa equivalent dose 483.5 (139.2) 454.7 (196.0) NS
Body mass index (kg/m2) 23.8 (2.2) 23.9 (2.2) 23.5 (2.1) 24.3 (1.7) NS Systolic blood pressure (mm Hg) 122.3 (10.2) 124.2(11.3) 122.4 (13.6) 125 (11.8) NS Diastolic blood pressure (mm Hg) 79.2 (8.3) 78.3 (8.2) 80.3 (9.2) 81.3 (9.3) NS
Smoking history 4 (10.0%) 5 (15.2%) 2 (9.1%) 3 (10.0%) NS Hypertension 17 (42.5%) 11 (27.5%) 7 (31.8%) 12 (30.0%) NS Diabetes mellitus 5 (12.5%) 5 (15.2%) 2 (9.0%) 3 (10.0%) NS Dyslipidemia 5 (12.5%) 3 (9.1%) 4 (13.6%) 4 (13.3%) NS Vitamin B12 (pg/ml) 634.0 (287.7) 657.8 (167.3) 649.1 (189.4) 755.1 (268.3) NS Folate (ng/ml) 9.3 (3.9) 10.1 (3.6) 9.2 (3.7) 10.2 (3.8) NS C-reactive protein (mg/dl) 1.4 (2.2)b 1.3 (1.9) 0.8 (0.9) 0.8 (1.1) 0.04 3 Homocysteine (µmol/L) 15.3 (5.9)c 12.7 (1.7) 12.9 (2.4) 11.9 (3.4) 0.03 5 Values are expressed as mean (SD) or numbers (percentage). PD-L, Parkinson’s disease with levodopa treatment; PD-L/E,
Parkinson’s disease with levodopa/entacapone treatment; PD-N, untreated Parkinson’s disease. aCompared to PD-N at p<0.05. bCompared to controls at p<0.05. cCompared to PD-L/E, PD-N or controls at p<0.05. NS, not significant.
26
Figure 4. Flow-mediated dilation in patients with PD and controls. Box-and-whisker plot revealed that
flow-mediated dilation was significantly decreased in PD patients with levodopa treatment compared with those with levodopa/entacapone treatment (p=0.03), no treatment (p<0.05), and controls (p<0.05). The black horizontal line in each box represents the median, the boxes represent the interquartile range, and the whiskers represent the minimum and maximum. *p=0.03, **p<0.05, ***p<0.05.
27
Figure 5. Relationship between flow-mediated dilation and homocysteine
Correlation analysis showed that the level of homocysteine was significantly negatively correlated with flow-mediated dilation.
28
Table 12. Multivariate-adjusted odds ratios of variables associated with the lowest tertile of FMD.
Univariate OR Multivariate OR (95% CI) p
Age (y) 1.081 1.09 (1.02-1.17) 0.011 UPDRS III 1.021 1.01 (0.95-1.06) NS Hypertension 1.34 1.29 (0.46-3.62) NS Diabetes 1.45 1.79 (0.39-8.07) NS Dyslipidemia 1.69 2.25 (0.51-10.06) NS BMI (kg/m2) 0.86 0.87 (0.68-1.11) NS Homocysteine quartiles 1st (< 10.9) Reference Reference 2nd (10.9 – 12.7) 1.14 0.93 (0.18-4.5) 0.928 3rd (12.7 – 14.5) 2.65 2.69 (0.62-11.56) 0.186 4th (> 14.5) 5.86 6.33 (1.61-26.65) 0.012
OR = odds ratio; CI = confidence intervals; UPDRS=unified Parkinson’s disease rating scale; BMI=body mass index; NS = not significant. Odds ratios were adjusted for age, sex, duration of levodopa medication, UPDRS III, HTN, DM, dyslipidemia, and BMI.
