[원저]
한국 폐경 여성에서 생물학적 스트레스 지표와 대사증후군의 요소
최영근, 오한진, 주일우
관동대학교 의과대학 제일병원 가정의학과
Biologic Stress Markers and Components of Metabolic Syndrome in Postmenopausal Korean Women
Younggun Choi, Hanjin Oh, Ilwoo Joo
College of Medicine, Kwandong University Dept. of Family Medicine, Cheil General Hospital
Background The key pathophysiology of metabolic syndrome (MS) is insulin resistance. Chronic stress may induce increased insulin resistance, high blood glucose, visceral obesity, and high blood pressure via increased cortisol levels from chronic activation of the hypothalamus-pituitary-adrenal axis (HPA axis).
However, the relationships between cortisol, dehydroepiandrosterone sulfate (DHEA-S), and cortisol)/DHEA-S and each of the components of MS have not yet been thoroughly investigated. In our study, we evaluated the relationships between cortisol, DHEA-S, and cortisol/DHEA-S as biologic stress markers and components of MS in postmenopausal Korean women.
Methods This study was a cross-sectional analysis of 223 postmenopausal women who visited our climacteric clinic at a university hospital in Seoul with stressful events. These women were seen between January 2001 and March 2008. Metabolic syndrome was diagnosed according to the NCEP-ATP III criteria using body mass index (BMI) instead of waist circumference. We evaluated the relationships between each biological stress marker and the components of MS.
Independent t-tests were conducted on each cut-off point of the MS components. The study population was classified as normal subjects (no MS components) or MS subjects (>3 MS components). Mean differences in biologic stress markers between normal and MS subjects were evaluated by independent t-tests.
Results Cortisol levels were positively associated with FPG (p=0.01), and DHEA-S levels were negatively associated with TG (p=0.019), but not with the other components of MS. DHEA-S levels showed statistically significant mean differences from BMI, FPG, TG, and HDL-C (p=0.022; p=0.004; p=0.012; p=0.010) by independent t-tests. Significant mean differences in DHEA-S and cortisol/DHEA-S between normal subjects and MS subjects were also observed (p=0.0002, p=0.039), but the mean difference in cortisol was not significant.
Conclusions It has been hypothesized that persistent chronic psychosocial stress may be a causative factor of MS. Unfortunately, we were unable to look into this hypothesis because of the limitations of the cross-sectional design. However, this study suggests that DHEA-S levels and MS might be meaningfully correlated. (Korean J Health Promot Dis Prev 2009 ; 9(1):50-55) Key words metabolic syndrome, stress, cortisol, DHEA-S
