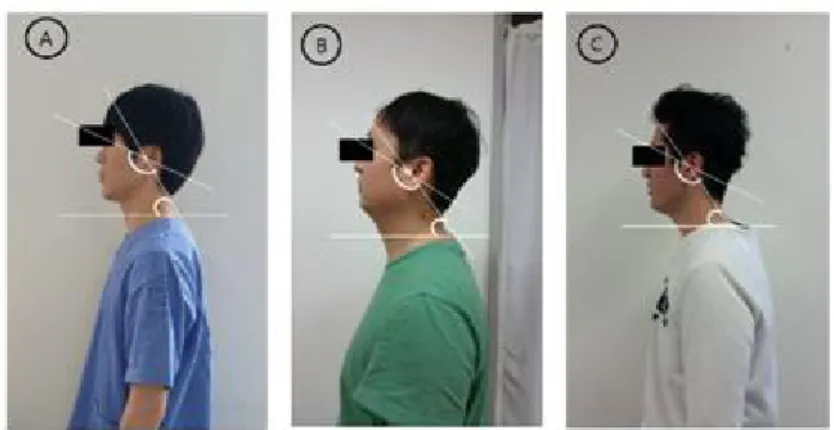
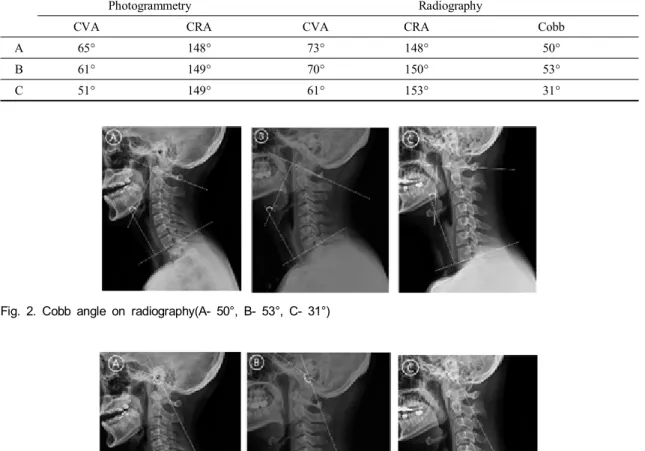
The Exception Case about the Diagnose Forward Head Posture using the CranioVertebra Angle, CranioRotation Angle and Cobb angle : a Case Report
6
0
0
전체 글
(2)
(3)
(4)
(5)
(6)
수치
관련 문서
In this study, the dislocation group had a wider width of AEB (p<0.05), and the posterior slope (TR angle) of the AER and the average of AEB were smoother (p<0.05) compared
Based on the above results, the 12-week complex type correction program had a positive effect on the shoulder angle, trunk rotation angle, and body shape
Melt lamination process, depending on the characteristics Floor laminate Out-of-Plane so the mechanical properties of the products according to the angle
When the fiber orientation angle is small, the member absorbed energy by laminar bending.. As the fiber orientation angle increases, the member was
To develope the water purifying system using the economical solar thermal energy, the box with the tilted angle of 15 o , 30 o , 45 o , 60 o and same basic area was
chair and boat conformation (free of angle strain); not planer with 120° bond angle (fully eclipsed). planer with 120 bond
Bent posture, and as a fast check of the measurement major pectoral muscle case, the patient lying immediately behind the head comes along,
(a) Low-Angle and High-Angle Boundaries (b) Special High-Angle Grain Boundaries (c) Equilibrium in