29
3.7. Effect of levodopa on endothelial function in PD: serial follow-up study
This study included 36 patients with de novo PD. Homocysteine levels and brachial artery FMD were investigated before and after 10-15 months of levodopa (LD; n=18) or dopamine agonist (DA; n=18) treatment. Homocysteine increased (11.52 ± 0.45 to 14.33 ± 0.68, p < 0.05) during levodopa treatment, but not in response to DA (10.59 ± 0.38 to 11.38 ± 0.67, p=0.184). FMD decreased after levodopa treatment (8.60 ± 0.46 to 7.210 ± 0.402, p=0.002) but there were no significant changes after DA treatment (8.33 ± 0.38 to 8.226 ± 0.330, p=0.266; Table 12) Correlation analysis revealed that the changes in homocysteine levels were negatively correlated with changes in FMD (r=-0.309, p=0.067). This indicates that 1 year of levodopa treatment may adversely affect endothelial function in de novo PD.
30
Table 13. Change of FMD and level of homocysteine after levodopa and dopamine agonist treatment
Levodopa (n= 18) Dopamine agonist (n=18)
Characteristic baseline follow up baseline follow up
Age (years) 69.7 (4.3) 65.3 (7.0) a
Sex (male) 7 (38.8%) 37 (49%)
Disease duration (months) 14.3 (5.6) 16.2 (6.7)
Motor UPDRS 17.5 (3.8) 15.1 (2.5) 16.7 (3.0) 15.7 (2.1)
Levodopa daily dose 0 231.9 (61.7) 0 202.8 (51.7)
FMD (%) 8.6 (0.4) 7.2 (0.4) 8.3 (0.4) a 8.2 (0.3)
Homocysteine 11.5 (0.45) 14.3 (0.6) 10.5 (0.3)a 11.4 (0.7)
Values are expressed as mean (SD) or numbers (with percentages). PD, Parkinson’s disease, UPDRS, Unified Parkinson’s Disease Rating Scale, a Significant difference between baseline and follow-up at p < 0.05.
31
3.8. Effect of endothelial dysfunction on cognition in PD
A total of 91 dementia-free PD patients were enrolled. FMD was positively correlated with verbal memory (delayed and recognition) and visual recognition memory, as well as some frontal domain scores (Figure 6). However, given the large number of comparisons (17 cognition tests * 1 FMD parameter = 17), the results did not survive multiple comparison corrections (a = 0.002 [(0.05/ (17)]).
32
Figure 6. Correlations between FMD and cognition in PD
R=0.28 P=0.007 R=0.25 P=0.01 R=0.23 P=0.03 R=0.21 P=0.04 R=0.21 P=0.06 R=0.21 P=0.05
33
3.9. Effect of subthalamic deep brain stimulation on FMD and HRV
Twenty patients with advanced PD who underwent subthalamic (STN) DBS surgery were enrolled. HRV and FMD were investigated before and 1 year after surgery. FMD improved (6.01 ± 1.51 to 6.79 ± 1.57, p=0.04), but there were no significant changes in HRV parameters (Table 13; Figure 7). While the level of homocysteine slightly decreased (13.9 ± 4.1 to 13.1 ± 3.1, p=0.041), there was no significant correlation between changes in homocysteine levels and alterations in FMD (r=-0.209, p=0.087).
34
Table 14. Change of FMD and level of homocysteine after DBS surgery in PD
Patients undergoing STN-DBS (n= 20 )
Characteristic baseline follow up
Age (years) 64.5 (8.0)
Sex (male) 12 (60%)
Disease duration (months) 123.5 (64.1)
Motor UPDRS (Off) 46.6 (13.2) 25.1 (11.3)
Levodopa equivalent daily dose 681 (133) 331.9 (61.7)
FMD (%) 6.01 (1.5) 6.79 (1.57)*
Homocysteine 13.9 (4.1) 13.1 (3.1)
Values are expressed as mean (SD) or numbers (with percentages). PD, Parkinson’s disease, UPDRS, Unified Parkinson’s Disease Rating Scale. a Significant difference between before and after DBS at p < 0.05.
35
Figure 7. The difference of FMD and HRV parameter before and after DBS
SDNN, standard deviation of the normal-to-normal RR interval; RMSSD, root mean square difference between successive RR intervals; TP, total spectral power; LF, low frequency; HF, high frequency. * Significant difference before and after
DBS at P < 0.05.
