대한화상학회지 제 14 권 제 1 호
39
Journal of Korean Burn SocietyVol. 14, No. 1, 39-42, 2011
책임저자:장영호, 대구시 남구 대명2동 2033-12
705-821, 대구푸른병원 마취통증의학과 Tel: 053-471-2800, Fax: 053-471-2806 E-mail: [email protected]
소아 화상 환자에서 Sevoflurane 마취 후 발생되는 술 후 각성 흥분
장영호ㆍ김상규
1ㆍ손용훈
1ㆍ박준모
1ㆍ이미영
2대구푸른병원 마취통증의학과, 1화상외과, 2계명대학교 의과대학 예방의학교실
Emergence Agitation after Sevoflurane Anesthesia in Burn Injured Children
Young Ho Jang, M.D., Ph.D., Sang Kyu Kim, M.D.
1, Yong Hoon Son, M.D.
1, Joon Mo Park, M.D.
1and Mi Young Lee, M.D., Ph.D.
2Departments of Anesthesiology and Pain Medicine, 1Burn Surgery, Pureun Hospital Burn Center, 2Department of Preventive Medicine, Keimyung University School of Medicine, Daegu, Korea
Purpose: Sevoflurane is a well accepted anesthetic in chil-
dren but results high incidence of undesirable emergence ag- itation (EA). We investigated the EA in burn injured children.Methods: In 219 un-premedicated burn injured children aged
2∼8 years, mask induction with sevoflurane was performed.On arriving operating room, modified Yale preoperative anxi- ety scale (m-YPAS) was checked. In the postanesthesia care unit, EA scale was recorded as follows; EA1 (no EA), EA2 (mild EA) and EA3 (marked EA).
Results: The incidence of EA was 50.2%. The m-YPAS was
significantly higher in EA2 and EA3 compared to EA1 (P<0.001). Burn surface area was significantly wider in EA3 com- pared to EA1 (P<0.05). In deep second-degree burned chil- dren, the incidence of EA1 was greatest, whereas EA3 was the greatest in third-degree burned children.
Conclusion: The incidence of EA after sevoflurane anes-
thesia in burn injured children was higher as the burn surface areas was greater. In addition, the symptoms of EA in third-degree burned children were more severe than in sec- ond-degree burned children. (J Korean Burn Soc 2011;14:39-42)
Key Words: Burn, Children, Postoperative agitation, Sevoflurane
서 론
기도 자극이 적고 낮은 혈액/조직 용해도로 인한 빠른 마 취유도 및 회복의 특성으로 인하여
1), 소아 흡입마취에는 대 부분 sevoflurane이 사용되고 있다. 그러나 소아에서 sevo- flurane 마취 후 흔히 발생되는 임상 증상인 술 후 각성 흥분 (emergence agitation, EA)은 과거 사용된 흡입마취제인 halothane에 비하여 발생률이 매우 높아 최고 80%까지 보 고되고 있으며
2), 이는 환아 신체의 손상, 출혈, 정맥 카테터 의 발관, 회복실 퇴실 지연 등의 부작용을 초래할 수 있다
3,4). EA의 발생에는 마취전투약, 마취약제 및 마취 방법 등과 같은 마취과적인 요인들이 그 원인이 될 수 있으며, 수술의 종류 혹은 술 후 통증 등과 같은 외과적인 요인들에 의해서 도 영향을 받을 수 있다
5).
한편 화상 환자들에서 소아가 차지하는 비율이 과반수에 이르며 이의 절반 이상이 미취학 아동으로 보고되는데
6,7), 이들 소아 화상 환자들의 많은 경우에서 가피절제술 혹은 피부이식술 등을 위하여 수술 및 마취를 경험하게 된다. 그 러나 지금까지 소아 화상 환자들에 있어서 EA에 대한 연구 가 보고된 바 없으며, 따라서 본 연구에서는 화상으로 인하 여 수술 및 마취를 시행 받는 소아 환자들에서 나타나는 EA의 발생에 대하여 조사하고자 하였다.
대상 및 방법
본원에서 입원하여 수술적 치료를 받은 미국마취과학회 신체등급 I, II에 해당되는 2∼8세 소아 중 심재성 2도 화상 및 3도 화상이며 화상범위가 전체표면적의 20%이하인 환 자들을 대상으로 하였다. 과거 수술 경험이 있는 경우와 발 달장애 혹은 정신 질환이 있는 경우는 제외하였다. 수술 전 날 마스크를 이용한 환기법을 설명하였고, 술 전 4∼6시간 금식을 시행하였으며, 마취전투약(premedication)은 시행 하지 않았다.