1)
∙교신저자 : 주 일 우
∙주 소 : 중구 묵정동 1-19 제일병원 가정의학과
∙전 화 : 02-2000-7159
∙E-mail : [email protected]
∙접 수 일 : 2008년 10월 1일 ∙채 택 일 : 2008년 12월 5일
서 론
대사증후군은 심혈관 질환의 발생과 밀접한 관련성을 가지 고 있다.1,2) 대사증후군은 1988년 Reaven GM에 의해 처음 기 술된 이후로 많은 관심과 임상적 의의를 가지게 되었다.3)
대사증후군의 유병률 은 사용되는 진단 기준에 따라 같은 연구 집단에서도 차이를 보이지만 진단의 핵심 요소는 대체 로 복부비만, 고중성지방혈증, 낮은 HDL 콜레스테롤, 고혈압, 고혈당이다. 실제로 많은 환자들에서 질환이 한가지만 존재 하기 보다는 비만, 고혈압, 당뇨병, 고지혈증과 같은 여러 질 환이 공존하고 있는 경우가 많다. 또한 여러 대사 이상을 보 이는 대사증후군의 핵심병리기전은 인슐린 저항성으로 생각 되어지고 있으며4), 유전적 인자와 더불어 여러 환경인자 및 생활습관이 대사증후군을 유발하는 것으로 추정되어진다.5,6)
스트레스에 대한 우리 몸의 반응은 자율신경계와 시상하부- 뇌하수체-부신 축에 의한 내분비계에 의해 나타난다. 코르티솔 (cortisol), DHEA-S, 또는 코르티솔(cortisol)/DHEA-S는 여러 급, 만성 스트레스에 대한 연구 지표로 활용되어 왔다.7-9) 특히 DHEA는 ACTH-regulated steoid로서 스트레스에 따른 anti-glucocorticoid property를 나타내므로 최근 스트레스에 대 한 민감도가 우수한 것으로 입증된 바 있다.8-9) Brunner 등은 대조군 연구를 통해 대사증후군에서 코르티솔(cortisol) 레벨의 상승과 카테콜라민 분비증가, 심장의 교감신경계 우세성을 입 증하였다.5) 스트레스에 의한 교감 신경계 이상은 심장과 큰 혈 관에 영향을 주어 혈압의 상승과 근육에서 포도당을 흡수하는 데 장애를 일으켜 인슐린 감수성을 저하시킨다.10,11) 또한 근골 격계의 교감신경계 항진은 근육으로 가는 영양 혈류의 흐름을 저해하여 지단백분해효소의 접근성이 떨어져 이상지혈증이 나 타나는데 기여를 한다. 급, 만성 스트레스에 대한 반응으로 코르티 솔(cortisol) 레벨이 상승하여 hypercortisolemia가 초래되면 조직에 지나친 코르티솔(cortisol) 노출로 비만을 일으킬 수 있다.12) 이 처럼 스트레스로 인해 나타나는 우리 몸의 반응은 스트레스가 대사증후군을 유발하는 원인 또는 악화 인자가 될 수 있다는 가설을 가능하게 한다.13,14)
이에 본 연구는 대사증후군과 스트레스와의 연관성을 밝히 기 위해 대사증후군의 요소와 생물학적 스트레스 지표인 코 르티솔(cortisol), DHEA-S, 코르티솔(cortisol)/DHEA-S와의 연 관성을 살펴보고 나아가 정상군과 대사증후군간의 차이가 있 는지 확인해 보고자 하였다.
방 법 1. 연구 대상
2001년 1월부터 2008년 3월까지 서울 시내 일개 종합병원에 스트레스를 주소로 내원하여 코르티솔(cortisol)과 DHEA-S 검사 가 시행된 폐경후 여성 293명을 대상으로 하였다. 폐경은 마지막
생리 후 1년이 경과하고 여포자극호르몬(follicular stimulation hormone)이 40 mIU/ml 이상인 경우로 정의하였다. 스트레스의 정의는 매우 모호하다. 본 연구에서 사용되는 스트레스라는 용 어는 Chrosus, Gold 그리고 McEwen이 제시한 ‘항상성을 위협 받는 상태’를 의미하며, 만성스트레스는 ‘항상성에 대해 장기적 으로 반복되는 붕괴’를 뜻한다.15,16)
특히 본 연구는 육체적 스트레스가 아닌 정신사회적 스트레 스에 한정하고 있다. 환자들은 대부분 남편과의 갈등, 이혼, 경 제적 어려움, 자녀와의 갈등 등 장기적인 생활 스트레스를 주소 로 내원하였다. 대상 환자 중 정신분열증이나 조울증과 같은 심 각한 정신과적 질환, 갑갑상선 질환이 있는 경우, AST(aspartate aminotransferase) 또는 ALT(Alanine aminotransferase) 수치가 100 이상인 경우, Creatinine이 1.5이상인 경우를 제외 하였고, 나이가 45세 미만이거나 60세 이상인 환자는 제외 하였다. 따라 서 선정된 293명 중 70명이 배제 되고 총 223명이 연구 대상 군 으로 확정되었다.
2. 연구 방법
대상 환자들로부터 연령과 체질량지수(kg/m2), 공복혈당, 총 콜레스테롤, 중성지방, HDL 콜레스테롤, LDL 콜레스테롤, 혈 압을 측정하였고 생물학적 스트레스 지표로 코르티솔(cortisol), DHEA-S 및 코르티솔(cortisol)/DHEA-S를 확인 하였다.
신장 및 체중은 가벼운 옷을 입은 상태에서 신체 계측기와 전자체중계를 사용하였으며 체중을 신장의 제곱으로 나누어 체질량지수를 계산하였다. 혈압은 환자가 충분히 안정을 취한 후 심장과 같은 높이에서 동일 검사자에 의하여 측정되었으며 초진과 이후 2회 내원시 측정된 혈압의 평균값으로 하였다.