* NS
NS NS
36
IV. Discussion
4.1. Cardiovascular autonomic system in PD
PD and ET are the most common movement disorders in the elderly. Both ET patients and the elderly can display subtle parkinsonian signs [54]. Furthermore, a recent study demonstrated that one in five patients with ET have a tremor at rest [55]. In patients with PD, postural tremors occur as frequently as tremors at rest, and may be the presenting symptom [56]. Accordingly, differentiating between ET and PD is often challenging [4,5]. To improve the early diagnosis of ET and PD, positron emission tomography (PET), cardiac MIBG scanning, and olfaction studies have been proposed [57,58]. However, simple markers are also needed to allow the accurate identification of PD during the early stages. Our results showed that almost all parameters of HRV were significantly lower in patients with PD compared to those with ET, whereas differences between the ET and control groups were not significant. This suggests that HRV may be helpful in differentiating PD from ET at the early stage of PD. Although PD and ET differ in their pathogenesis, their clinical features are similar. Patients with TDPD usually respond poorly to levodopa treatment, and their prognosis is favorable. In addition, some patients with definite signs of PD have normal 18F-dopamine PET scans, and those with isolated resting or action tremors have consistently abnormal striatal dopamine transporter (DAT) uptake [59]. As such, early TDPD is commonly misdiagnosed as ET, emphasizing the need for an additional simple diagnostic tool capable of distinguishing between the two conditions. The distinction is important in determining prognosis, treatment planning, and identifying eligible patients for clinical studies.
TP and SDNN represent overall cardiac autonomic dysfunction, and RMSSD represents parasympathetic function. While LF predominantly represents the sympathetic nervous system, the HF component is generally a marker of the vagal nervous system. In our study, most HRV parameters were significantly lower in the PD group compared to the ET and control groups. Among HRV components, overall cardiac autonomic dysfunction (TP, SDNN) and cardiac sympathetic dysfunction (LF) was more prominent than parasympathetic dysfunction (HF, RMSSD). Our findings suggest that cardiac sympathetic dysfunction is prominent, but cardiac parasympathetic dysfunction is also present in early PD. This is consistent with previous studies reporting prominent peripheral sympathetic denervation combined with significant central autonomic dysfunction in the brainstem including the
37
dorsal vagal nucleus in PD. However, an understanding of the pathological role played by HRV is needed to validate its usefulness as an early non-invasive imaging marker in PD.
Dementia is one of the most disabling non-motor symptoms that occurs in PD. Our findings show that decreased cardiac MIBG uptake increases the risk for the development of dementia.
Several studies have indicated that cognition, olfaction, visual hallucination and RBD are associated with decreased cardiac MIBG uptake in PD [25-27]. By contrast, striatal dopamine depletion is not well correlated with non-motor symptoms [60,61] but rather is correlated with motor severity and predicts the motor progression [62]. This suggests that the cardiac MIBG uptake might provide information regarding the presence of an extranigral alpha-synuclein pathology. Our results are in agreement with those of a previous Japanese follow up study, which showed a significant difference in the motor progression and the occurrence of dementia between the two groups that were divided according to delayed H/M ratio [63].
The clinical significance of HRV on cognition remains unclear. Some cross-sectional studies found that HRV in patients with MCI was similar to that of healthy controls [64], but others showed that HRV was slightly impaired compared to controls when subjects were standing [65,66]. Our findings demonstrate that in early PD, visuospatial and frontal function are correlated with some HRV parameters. There are several explanations for these observed associations. First, low HRV as a reflection of autonomic dysfunction might directly underlie cognitive impairment by causing dysregulation of cerebral perfusion [67,68]. Furthermore, it is possible that low HRV might reflect established cerebral lesions and neurodegenerative processes present in the brain [69]. Secondly, that low HRV is associated with increased blood pressure variability, which is associated with cognitive decline and structural brain changes [70]. Executive function is mainly controlled by the prefrontal cortex of the brain. Reduced HRV is associated with hypoactivity of the prefrontal cortex, which is likely to affect executive function [71]. Furthermore, the frontal cortex is able to adjust HRV via subcortical structures such as the amygdala. This cortico-subcortical inhibitory circuit represents the structural connection between neuropsychological processes (such as cognitive function) and physiologic processes (such as HRV). Abnormalities in the cortico-subcortical circuit can be reflected in HRV. Future brain imaging studies could provide new insight into the biology of these associations [72].