모든 환자들은 정맥로를 확보하지 않고 마스크를 이용한
sevoflurane 흡입마취유도 및 유지를 시행하였다. 환자와
40
대한화상학회지 Vol. 14, No. 1, 2011Table 1. Emergence Agitation Scale
Scale Agitation status
1 No symptoms - no symptoms of agitation 2 Mild symptoms - occasional movement or crying,
no need for restraint 3 Marked symptoms - thrashing and/or needs
restraint and/or constant crying
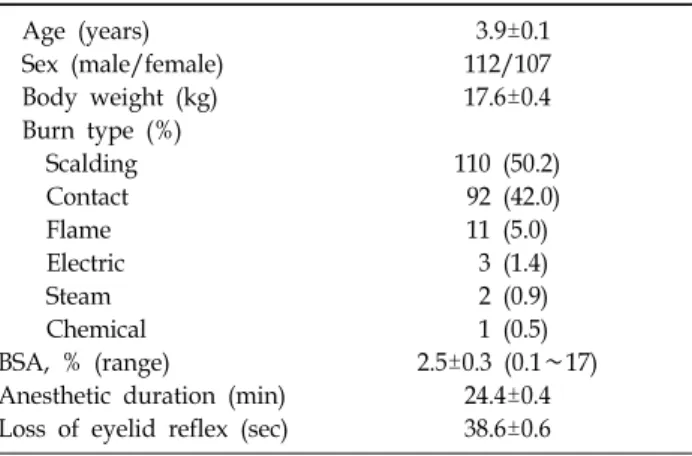
Table 2. Characteristics of Children, Burn, Anesthesia (n=
219)
Age (years) 3.9±0.1
Sex (male/female) 112/107
Body weight (kg) 17.6±0.4
Burn type (%)
Scalding 110 (50.2)
Contact 92 (42.0)
Flame 11 (5.0)
Electric 3 (1.4)
Steam 2 (0.9)
Chemical 1 (0.5)
BSA, % (range) 2.5±0.3 (0.1∼17)
Anesthetic duration (min) 24.4±0.4 Loss of eyelid reflex (sec) 38.6±0.6 BSA = body surface area (%)
Fig. 2. Emergence agitation (EA) and burn surface area (BSA).
EA1 = no EA, EA2 = mild EA, EA3 = marked EA. *P<0.05 vs.
EA1.
Fig. 1. Emergence agitation (EA) and preoperative anxiety.
mYPS = modified Yale preoperative anxiety scale, EA1 = no EA, EA2 = mild EA, EA3 = marked EA. *P<0.05 vs. EA1.
부모가 함께 수술실에 들어온 후 환자의 술 전 불안 정도를 변형된 Yale 술 전 불안 척도(modified Yale preoperative anxiety scale, m-YPAS)를
8)이용하여 평가한 다음, 마스크 환기를 시행하여 환자의 안검반사가 소실된 후 부모는 퇴 실하도록 하였다. 수술 및 마취 종료 후 발생되는 EA 정도 를 Table 1과 같이 무증상(no symptoms, EA1), 경등도 증 상(mild symptoms, EA2), 중등도 증상(marked symptoms, EA3)의 3등급으로 분류하였다
9). 각 점수는 마취에 관여하 지 않은 한 명의 간호사에 의하여 체크되었으며, 화상 범위 및 깊이에 따른 EA의 발생 차이에 대하여 조사하였다. 결 과 값은 SPSS 프로그램(SPSS for Windows, Release 12.0;
SPSS Inc, Chicago, IL, USA)으로 one-way ANOVA와 Chi- square test를 이용하여 비교하였으며, P값이 0.05 미만인 경우 의의 있는 것으로 판단하였다. EA 발생에 영향을 미 치는 인자들의 분석은 로지스틱 회귀분석으로 시행하였다.
결 과
2009년 6월부터 2010년 5월까지 219명의 소아 화상 환자 들이 대상이 되었다. 환자들의 평균 연령은 3.9±0.1세, 평균 체중은 17.6±0.4 kg이었으며, 성별은 남자가 112명, 여자가
107명이었다(Table 2). 화상의 종류는 열탕화상(50.2%)이 가장 많았으며 그 다음으로 접촉화상(42.0%), 화염화상 (5.0%) 등의 순이었다. 평균 화상 범위는 전체표면적의 2.5±
0.3%이었다. 마스크 적용 후 안검반사 소실까지는 평균 38.6±0.6초가 소요되었으며, 평균 마취 시간은 24.4±0.4분이 었다.