혈액 검사는 대상자가 8시간 이상 금식 후 시행 되었으며, 공 복혈당은 glucose oxidase법을 이용하여 측정하였고, 지질 농 도는 자동분석기(Hitachi 7150, Tokyo, Japan)로 분석하였다.
HDL, LDL 콜레스테롤의 분류는 침전 기법으로 고밀도 지단 백 콜레스테롤을 먼저 효소법으로 측정 후 choelstest-LDL을 실시하였다. 혈청 코르티솔(cortisol)과 DHEA-S는 아침 9시 에 서 10시 사이에 채취되어 방사면역측정법(N-tactosteo SP, INCSTAR Corp., Stillwater, MN)을 사용하여 측정 되었다.
대사증후군은NCEP-ATP III 진단 기준17)을 사용하되 허리 둘레 대신 체질량지수를 적용하여 다음 다섯 가지 중 세가지 이상인 경우로 하였다. 1) 비만, 체질량지수 ≥ 25.0 kg/m2인 경우로 정의하였다; 2) 높은 혈압, 수축기 혈압이 130 mmHg 이상이거나 혹은 이완기 혈압이 85mmHg 이상인 경우; 3) 고 중성지방혈증, 공복 혈청 중성지방 레벨이 150 mg/dL 이상 인 경우; 4) 낮은 HDL 콜레스테롤, 혈청 HDL 콜레스테롤이
Table 1. Characteristics of the study population (mean ± S.D.)
Total (n=223) Range
Age (yrs) 53.54 ± 4.37 47 - 59 BMI (kg/m2) 23.52 ± 2.97 16.7 - 35.2 FPG (mg/dL) 99.00 ± 21.30 65 - 320 TC (mg/dL) 209.69 ± 37.02 105 - 346 TG (mg/dL) 132.68 ± 66.99 39 - 496 HDL-C (mg/dL) 57.50 ± 10.79 28 - 100 LDL-C (mg/dL) 125.71 ± 33.34 34.6 - 267.2 SBP (mmHg) 127.18 ± 11.76 90 - 170 DBP (mmHg) 81.90 ± 7.08 50 - 110 cortisol (μg/dL) 8.94 ± 3.44 2 - 24 DHEA-S (μg/dL) 68.08 ± 35.96 4 - 188 cortisol/DHEA-S 0.174 ± 0.127 0.03 - 0.82 BMI = body mass index, FPG = fasting plasma glucose, TC = total cholesterol, TG = triglyceride, HDL-C = high-density lipoprotein cholesterol, LDL-C = low-density lipoprotein cholesterol, SBP = systolic blood pressure, DBP = diastolic blood pressure, DHEA-S = dehydroepiandrosterone sulfate.
Table 2. Relationships between biologic stress markers and components of metabolic syndrome
cortisol DHEA-S
r values (p values)
cortisol/DHEA-S
BMI (kg/m2) 0.025 (0.702) -0.068 (0.303) 0.039 (0.557) FPG (mg/dL) 0.170 (0.010)* 0.010 (0.878) 0.032 (0.635) TG (mg/dL) 0.093 (0.161) -0.155 (0.019)* 0.110 (0.096) HDL-C (mg/dL) 0.041 (0.538) 0.111 (0.095) 0.024 (0.715) SBP (mmHg) 0.047 (0.481) -0.050 (0.450) 0.061 (0.359) DBP (mmHg) 0.057 (0.389) -0.078 (0.240) 0.071 (0.284)
* p < 0.05
Table 3. Independent t-test comparing biologic stress markers and components of metabolic syndrome
cortisol DHEA-S cortisol/DHEA-S
Mean ± S.D.