38
4.2. Vascular endothelial system in PD
Levodopa treatment is the gold standard therapy in PD patients. However, this therapy increases serum levels of homocysteine, due to its metabolism via catechol-O-methyltransferase [73]. Several reports have shown that hyperhomocysteinemia might be associated with increased prevalence of coronary artery disease, carotid intima media thickness, peripheral neuropathy, and cognitive impairment in patients with PD [74-77], although there have been conflicting results concerning the risk of stroke in PD [78].
It is generally accepted that endothelial dysfunction is part of the early pathogenesis of atherosclerosis [46]. Along with traditional vascular risk factors, hyperhomocysteinemia is known to decrease FMD [79]. In this study, FMD was significantly lower in the levodopa treatment group compared to those in the levodopa/entacapone treatment group and controls. In addition, homocysteine level was negatively correlated with FMD, and was an independent predictor of the lowest tertile, indicating that endothelial dysfunction as assessed by the FMD is associated with chronic levodopa treatment in PD patients.
In our prospective follow-up study in de novo PD, FMD decreased after 1 year of levodopa treatment. However, there was no correlation between the changes in homocysteine levels and FMD. In addition, STN DBS surgery could decrease levodopa dosage by almost 50%, and improve motor and endothelial function but had no direct effect on cardiac autonomic function.
Decreased FMD has been found in patients with cerebrovascular risk factors [80] and has been shown to have prognostic significance in the development of cardiovascular events [81]. In addition to traditional vascular risk factors, hyperhomocysteinemia is known to decrease FMD [79]. However, it is unclear whether hyperhomocysteinemia is a direct cause of decreased FMD or a marker of atherosclerosis. Several studies demonstrated that acute changes in homocysteine by methionine loading can cause decreased FMD in healthy elderly patients [82]. In this regard, the results of the present study provide evidence of a possible association between FMD and homocysteine levels in patients with PD. In line with our findings, Yong et al. demonstrated that changes in homocysteine levels after treatment with levodopa affect cerebral hemodynamics, such as pulsatility index. This may reflect systemic vascular resistance and increased vascular stiffness associated with endothelial dysfunction [83]. Similarly, in patients with ischemic stroke, hyperhomocysteinemia was independently associated with an increased pulsatility index in the cerebral arteries [84]. In addition,
39
several reports have demonstrated that homocysteine-lowering therapy (using folic acid or vitamin B) can improve endothelial dysfunction as assessed by FMD [85] and reduce progression of carotid intima media thickness (a marker of early atherosclerosis) in asymptomatic subjects with hyperhomocysteinemia [86]. However, our prospective study shows that changes in homocysteine levels after levodopa treatment or DBS surgery did not correlate with FMD changes. It is possible levodopa may generate more oxidative stress, which may affect endothelial function [87].
Several recent studies report evidence of vascular involvement in PD, supporting our findings. For example, CSF biomarkers of angiogenesis are increased in PD, and are associated with gait impairments, increased blood brain barrier permeability, white matter lesions and cerebral microbleeds, indicating that abnormal angiogenesis may be present in PD pathogenesis and contribute to dopa-resistant symptoms [88]. Other lines of evidence include a human pathological study of PD cases showing endothelial degeneration and preservation of basement membrane, leading to an increase in string vessel formation in PD. String vessels have no function in circulation, suggesting cerebral hypoperfusion may contribute to the neuronal degeneration characteristic of PD [45].