대상 환자들에서 EA2이 86명(39.3%), EA3가 24명(11.0%) 에서 나타나 총 110명(50.2%)에서 EA가 나타났다. EA1, EA2, EA3군에서 m-YPAS는 각각 56.5±2.0, 73.5±2.4 (P<
0.001 vs. EA1) 및 80.0±4.5 (P<0.001 vs. EA1)로 경등도 및 중등도의 EA가 발생된 환자에서 m-YPAS가 높게 측정되었 다(Fig. 1).
EA1, EA2 및 EA3에서 전체표면적에 대한 화상 범위는
각각 1.9±0.2%, 3.0±0.7% 및 4.3±0.9%로 EA3군에서 EA1군
장영호 등:소아 화상 환자에서 Sevoflurane 마취 후 발생되는 술 후 각성 흥분
41
Table 3. Emergence Agitation and Burn Depth
Burn depth EA1 EA2 EA3 Total
Deep second 104 (52.0%) 80 (40.0%) 16 (8.0%) 200 (100%)
Third 5 (26.3%) 6 (31.6%) 8 (42.1%) 19 (100%)
EA1 = no EA, EA2 = mild EA, EA3 = marked EA. P<0.001 with Chi-square test
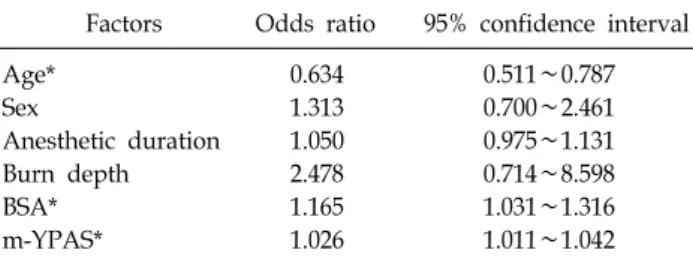
Table 4. Risk Factors of Emergency Agitation
Factors Odds ratio 95% confidence interval
Age* 0.634 0.511∼0.787
Sex 1.313 0.700∼2.461
Anesthetic duration 1.050 0.975∼1.131
Burn depth 2.478 0.714∼8.598
BSA* 1.165 1.031∼1.316
m-YPAS* 1.026 1.011∼1.042
BSA = burn surface area, m-YPAS = modified Yale pre- operative anxiety scale. *Indicates risk factors of emergency agitation by logistic regression
에 비하여 의의 있게 높았다(P<0.05) (Fig. 2).
심재성 2도 화상에서 EA1, EA2 및 EA3가 각각 52.0%, 40.0% 및 8.0%에서 발생되었으며, 3도 화상에서는 각각 26.3%, 31.6% 및 42.1%에서 발생되었다(Table 3).
EA 발생에 영향을 미치는 인자를 분석한 결과 연령, 화 상 범위 및 m-YPAS가 위험 인자로 나타났다(Table 4).
고 찰
소아에서 sevoflurane 마취 시 과거 사용된 halothane에 비하여 EA가 더욱 많이 발생되는데
10), 통증, 빠른 마취 회 복, 연령 등의 다양한 요인들이 그 원인이 되는 것으로 알려 지고 있다
11). EA는 미취학 아동에게 많이 발생되는데
12), 본 연구에서는 2∼8세의 미취학 소아 환자들을 대상으로 하여 EA 발생이 높은 연령들로 구성되었다. 본 연구 결과 50.2%
의 소아 환자들에서 경등도 및 중등도의 EA가 발생되었으 며 그 빈도는 기존의 소아들을 대상으로 한 보고들과 유사 하였다.
m-YPAS는 2세 이상 소아들에서 1분 이내에 술 전 불안 정도를 유용하게 측정하는 도구로 5개의 항목(anxiety, vo- calization, emotional expressivity, state of apparent arous- al, use of parents)으로 구성되어 있으며, 최하 28.5점에서 최고 100점으로 100점인 경우 불안 정도가 최고임을 의미 한다
13). 본 연구 대상 소아 환자들에서 EA가 발생된 경우에 서 EA가 발생되지 않은 군에 비하여 m-YPAS가 높게 나타
나 술 전 불안 정도가 EA 발생에 영향을 미치는 것으로 나 타났다. 이는 다변형 회귀분석에서도 m-YPAS이 EA 발생 에 영향을 미치는 인자로 확인할 수 있었다. 이러한 결과는 술 전 불안 정도가 EA 발생에 영향을 미친다는 다른 보고 들과 유사하다
9,14).