BMI ≥25
<25 p value
9.09 ± 3.20 8.89 ± 3.52 0.707
59.61 ± 29.19 70.84 ± 37.57 0.022*
0.20 ± 0.12 0.17 ± 0.13 0.130 FPG ≥110
<110 p value
10.08 ± 4.07 8.72 ± 3.28 0.065
56.25 ± 23.45 70.30 ± 37.48 0.004*
0.20 ± 0.10 0.17 ± 0.13 0.141 TG ≥150
<150 p value
9.30 ± 4.33 8.79 ± 2.30 0.381
58.84 ± 32.79 71.93 ± 36.61 0.012*
0.20 ± 0.11 0.16 ± 0.13 0.097 HDL-C <50
≥50 p value
8.92 ± 3.41 8.98 ± 3.56 0.912
71.26 ± 37.35 58.54 ± 29.73 0.010*
0.17 ± 0.13 0.19 ± 0.12 0.227 SBP ≥130
<130 p value
9.14 ± 3.43 8.70 ± 3.46 0.341
65.30 ± 34.44 71.45 ± 37.62 0.200
0.18 ± 0.12 0.16 ± 0.13 0.251 DBP ≥85
<85 p value
9.52 ± 3.55 8.72 ± 3.38 0.113
66.68 ± 36.11 68.61 ± 35.70 0.718
0.18 ± 0.10 0.17 ± 0.14 0.681
* p<0.05
50 mg/dL 미만인 경우; 5) 고혈당 상태, 공복 혈장 포도당 레벨이 110 mg/dL 이상인 경우.
3. 통계분석
생물학적 스트레스 지표와 각 대사증후군의 요소와의 상관 성을 밝히기 위해 Pearson 상관계수가 사용 되었다. 각각의 대 사증후군의 요소에서 경계점을 기준으로 생물학적 지표의 평 균간 차이가 있는지 알아보기 위해 독립표본 T-test가 사용 되 었다. 마지막으로 대상 환자들을 대사증후군의 요소 수가 3개 이상인 경우와 그 미만인 경우로 각각 대사증후군 환자와 정상 군으로 나누었을 때 생물학적 스트레스 지표들의 각 군간 평균 이 유의한 차이가 있는지 알아보기 위해 독립표본 T-test가 사 용 되었다. 모든 통계 분석은 SPSS version 12.0 (for windows) 을 이용하였으며 P value 0.05 미만을 통계학적으로 유의 하다 고 간주 하였다.
결 과 1. 연구대상자들의 일반적 특징
대상 군의 평균 연령은 53.5±4.4[S.D.](범위 47~59)세이며 평균 체질량지수는 23.5±3.0[S.D.]kg/m2이었다. 공복혈당의 평균은 99.0±21.3[S.D.]mg/dL이었고 중성지방은 132.7±67.0[S.D.]mg/dL,
HDL 콜레스테롤은 57.5±10.8[S.D.]mg/dL, 혈압은 129.2/82.0±10.7/
8.1[S.D.]mmHg이었다. 혈청 코르티솔(cortisol)은 8.94±3.44, DHEA-S는 68.08±35.96이었으며, 코르티솔(cortisol)/DHEA-S는 0.174±0.127이었다(Table 1).
2. 생물학적 스트레스 지표와 대사증후군 요소와의 상관성
코르티솔(cortisol), DHEA-S 그리고 코르티솔(cortisol)/DHEA-S 와 대사증후군의 요소 간의 상관성에 대해 살펴보면 코르티솔 (cortisol)은 공복혈당과 유의한 양의 상관관계(r=0.170, p=0.010)가 있었고, DHEA-S는 중성지방과 유의한 음의 상관관계(r=-0.155, p=0.019)를 보였다(Table 2).
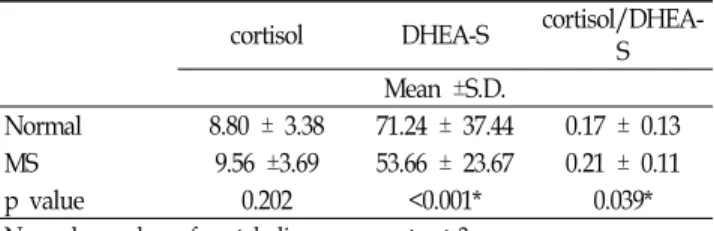
Table 4. Independent t-test comparing normal subjects and those with metabolic syndrome
cortisol DHEA-S cortisol/DHEA-
S Mean ±S.D.