V. Conclusion
Neurodegeneration does not occur in isolation but is believed to result from various chronic insults such as neurotoxic material, mitochondrial dysfunction, and accumulation of abnormal proteins that interact over time leading to selective neuronal loss.
Cardiac autonomic dysfunction occurs early in Lewy body disorders, including PD, DLB, and RBD, reflecting the early accumulation of Lewy bodies in cardiac sympathetic postganglionic nerves. HRV was significantly lower in early PD and DLB, and higher HRV was associated with better cognitive function. In addition, a reduction in cardiac MIBG uptake was associated with subsequent risk of dementia, suggesting reduced uptake may reflect wider extension of alpha-synuclein pathology in PD Traditional vascular risk factors and brain white matter changes contribute to the neurodegenerative process in PD. Vascular endothelial dysfunction occurs during early stages of atherosclerosis, and plays an important role in selective permeability of molecules entering the brain from the bloodstream. FMD was significantly lower in PD patients, which was associated with levodopa treatment. STN-DBS could reduce levodopa dosage and improve FMD with significant motor improvement. The
40
modification of these parameters represents a promising therapeutic approach to treat PD.
Figure 8. Proposed mechanism of the relationship between cardiac autonomic and vascular endothelial
dysfunction in PD.
41 References
[1] Cai W, Zhang K, Li P, et al. Dysfunction of the neurovascular unit in ischemic stroke and neurodegenerative diseases: An aging effect. Ageing research reviews 2017;34:77-87.
[2] Collins LM, Toulouse A, Connor TJ, et al. Contributions of central and systemic inflammation to the pathophysiology of Parkinson's disease. Neuropharmacology 2012;62:2154-68.
[3] Joe EH, Choi DJ, An J, et al. Astrocytes, Microglia, and Parkinson's Disease. Experimental neurobiology 2018;27:77-87.
[4] Grammas P, Martinez J, Miller B. Cerebral microvascular endothelium and the pathogenesis
of neurodegenerative diseases. Expert reviews in molecular medicine 2011;13:e19.
[5] Nelson AR, Sweeney MD, Sagare AP, et al. Neurovascular dysfunction and
neurodegeneration in dementia and Alzheimer's disease. Biochimica et biophysica acta 2016;1862:887-900.
[6] Sweeney MD, Sagare AP, Zlokovic BV. Blood-brain barrier breakdown in Alzheimer disease
and other neurodegenerative disorders. Nature reviews Neurology 2018;14:133-50.
[7] Nanhoe-Mahabier W, de Laat KF, Visser JE, et al. Parkinson disease and comorbid
cerebrovascular disease. Nature reviews Neurology 2009;5:533-41.
[8] Sweeney MD, Kisler K, Montagne A, et al. The role of brain vasculature in neurodegenerative disorders. Nature neuroscience 2018;21:1318-31.
[9] Gorelick PB, Scuteri A, Black SE, et al. Vascular contributions to cognitive impairment and dementia: a statement for healthcare professionals from the american heart association/american stroke association. Stroke 2011;42:2672-713.
[10] Ziemssen T, Reichmann H. Cardiovascular autonomic dysfunction in Parkinson's disease.
Journal of the Neurological Sciences 2010;289:74-80.
[11] Xhyheri B, Manfrini O, Mazzolini M, et al. Heart Rate Variability Today. Progress in
Cardiovascular Diseases 2012;55:321-31.
[12] Postuma RB, Lanfranchi PA, Blais H, et al. Cardiac autonomic dysfunction in idiopathic REM sleep behavior disorder. Movement Disorders 2010;25:2304-10.
[13] Kasanuki K, Iseki E, Fujishiro H, et al. Impaired heart rate variability in patients with dementia with Lewy bodies: Efficacy of electrocardiogram as a supporting diagnostic marker. Parkinsonism & related disorders 2015;21:749-54.
42
rate variability and sympathetic skin response in Parkinson’s disease. Journal of Neural Transmission 2015;122:419-25.