한편 소아 화상 환자에서 sevoflurane 마취 후 발생되는 EA에 대한 연구는 보고되지 않았다. 본 연구 대상의 소아 화상 환자에서 화상 범위와 EA 발생에 대한 연구 결과 EA 가 나타나지 않은 EA1군에 비하여 EA가 심하게 나타난 EA3군에서 화상 범위가 높았는데, 이는 화상 범위가 넓으 면 EA 증상이 심하게 나타남을 의미한다. 한편 심재성 2도 화상의 경우 48.0%의 환자에서 EA가 발생된 반면 3도 화상 의 경우에는 73.7%에서 EA가 발생되었다. 또한 심재성 2도 화상의 경우 EA 발생 환자들 중 경등도의 EA가 더욱 많이 발생된 반면에 3도 화상인 경우에는 중등도의 EA가 더욱 많이 발생되었다. 이러한 결과는 화상 깊이와 범위에 따라 EA 발생의 빈도 및 증상의 정도에 차이가 있음을 보여준 다.
술 후 통증이 EA 발생을 증가시킬 수 있다고 알려져 있
다
15-17). 본 연구에서 통증 정도를 직접 체크하지는 않았지
만 화상 정도가 심하고 넓을수록 EA 발생이 증가하고 증상 이 더욱 심하게 나타났는데 이러한 결과 역시 술 후 통증에 의한 것으로 추측된다.
소아에서 발생되는 EA는 sevoflurane과 같은 흡입마취 를 하는 경우에 비하여 propofol을 이용한 정맥마취를 하는 경우 발생 빈도가 감소한다고 알려져 있다
18). 그러나 본원 에서는 수술 시간이 비교적 짧고 간단한 시술을 하는 경우 환자 및 보호자의 불안감을 감소시키기 위하여 수 년 동안 정맥로를 확보하지 않은 상태로 전신마취를 시행해 오고 있다. 따라서 propofol을 이용한 정맥마취로 소아 화상 환 자에서 EA를 얼마나 효과적으로 감소시킬 수 있는지에 대 해서는 직접적으로 확인할 수 없었다.
한편 소아 환자에서 sevoflurane 마취 후 발생되는 EA를
감소시키기 위하여 마취전투약
19), 술 중 및 술 후 진통제의
투여
20), 마취 회복 직전 소량의 propofol 투여
21)등의 방법
들이 이용되고 있다. 본 연구 대상 환자들에서는 모두 전투
약이 시행되지 않았으며 정맥로를 확보하지 않은 전신마취
42
대한화상학회지 Vol. 14, No. 1, 2011를 시행하므로 술 중 및 술 후 진통제를 투여하지 않았다.
그러나 sevoflurane 마취 후 발생되는 EA를 줄이기 위해서 마취 유도 후 정맥로를 확보하고 진통제를 투여하거나 마 취회복 직전 정맥마취제인 propofol을 소량 투여하는 방법 도 고려해볼 수 있을 것으로 생각된다.
본 연구에서 성별, 연령, 마취시간, 화상 깊이, 화상 범위, 술 전 불안 정도 등의 인자가 EA 발생에 영향을 미치는가 에 대한 다변량 회귀분석 결과 연령, 화상 범위, 술 전 불안 정도가 EA 발생의 위험 인자가 됨을 알 수 있었다. 따라서 EA 발생 빈도가 높은 소아 환자에서 술 전 불안감 감소를 최소화하고 특히 화상 정도가 심하고 화상 범위가 넓은 환 자에서 EA 발생 및 이의 예방에 보다 신중을 기하여야 할 것으로 생각된다.
결 론
소아 화상 환자들에서 sevoflurane 마취 후 50.2%에서 EA가 발생되었다. EA의 발생은 술 전 불안 정도가 심할수 록 빈도가 증가하고 증상 정도가 심하였다. EA 발생 빈도 는 심재성 2도 화상에 비하여 3도 화상에서 높았으며, 화상 범위가 넓을수록 EA가 더욱 많이 발생되었다. 향후 화상 정도가 심하고 범위가 넓은 소아 환자들에서 sevoflurane 마취 후 발생될 수 있는 EA를 감소시키기 위한 다양한 방 법들을 고려해야 하겠다.
REFERENCES
1) Welborn LG, Hannallah RS, Norden JM, Ruttimann UE, Callan CM. Comparison of emergence and recovery charac- teristics of sevoflurane, desflurane, and halothane in pediatric ambulatory patients. Anesth Analg. 1996;83:917-920.