Normal 8.80 ± 3.38 71.24 ± 37.44 0.17 ± 0.13
MS 9.56 ±3.69 53.66 ± 23.67 0.21 ± 0.11
p value 0.202 <0.001* 0.039*
Normal: number of metabolic components < 3
MS: metabolic syndrome, number of metabolic components ≥ 3
* p<0.05
3. 분리 점을 사용한 평균비교
다섯 개의 대사증후군 요소 각각에 대해 정의에 따른 분리 점을 사용하여 두 군으로 나누어 코르티솔(cortisol), DHEA-S, 그리고 코르티솔(cortisol)/DHEA-S의 두 집단 간 평균의 차 이가 있는지 독립표본 T-test를 통해 알아 보았다. 코르티솔 (cortisol)과 코르티솔(cortisol)/DHEA-S는 어떤 요소에서도 유의한 평균 차이를 보이지 않았다. 그러나 DHEA-S는 다섯 요소 중 혈압을 제외한 네 가지 요소에서 유의한 평균 차이 (체질량지수, p=0.022; 공복혈당, p=0.004; 중성지방, p=0.012;
HDL-C, p=0.010)를 보였다(Table 3). 독립표본 T-test를 이용 하여 대상 군을 요소 수가 3개 이상인 대사증후군과 2개 이 하인 정상군으로 분류하여 평균비교를 하였다.
코르티솔(cortisol)은 정상군과 대사증후군 간에 유의한 차 이가 없었으나 DHEA-S와 코르티솔(cortisol)/DHEA-S에서는 두 군간에 유의한 차이(p<0.001, p=0.039)가 있었다(Table 4).
고 찰
스트레스에 대한 자율신경계의 반응은 맥박과 혈압상승 식욕 감소 및 장 운동의 저하로 나타나고, 내분비 반응인 시상하부-뇌 하수체-부신축은 부신 피질의 글루코코르티코이드를 분비하여 우리 몸의 항상성과 스트레스 반응을 조절한다. 급성 스트레스 에 대한 이러한 우리 몸의 반응은 좋은 측면으로는 한 개체의 생존을 도모하고 감정적, 지적 성장과 발전을 향상시키는 긍정 적 기능을 가지고 있다.18) 그러나, 개체가 감당할 수 없는 조절 불가능한 위협적 상황에 노출 되거나 만성적인 스트레스 상황에 놓이는 경우 시상하부-뇌하수체-부신축의 만성적인 활성화를 초 래하여 감정적, 신체적 질환을 초래 할 수도 있다.19-21) 스트레스 에 대한 반응 중 내분비 반응인 시상하부-뇌하수체-부신축의 활 성화는 비만, 우울증, 대사증후군과 같은 질환과 유사한 병태 생 리를 공유하고 있다.22) 여러 역학 자료들은 코르티솔(cortisol) 수
치와 대사 증후군의 핵심 요소들 간의 양의 상관 관계에 대해 밝히고 있으며, 코르티솔(cortisol), DHEA 또는 DHEA-S는 스트 레스를 연구한 많은 논문들에서 생물학적 지표로 사용되어 왔다.
특히 DHEA는 ACTH-regulated steoid로서 스트레스에 따른 anti-glucocorticoid property를 나타내므로 최근 스트레스에 대 한 민감도가 우수한 것으로 입증된 바 있다.8-9)
본 연구는 만성적인 스트레스와 대사증후군 사이의 연관성 을 생물학적 스트레스 지표인 코르티솔(cortisol), DHEA-S 및 코르티솔(cortisol)/DHEA-S로 알아 보고자 하였다.
본 연구의 결과에서 코르티솔(cortisol)은 공복혈당과 양의 상관관계를 보였으나 그외의 대사증후군 요소와는 통계학적 유의성이 없었고 독립표본 T-test에서도 유의한 평균 차이를 보이는 요소는 없었다. DHEA-S는 중성지방과 음의 상관관계 를 보였으며, 독립표본 T-test에서 체질량지수, 공복혈당, 중성 지방, HDL 콜레스테롤의 분리 점에서 유의한 평균 차이를 볼 수 있었다.
급성 스트레스로 유발된 Hyper코르티솔(cortisol)ism은 고혈 당, 비만, 고중성지질혈증, 낮은 HDL 콜레스테롤과 상관성을
보인다.23-24) 또한 만성적인 스트레스 노출로 반복되는 부신피
질자극호르몬의 분비는 부신의 민감성을 증가 시켜 분비되는 코르티솔(cortisol)의 양을 증가 시킬 수 있다.25) 본 연구에서는 대사증후군과 연관된 비만 관련 인자나 이상지혈증이 코르티 솔(cortisol)과는 연관성이 없는 것으로 나타났으나 향후 코르 티솔(cortisol)의 일주기에 따른 측정방법을 통해 그 관련성을 확인해야 할 것으로 생각된다. 반면 코르티솔(cortisol)과 공복 혈당간의 양의 상관관계 결과는 만성적인 스트레스 노출에 의 해 증가된 새벽의 코르티솔(cortisol) 레벨이 오전 공복시에 측 정되는 혈당치에 영향을 주어 나타난 결과로 생각되어 진다.