[15] Valappil RA, Black JE, Broderick MJ, et al. Exploring the electrocardiogram as a potential tool to screen for premotor Parkinson's disease. Movement Disorders 2010;25:2296-303.
[16] Palma J-A, Carmona-Abellan M-M, Barriobero N, et al. Is cardiac function impaired in
premotor Parkinson's disease? A retrospective cohort study. Movement Disorders 2013;28:591-6.
[17] Alonso A, Huang X, Mosley TH, et al. Heart rate variability and the risk of Parkinson disease: The Atherosclerosis Risk in Communities study. Annals of Neurology 2015;77:877-83. [18] da Silva VP, Ramalho Oliveira BR, Tavares Mello RG, et al. Heart Rate Variability Indexes
in Dementia: A Systematic Review with a Quantitative Analysis. Current Alzheimer research 2018;15:80-8.
[19] Bellelli G, Pezzini A, Bianchetti A, et al. Increased blood pressure variability may be
associated with cognitive decline in hypertensive elderly subjects with no dementia. Archives of internal medicine 2002;162:483-4.
[20] Kanemaru A, Kanemaru K, Kuwajima I. The Effects of Short-Term Blood Pressure Variability and Nighttime Blood Pressure Levels on Cognitive Function. Hypertension Research 2001;24:19-24.
[21] Sloan RP, Demeersman RE, Shapiro PA, et al. Cardiac autonomic control is inversely related to blood pressure variability responses to psychological challenge. American Journal of Physiology-Heart and Circulatory Physiology 1997;272:H2227-H32.
[22] Thayer JF, Hansen AL, Saus-Rose E, et al. Heart Rate Variability, Prefrontal Neural Function, and Cognitive Performance: The Neurovisceral Integration Perspective on Self-regulation, Adaptation, and Health. Annals of Behavioral Medicine 2009;37:141-53.
[23] Takahashi M, Ikemura M, Oka T, et al. Quantitative correlation between cardiac MIBG uptake and remaining axons in the cardiac sympathetic nerve in Lewy body disease. Journal of Neurology, Neurosurgery & Psychiatry 2015;86:939-44.
[24] Sakakibara R, Tateno F, Kishi M, et al. MIBG myocardial scintigraphy in pre-motor
Parkinson's disease: A review. Parkinsonism & related disorders 2014;20:267-73.
[25] Mizutani Y, Nakamura T, Okada A, et al. Hyposmia and cardiovascular dysautonomia
correlatively appear in early-stage Parkinson's disease. Parkinsonism & related disorders 2014;20:520-4.
43
[26] Nomura T, Inoue Y, Högl B, et al. Relationship between 123I-MIBG scintigrams and REM
sleep behavior disorder in Parkinson’s disease. Parkinsonism & related disorders 2010;16:683-5.
[27] Kim J-S, Shim Y-S, Song I-U, et al. Cardiac sympathetic denervation and its association with cognitive deficits in Parkinson's disease. Parkinsonism & related disorders 2009;15:706-8.
[28] McDonald C, Newton JL, Burn DJ. Orthostatic hypotension and cognitive impairment in
Parkinson's disease: Causation or association? Movement Disorders 2016;31:937-46.
[29] Udow SJ, Robertson AD, MacIntosh BJ, et al. ‘Under pressure’: is there a link between
orthostatic hypotension and cognitive impairment in α-synucleinopathies? Journal of
Neurology, Neurosurgery & Psychiatry 2016;87:1311-21.
[30] Centi J, Freeman R, Gibbons CH, et al. Effects of orthostatic hypotension on cognition in Parkinson disease. Neurology 2017;88:17-24.
[31] Zlokovic BV. Neurovascular pathways to neurodegeneration in Alzheimer's disease and other disorders. Nature reviews Neuroscience 2011;12:723-38.
[32] Malek N, Lawton MA, Swallow DM, et al. Vascular disease and vascular risk factors in
relation to motor features and cognition in early Parkinson's disease. Movement disorders : official journal of the Movement Disorder Society 2016;31:1518-26.