2) Cravero J, Surgenor S, Whalen K. Emergence agitation in paediatric patients after sevoflurane anaesthesia and no surgery: a comparison with halothane. Paediatr Anaesth.
2000;10:419-424.
3) Voepel-Lewis T, Malviya S, Tait AR. A prospective cohort study of emergence agitation in the pediatric postanesthesia care unit. Anesth Analg. 2003;96:1625-1630.
4) Uezono S, Goto T, Terui K, Ichinose F, Ishguro Y, Nakata Y, et al. Emergence agitation after sevoflurane versus propofol in pediatric patients. Anesth Analg. 2000;91:563-566.
5) Ozer Z, Görür K, Altunkan AA, Bilgin E, Camdeviren H, Oral U. Efficacy of tramadol versus meperidine for pain relief and safe recovery after adenotonsillectomy. Eur J Anaesthesiol 2003;20:920-924.
6) Brusselaers N, Monstrey S, Vogelaers D, Hoste E, Blot S.
Severe burn injury in Europe: a systemic review of the incidence, etiology, morbidity, and mortality. Crit Care. 2010;
14:R188.
7) D'Souza AL, Nelson NG, McKenzie LB. Pediatric burn injuries treated in US emergency departments between 1990 and 2006. Pediatrics. 2009;124:1424-1430.
8) Golden L, Pagala M, Sukhavasi S, Nagpal D, Ahmad A, Mahanta A. Giving toys to children reduces their anxiety about receiving premedication for surgery. Anesth Analg.
2006;102:1070-1072.
9) Keegan NJ, Yudkowitz FS, Bodian CA. Determination of the reliability of three scoring systems to evaluate children after general anaesthesia. Anaesthesia. 1995;50:200-202.
10) Kuratani N, Oi Y. Greater incidence of emergence agitation in children after sevoflurane anesthesia as compared with halothane: a meta-analysis of randomized controlled trials.
Anesthesiology. 2008;109:225-232.
11) Aono J, Ueda W, Mamiya K, Takimoto E, Manabe M. Greater incidence of delirium during recovery from sevoflurane anesthesia in preschool boys. Anesthesiology. 1997;87:1298- 1300.
12) Beskow A, Westrin P. Sevoflurane causes more postoperative agitation in children than does halothane. Acta Anaesthesiol Scand. 1999;43:536-541.
13) Kain ZN, Mayes LC, Cicchetti DV, Bagnall AL, Finley JD, Hofstadter MB. The Yale preoperative anxiety scale: how does it compare with a "gold standard"? Anesth Analg.
1997;85:783-788.
14) Aouad MT, Nasr VG. Emergence agitation in children: an update. Curr Opin Anaesthesiol. 2005;18:614-619.
15) Radtke FM, Franck M, Hagemann L, Seeling M, Wernecke KD, Spies CD. Risk factors for inadequate emergence after anesthesia: emergence delirium and hypoactive emergence.
Minerva Anesthesiol. 2010;76:394-403.
16) Aouad MT, Kanazi GE, Siddik-Sayyid SM, Gerges FJ, Rizk LB, Baraka AS. Preoperative caudal block emergence agitation in children following sevoflurane anesthesia. Acta Anaestheiolo Scand. 2005;49:300-304.
17) Weldon BC, Bell M, Craddock T. The effect of caudal analgesia on emergence agitation in children after sevoflurane versus halothane anesthesia. Anesth Analg. 2004;98:321-326.
18) Nakayama S, Furukawa H, Yanai H. Propofol reduces the incidence of emergence agitation in preschool-aged children as well as in school-aged children: a comparison with sevoflurane. J Anesth. 2007;21:19-23.
19) Karamaz A, Kaya S, Turhanoglu S, Ozyilmaz MA. Oral ketamine premedication can prevent emergence agitation in children after desflurane anaesthesia. Paediatr Anaesth.
2004;14:477-482.
20) Ghai B, Ram J, Chauhan S, Wig J. Effects of clonidine on recovery after sevoflurane anaesthesia in children undergoing cataract surgery. Anaesth Intensive Care. 2010;38:530-537.
21) Aouad MT, Yazbeck-Karam VG, Nasr VG, El-Khatib MF, Kanazi GE, Bleik JH. A single dose of propofol at the end of surgery for the prevention of emergence agitation in children undergoing strabismus surgery during sevoflurane anesthesia. Anesthesiology. 2007;107:733-738.