DHEA 역시 부신피질자극호르몬에 의해 분비되는 부신 피 질의 스테로이드 호르몬이다.26)
혈청 DHEA와 DHEA-S의 나이와 연관된 현저한 감소는 노 화와 관련된 질환들과 원인적 연관성이 있을 수 있다는 것을 시사한다.27) 체질량지수와 DHEA 간에는음의 상관 관계를 보 이는 것으로 여겨지지만28-30), DHEA-S의 경우 그 결과가 일치 하지 않는다.
Barrett-Connor 와 Ferrara는 659명의 폐경후 여성을 대상으로 한 연구에서 체질량지수와 DHEA-S간에 음의 상관관계(r=-0.06) 를 보인다고 하였다.29) 본 연구에서 체질량지수와 DHEA-S간에 Pearson 상관계수는 -0.068이었으나 통계학적 유의성은 없었다 (p=0.303). 이는 폐경 후 특정 연령의 여성만을 대상으로 한 연 구 자료의 한계성으로 생각된다.
본 연구에서는 복부비만의 진단 지표로 사용되었어야 할 허 리둘레 대신 체질량지수를 사용하였다. 체질량지수 역시 여러
연구에서 당뇨의 발생과 대사 이상 등을 예측하는데 좋은 결과 를 보였다.31-34) 그러나 대사증후군의 요소인 허리 둘레를 체질 량지수로 대체한 것이 본연구의 한계성의 하나임을 인정할 수 밖에 없다.
이상에서 살펴본 본 연구의 제한 점은 다음과 같다. 1) 단면연 구이기 때문에 만성스트레스와 대사증후군간의 인과관계에 대 한 설득력이 부족하며 선택편견의 오류 가능성을 배제할 수 없 다. 2)코르티솔(cortisol)의 측정 방법이 일중변동을 반영하지 못 하였다. 3) DHEA-S의 결과 해석에 노화에 따른 연령의 영향이 있을 수 있다. 4) 체질량지수를 허리둘레의 대체 지표로 사용한 것에 이의를 제기할 수 있다. 그러나 본 연구가 만성 스트레스와 대사증후군 간의 선후 관계를 명확히 입증할 수는 없으나 대사 증후군의 요소와 연관된 DHEA-S의 유의한 차이는 만성스트레 스와 대사증후군간의 연관 가능성을 시사한다고 볼 수 있다.
이는 대사증후군 등의 유발에 정신적인 스트레스가 영향을 미친다는 것을 간과해서는 안됨을 주지시키고 있으며 이를 위한 향후 코르티솔(cortisol)및 DHEA의 일중 변동을 고려한 대규모의 전향적 연구가 필요할 것이다.
요 약 연구배경
대사증후군의 핵심 병리기전은 인슐린 저항성이다. 만성스 트레스는 뇌하수체-시상하부-부신 축의 활성화로 코르티솔 (cortisol) 수치의 증가를 유발하여 혈당상승, 인슐린 저항성의 증가 및 혈압의 상승을 초래할 수 있다. 이에 우리는 폐경이 란 특수 상황을 공통적으로 겪은 폐경후 여성을 대상으로 대 사증후군의 요소와 생물학적 스트레스 지표인 코르티솔 (cortisol), dehydroepiandrosterone(DHEA-S), 그리고 코르티 솔(cortisol)/DHEA-S와의 연관성에 대해 알아보고자 하였다.
방 법
2001년 1월부터 2008년 3월까지 서울시내 일개 종합병원에 스트레스를 주소로 내원한 폐경후 여성 223명을 대상으로 하 였다. 대사증후군은 NCEP-ATP III 진단기준을 적용하되 허 리둘레 대신 체질량지수를 사용하였다. 생물학적 스트레스 지표들과 대사증후군의 요소과의 상관성에 대해 확인하였다.