[33] Tsao CW, Seshadri S, Beiser AS, et al. Relations of arterial stiffness and endothelial function to brain aging in the community. Neurology 2013;81:984-91.
[34] Mitchell GF, van Buchem MA, Sigurdsson S, et al. Arterial stiffness, pressure and flow
pulsatility and brain structure and function: the Age, Gene/Environment Susceptibility--Reykjavik study. Brain : a journal of neurology 2011;134:3398-407.
[35] Kotagal V, Albin RL, Muller ML, et al. Clinical features of Parkinson disease when onset of diabetes came first: a case-control study. Neurology 2012;79:1835-6; author reply 6.
[36] de Laat KF, van Norden AG, Gons RA, et al. Cerebral white matter lesions and lacunar infarcts contribute to the presence of mild parkinsonian signs. Stroke 2012;43:2574-9.
[37] Hatate J, Miwa K, Matsumoto M, et al. Association between cerebral small vessel diseases and mild parkinsonian signs in the elderly with vascular risk factors. Parkinsonism & related disorders 2016;26:29-34.
[38] Guan J, Pavlovic D, Dalkie N, et al. Vascular degeneration in Parkinson's disease. Brain pathology (Zurich, Switzerland) 2013;23:154-64.
44 dementia. J Neurol Sci 2009;283:28-31.
[40] Bartels AL, Willemsen AT, Kortekaas R, et al. Decreased blood-brain barrier P-glycoprotein function in the progression of Parkinson's disease, PSP and MSA. Journal of neural transmission (Vienna, Austria : 1996) 2008;115:1001-9.
[41] Kortekaas R, Leenders KL, van Oostrom JC, et al. Blood-brain barrier dysfunction in
parkinsonian midbrain in vivo. Ann Neurol 2005;57:176-9.
[42] Desai BS, Monahan AJ, Carvey PM, et al. Blood-brain barrier pathology in Alzheimer's and Parkinson's disease: implications for drug therapy. Cell transplantation 2007;16:285-99. [43] Ohlin KE, Francardo V, Lindgren HS, et al. Vascular endothelial growth factor is upregulated
by L-dopa in the parkinsonian brain: implications for the development of dyskinesia. Brain : a journal of neurology 2011;134:2339-57.
[44] Lerner RP, Francardo V, Fujita K, et al. Levodopa-induced abnormal involuntary movements correlate with altered permeability of the blood-brain-barrier in the basal ganglia. Scientific reports 2017;7:16005.
[45] Yang P, Pavlovic D, Waldvogel H, et al. String Vessel Formation is Increased in the Brain of Parkinson Disease. Journal of Parkinson's disease 2015;5:821-36.
[46] Celermajer DS. Endothelial dysfunction: does it matter? Is it reversible? Journal of the American College of Cardiology 1997;30:325-33.
[47] Vita JA, Keaney JF, Jr. Endothelial function: a barometer for cardiovascular risk? Circulation 2002;106:640-2.
[48] Dede DS, Yavuz B, Yavuz BB, et al. Assessment of Endothelial Function in Alzheimer's
Disease: Is Alzheimer's Disease a Vascular Disease? Journal of the American Geriatrics Society 2007;55:1613-7.
[49] Gonzales MM, Tarumi T, Tanaka H, et al. Functional imaging of working memory and
peripheral endothelial function in middle-aged adults. Brain and Cognition 2010;73:146-51. [50] Hoth KF, Tate DF, Poppas A, et al. Endothelial function and white matter hyperintensities in
older adults with cardiovascular disease. Stroke 2007;38:308-12.
[51] White RP, Deane C, Vallance P, et al. Nitric oxide synthase inhibition in humans reduces cerebral blood flow but not the hyperemic response to hypercapnia. Stroke 1998;29:467-72.
[52] Ahn H-J, Chin J, Park A, et al. Seoul Neuropsychological Screening Battery-Dementia
Version (SNSB-D): A Useful Tool for Assessing and Monitoring Cognitive Impairments in Dementia Patients. J Korean Med Sci 2010;25:1071-6.