2008;22:1-7 □
종 설
□1 책임저자:원종호, 서울시 용산구 한남동 657
순천향대학교병원 내과, 140-743 Tel: 02-709-9203, Fax: 02-709-9200 E-mail: [email protected]
조혈모세포이식 영역에서의 세포치료
순천향대학교 의과대학 내과학교실 박 성 규ㆍ원 종 호
Cell Therapy in Hematopoietic Stem Cell Trans- plantation
Seong-Kyu Park, M.D. and Jong-Ho Won, M.D.
Department of Internal Medicine, Soonchunhyang University College of Medicine, Seoul, Korea
Mesenchymal stem cells (MSCs) are attractive not only in regenerative medicine but also for the treatment of graft- versus-host disease (GVHD). During stem cell transplan- tation, the damaged marrow stroma induced by conditioning regimen can be regained their function with cotransplantation of culture-expanded MSCs. So, MSCs are capable of enhan- cing hematopoietic cell engraftment owing to providing optimal environment for hematopoietic regeneration. MSCs have been shown to exert immunoregulatory activity in various studies.
In vitro data suggested that they inhibit T-cell proliferation
to alloantigens and mitogens and their effect is directed mainly at the level of cell proliferation. MSCs have started to be used in clinical trials for the prevention and treatment of GVHD after allogeneic stem cell transplantation. Some data suggested that cotransplantation of MSCs with hema- topoietic stem cells reduced the incidence and severity of GVHD and the remission of grade III-IV acute GVHD can be achieved after infusion of donor-derived MSCs. However, several problems need to be addressed before the therapeu- tical potential of MSCs can be realized, including the inves- tigation to characterize their phenotype, their mechanisms of action, and optimize their in vitro expansion for clinical use.
Conclusively, MSCs may be used for hematopoiesis enhan- cement, as GVHD prophylaxis, and for the treatment of severe acute GVHD. And further studies are required to evaluate their therapeutic potentials. (J Korean Soc Transplant 2008;
22:1-7)
Key Words: Mesenchymal stem cells, Hematopoietic stem
cell transplantation, Tissue repair, Immunosu- ppression, Graft-versus host disease
중심 단어: 중간엽줄기세포, 조혈모세포이식, 조직 복구, 면역억제, 이식편대숙주병
서 론
조혈모세포이식은 악성 혈액질환뿐만 아니라 일부 고형 암 및 선천성 대사이상 질환을 완치시킬 수 있는 치료법으 로 널리 사용되고 있다. 최근 조혈모세포이식 기법의 발달 로 이식의 범위가 넓어져 혈연간과 비혈연간 이식 또는 HLA (human leukocyte antigen) 불일치 공여자를 이용한 이 식이 증가하고 있으며, 고령자에서의 이식 역시 증가 추세 에 있다. 그러나 이식편대숙주병과 골수기능의 회복 지연 으로 인한 감염성 합병증 등은 여전히 치료에 연관된 사망 을 유발하는 주요 원인이다. 현재 여러 조혈성장인자와 새 로운 항생제의 도입으로 지지요법이 보다 효과적으로 이루 어지고 있으며, 다양한 면역억제제가 도입되고 약제간의 이상적인 조합에 대하여 많은 연구가 진행되고 있으나, 아 직 만족할 만한 성과를 거두지 못하고 있다.
인간의 골수 내에는 서로 다른 계통의 두 가지 줄기세포 들이 존재한다. 조혈모세포는 말초혈액을 구성하는 세포들 을 생산하며, 중간엽줄기세포는 조혈모세포의 분화를 보조 하는 골수의 간질결합조직(stromal connective tissue)을 구성 하고 다양한 중배엽성 조직의 근원세포로 역할을 한다.(1) 아직까지 중간엽줄기세포는 진정한 줄기세포로 보기에 어 려운 면들이 있고 세포 자체를 정의할 수 있는 명확한 기준 을 제시할 수 없지만, 성체 줄기세포의 일종으로 많은 연구 가 이루어지고 있다.
중간엽줄기세포는 Friedenstein 등(2)이 골수간질세포의
이식에 의한 골 형성을 연구하는 중 세포배양 용기의 바닥
에 부착하여 자라는 섬유아세포(fibroblast) 형태의 세포들을
처음 기술한 이후로 지방조직, 태아 간, 혈액, 폐, 제대혈 등
에서 발견되었다.(3-5) 중간엽줄기세포는 다양한 중배엽 조
직으로 분화가 가능하며, 배양조건에 따라 뼈, 연골, 근육, 지
방조직 등과 함께 골수 간질세포로의 분화가 가능하다.(6-8)
최근 중간엽줄기세포의 일종으로 nutrient poor medium에서
성장하는 multipotent adult progenitor cells (MAPCs)들은 내
배엽계, 중배엽계, 및 외배엽계 세포로 분화할 수 있다고 알
려졌다.(9,10) 이 세포들을 쥐의 배아줄기세포에 주입하거
나 방사선치료로 전처치한 면역결핍 쥐에서 정맥을 통하여 주입하는 경우 다중분화능(multipotential)을 확인할 수 있 다.(11) 이런 결과들은 재생의학분야에서 중간엽줄기세포 관련 연구의 타당성을 제공한다.