결 과
공복혈당은 코르티솔(cortisol)과 양의 상관관계(p=0.01)를
보이고 중성지방과 DHEA-S간에는 음의 상관관계(p=0.019)를 보였다. 대사증후군의 요소 각각에 대해 정의에 따른 분리점을 사용하여 두 군으로 나누어 생물학적 지표의 두 집단 간 평균 비교를 했을 때 DHEA-S만이 혈압을 제외한 네 가지 요소에서 유의한 평균 차이(체질량지수, p=0.022; 공복혈당, p=0.004; 중 성지방, p=0.012; HDL-C, p=0.010)를 보였다. 대상환자를 정상 과 대사증후군으로 구분하여 비교하였을 때 DHEA-S와 코르티 솔(cortisol)/DHEA-S의 집단간 평균이 유의(p<0.001, p=0.039) 한 차이가 있었다.
결 론
본 연구 결과가 만성 스트레스와 대사증후군 간의 인과 관 계를 명확히 밝힐 수는 없으나 DHEA-S의 대사증후군의 요소 증가에 따른 유의한 차이와 각 요소와의 관련성은 만성스트레 스와 대사증후군간의 밀접한 연관성을 시사한다고 볼 수 있다.
향후 대규모의 구체화된 실험적 연구가 필요할 것이다.
중심단어
대사증후군, 스트레스, 코르티솔, DHEA-S, 코르티솔(cortisol)/
DHEA-S
참고문헌
1. Lakka HM, Laaksonen DE, Lakka TA, Niskanen LK, Kumpusalo E, Tuomilehto J, Salonen JT. The metabolic syndrome and total and cardiovascular disease mortality in middle-aged men. JAMA.
2002;288:2709-16.
2. Laaksonen DE, Lakka HM, Niskanen KL, Kaplan GA, Salonen JT, Lakka TA. Metabolic syndrome and development of diabetes:
application and validation of recently suggested definitions of the metabolic syndrome in a prospective Cohort study. Am J Epidemiol. 2002;156:1070-7.
3. Reaven GM. Banting lecture 1988. Role of insulin resistance in human disease. Diabetes. 1988;37:1595-607.
4. Hanley AJ, Wagenknecht LE, D’Agostino RB Jr, et al. Identification of subjects with insulin resistance and beta-cell dysfunction using alternative definitions of the metabolic syndrome. Diabetes.
2003;52:2740-7.
5. Brunner EJ, Hemingway H, Walker BR, et al. Adrenocortical, autonomic, and inflammatory causes of the metabolic syndrome:
nested case-control study. Circulation. 2002;106:2659-65.
6. Rosmond R. Role of stress in the pathogenesis of the metabolic syndrome. Psychoneuroendocrinology. 2005;30:1-10.
7. Widmer IE, Puder JJ, Konig C, Pargger H, Zerkowski HR, Girard J, Muller B. cortisol response in relation to the severity of stress and illness. J Clin Endocrinol Metab. 2005;90:4579-86.
8. Yang Y, Koh D, Ng V, Lee FC, Chan G, Dong F, Chia SE.
Salivary cortisol levels and work-related stress among emergency department nurses. J Occup Environ Med. 2001;43:1011-8.
9. Morgan III CA, Southwick S, Hazlett G, Rasmusson A, Hoyt G, Zimolo Z, Charney D. Relationships among plasma dehydroepiandrosterone sulfate and cortisol levels, symptoms of dissociation, and objective performance in humans exposed to acute stress. Arch Gen Psychiatry. 2004;61:819-25.
10. Reaven GM, Lithell H, Landsberg L. Hypertension and associated metabolic abnormalities – the role of insulin resistance and the sympathoadrenal system. N Engl J Med. 1996;334:374-81.
11. Hjemdahl P. Stress and the metabolic syndrome; An interesting but enigmatic association. Circulation. 2002;106:2634-6.
12. Bujalska IJ, Kumar S, Stewart PM. Does central obesity reflect
"Cushing’s disease of the omentum"? Lancet. 1997;349:1210-3.
13. Bjorntorp P. Visceral obesity: a civilization syndrome. Obes Res.
1993;1:206-22.
14. Chrousos GP. The role of stress and the hypothalamic-pituitary-adrenal axis in the pathogenesis of the metabolic syndrome: neuro-endocrine and target tissue-related cause. Int J Obesity. 2000;24:50-5.
15. Chousos GP, Gold PW. The concepts of stress and stress system disorders. Overview of physical and behavioral homeostasis.
JAMA. 1992;267:1244-52.
16. McEwen BS. Protective and damaging effects of stress mediators.
N Engl J Med. 1998;338:171-9.
17. Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Executive summary of the third report of the National Cholesterol Education Program(NCEP) Expert Panel on Detection, Evaluation, and Treatments of High Blood Cholesterol in Adults(Adult Treatment Panel III).
JAMA.2001;285:2486-97.
18. Tsigos C, Chrousos GP. Hypothalamic-pituitary-adrenal axis, neuroendocrine factors and stress. J Psychosom Res. 2002;53:865-71.
19. Chrousos GP. Regulation and dysregulation of the hypothalamic-pituitary-adrenal axis: the corticotropin releasing hormone perspective. Endocrinol Metab Clin North Am.
1992;21:833-58.
20. Tsigos C, Chrousos GP. Physiology of the hypothalamic-pituitary-adrenal axis in health and dysregulation in psychiatric and autoimmune disorders. Endocrine Metab Clin North Am. 1994;23:451-66.
21. Rosmond R, Dallman MF, Bjorntorp P. Stress-related cortisol secretion in Men: relationships with abdominal obesity and endocrine, metabolic and hemodynamic abnormalities. J Clin Endocrinol Metab. 1998;83:1853-9.
22. Skilton MR, Moulin P, Terra JL, Bonnet F. Association between anxiety, depression, and the metabolic syndrome. Biol Psychiatry.
2007;62:1251-7.
23. Anuurad E, Shiwaku K, Nogi A, Kitajima K, Enkhmaa B, Shimono K, Yamane Y. The new BMI criteria for asian by the regional office for the western pacific region of WHO are suitable for screening of overweight to prevent metabolic syndrome in elder Japanese workers. J Occup Health. 2003;45:335-43.
24. Bjorntorp P, Rosmond R. Hypothalamic origin of the metabolic syndrome X. Ann NY Acad. 1999;892:297-307.
25. Laatikainen TJ. Corticotropin-releasing hormone and opioid peptides in reproduction and stress. Ann Med. 1991;23:489-96.
26. Nieschlag E, Loriaux DL, Ruder HJ, Zucker IR, Kirschner MA, Lipselt MB. The secretion of dehydroepiandrosterone and dehydroepiandrosterone sulphate in man. J Endocrinol.
1973;57:123-134.
27. Tchernof A, Labrie F. Dehydroepiandrosterone, obesity and cardiovascular disease risk: a review of human studies. Eur J Endocrinol. 2004;151:1-14.
28. De Pergola G, Zamboni M, Sciaraffia M, Turcato E, Pannacciulli N, Armellini F et al. Body fat accumulation is possibly responsible for lower dehydroepiandrosterone circulating levels in premenopausal obese women. Int J Obes Relat Metab Disord.
1996;20:1105-10.
29. Barrett-Connor E, Ferrara A. Dehydroepiandrosterone, dehydroepiandrosterone sulfate, obesity, waist-hip ratio, and noninsulin-dependent diabetes in postmenopausal women: the Rancho Bernado Study. J Clin Endocrinol Metab. 1996;81:59-64.
30. De Pergola G, Giagulli VA, Garruti G, Cospite MR, Giorgino F, Cignarelli M et al. Low dehydroepiandrosterone circulating levels in premenopausal obese women with very high body mass index. Metabolism 1991;40:187-90.
31. The Examination Committee of Criteria for "Obesity Disease" in Japan. Japan Society for Study of Obesity. New Criteria for
"Obesity Disease" in Japan. Cir J 2002;66:987-92.
32. Shen W, Punyanitys M, Chen J, Gallagher D, Albu J, Pi-Sunyer X, Lewis CE, Grunfeld C, Heshka S,Heymsfield SB. Waist circumference correlates with metabolic syndrome indicates better than percentage fat. Obesity. 2006;14:727-36.
33. Sung KC, Ryu S, Reaven GM. Relationship between obesity and several cardiovascular disease risk factors in apparently healthy Korean individuals: Comparison of body mass index and waist circumference. Metabolism Clinical and Experimental. 2007;56:297-303.
34. Farin Helke M.F., Abbasi F, Reaven GM. Comparison of body mass index versus waist circumference with the metabolic changes that increase the risk of cardiovascular disease in insulin resistant individuals. Am J Cardiol. 2006;98:1053-6.