몇몇 조건에서 조직회복에 대한 중간엽줄기세포의 효과 는 우선적으로 paracrine 역할에 연관되어 나타나는 것으로 평가되며, 중간엽줄기세포 자체가 손상된 조직으로 이동하 여 생착한 후 해당 조직으로 분화되는 재생능력에 의한 것 이 아닌 것으로 보인다.(12) 이런 주장은 중간엽줄기세포가 연구대상에 투입된 후에 극소수만이 발견되고, 손상된 부 위에 제한적으로 발견된다는 in vivo tracking 연구(13,14)들 을 통하여 뒷받침되고 있다. 따라서 다양한 조건에서 최상 의 배양조건과 기능적 특성에 대한 보다 많은 연구가 필요 하다.
아직까지 중간엽줄기세포를 규정할 수 있는 단일 특정단 백은 발견되지 않았으며, 정의를 하기도 어렵다. 따라서 다 양한 계통으로 분화할 수 있는 능력을 기준하여 구분할 수 있으며, 세포표지자검사에서 조혈계통의 세포가 아니라는 증거로서 CD34, CD45, CD14, HLA-DR 등이 음성이고, CD73, CD90, CD105 양성이며, 보다 최근에 SSCA-1, SSCA-4 및 GD2 등이 표현된다는 것이 알려졌다.(15)
지난 10년간 재생의학(regenerative medicine) 분야에서 중 간엽줄기세포를 이용하여 심각한 손상을 입은 장기 또는 조직을 복구하고 기능적인 호전을 유도하려는 많은 노력이 있었다. 분절된 뼈 손상을 입은 쥐 모델에서 뼈의 재생을 위하여 사람의 중간엽줄기세포를 이용한 실험(16)이 있었 으며, 배양 증식된 중간엽줄기세포가 관절내 연골 손상을 회복시키고, 아킬레스(Achilles)건의 파열 손상을 복구시킨 예도 있었다.(17,18) 뼈 질환에 대한 중간엽줄기세포의 효과 를 평가한 임상연구 중 골형성부전증(osteogenesis imper- fecta) 환자들을 대상으로 진행된 연구(19)에서 중간엽줄기 세포의 생착을 확인하였으며, 무기질 양과 뼈 증식속도의 증가가 있어 골절과 같은 뼈 관련 합병증의 빈도가 현저하 게 줄었다. 그러나 장기간 추적관찰에서는 성장속도가 정 상인에 비하여 저하되었으며, 질병을 앓고 있는 다른 환자 에 비해서도 차이가 없는 것으로 확인되었다. 그 외에 다른 질환에 대한 연구도 다수 진행되었는데, 허혈성 손상에 의 한 신장 손상(12)과 특정약물에 의한 폐 손상(20)이 있는 동 물모델에서 중간엽줄기세포를 투여한 후 손상부위가 감소 되었고 상처의 회복을 촉진되었다는 보고가 있었다. 보다 최근에 진행된 심근경색의 연구(21)에서는 관상동맥형성술 후 손상된 부위에 중간엽줄기세포를 투여하여 심기능이 현 저하게 향상되었다는 보고가 있으며, 현재도 대규모의 임 상연구가 진행되고 있다.
본 론
1) 조혈 영역에서의 중간엽줄기세포의 역할
골수 간질세포들은 세포간의 접촉 또는 조혈성장인자, 특정 생화학물질, 세포외기질 분자(extracellular matrix mole- cule)들의 분비를 통하여 조혈모세포의 생존, 자기복제, 이 동 및 분화에 관여한다. 골수 간질은 조혈모세포로부터 유 래한 대식세포와 함께 중간엽줄기세포로부터 유래한 지방 세포, 골세포, 망상세포들에 의하여 구성되며, 골수 내부의 3차원 망상구조를 형성한다.(22) 따라서 중간엽줄기세포는 조혈을 보조하며, 분화된 간질세포의 공급원으로서 중요한 역할을 하고 있다. Gene array 분석에서 중간엽줄기세포는 발생단계와 줄기세포 기능에 관련한 여러 특이유전자를 발 현하는 것을 확인하였다.(23) 또한, 최근 골내막성 골아세포 와 유사한 세포들이 조혈모세포의 성장과 밀접한 관계가 있고, 부갑상선 호르몬을 투여하여 골수 내에 골아세포의 수가 증가하는 경우 조혈모세포가 선택적으로 증식하는 것 이 확인되었다.(24) 특히 N-cadherin을 발현하는 골아세포가 조혈모세포의 자기복제를 조절하는 중요인자로 작용하는 것으로 보이며, 조혈모세포를 세포주기 중 정지기에 머물 게 하는 작용에는 Notch와 Tie-2/Ang 1 신호전달계가 관여 하는 것으로 보인다.(25,26)
반복적인 항암화학요법과 방사선요법은 골수 미세 환경 을 손상시키며, 조혈기능을 저하시키거나 기능회복을 지연 시킨다는 것이 알려졌다.(28,29) 골수 미세 환경 손상에 의 한 골수기능의 회복 지연은 치명적인 감염성 합병증을 유 발할 수 있어 치료에 연관된 사망률 증가로 직결된다. 특히, 최근 평균 여명이 길어지면서 악성 혈액질환을 앓고 있는 고령의 환자가 현저하게 증가하는 추세에 있어 이들을 대 상으로 최선의 치료법을 선택하는데 여러 어려움이 있다.
조혈모세포이식 분야에서 전 처치 방법으로 고용량의 항
암화학요법과 방사선요법을 사용하기 때문에 골수 미세 환
경 손상은 심각한 수준으로 발생하며, 때로 적정 수준의 조
혈을 유지하지 못하는 경우도 발생한다.(27,28) 이런 종류의
손상은 상당히 오랫동안 지속되는데, 심지어는 12년 후에
도 조혈 기능이 정상으로 회복되지 못하여 colony-forming
units-fibroblast (CFU-F)의 수가 정상으로 회복되지 못한다
는 보고도 있다.(29) 또한, CFU-F 수의 감소는 뼈의 무기물
농도 및 long-term culture-initiating cells (LTC-IC) 수의 감소
와 연관성이 있다. 자가 조혈모세포이식을 시행 받은 환자
에서도 조혈성장인자의 생산 장애는 이식 후 1년 이상 지속
되기도 한다. 따라서 적절한 조혈기능을 위하여 손상된 골
수의 간질세포는 재생되어야 한다.(29) 그러나 조혈모세포
이식 과정 중에 공여자로부터 이식되는 중간엽줄기세포의
수는 극히 제한적이기 때문에 이식 후 환자의 골수 내에
존재하는 간질세포는 환자에서 유래한 세포만이 존재하고
공여자로부터 유래한 세포는 확인되지 않는다.(30,31) 최근 골수에서 유래한 중간엽 줄기세포를 분리하여 체외 증식시킬 수 있는 방법이 개발되었다. 이 방법으로 증식된 세포들은 체외에서 모세포의 특징을 소실하지 않으면서 증 식할 수 있고, 골원성(osteogenic), 연골성(chondrogenic), 지 방성(adipogenic) 등으로 분화가 가능하며 골수의 간질세포 계로 분화도 가능하다. 따라서 조혈영역에서 중간엽줄기세 포는 손상된 간질세포를 보충하며, 적절한 미세 환경을 만 들기 위한 좋은 대안으로 인식되었고, 여러 동물연구와 임 상연구가 진행되었다.
여러 동물모델에서 방사선 전 처치 후에 공여자의 조혈 모세포와 함께 중간엽줄기세포를 이식하는 경우 조혈기능 이 조기에 회복된 보고들이 있다.(32,33) In vitro 연구에서도 유사한 결과를 얻을 수 있는데, Dexter 배양 중에 골수 간질 세포들을 조혈모세포와 함께 배양하는 경우 조혈을 6개월 이상 유지할 수 있다.(34) 간질세포의 보조 역할은 어떤 특 정 세포 계에 국한되지 않는데, 이에 대한 정확한 작용기전 은 규명되지 않았다. 일부 major histocompatibility complex (MHC) 항원에 의하여 영향을 받는 것으로 보이며, MHC 불 일치 간질세포와 배양하는 경우에 cobble stone 집락형성이 MHC 일치의 경우에 비하여 현저하게 줄었다는 보고가 있 다.(35)
저자가 참여한 조혈모세포의 생착에 대한 중간엽줄기세 포의 역할을 분석한 연구(34)에서 조혈모세포와 중간엽줄 기세포를 동시 이식한 경우가 보다 효율적이고 성공적으로 조혈모세포의 생착이 이루어졌으며, 이식된 중간엽줄기세 포의 양도 생착률에 영향을 준다는 것을 알 수 있었다. 이종 조혈모세포이식(xeno-transplantation) 모델을 이용한 이 연 구에서 이식된 중간엽줄기세포의 분포를 확인하기 위하여 사람의 Y 염색체에 대한 FISH 검사를 시행하였으며, 골수 를 비롯하여 비장, 간, 폐, 신장, 심장, 장, 피부 등의 다양한 장기에서 이식된 중간엽줄기세포를 확인하였다.
중간엽줄기세포를 이용한 초기 임상연구(36)에서 유방암 환자에서 체외에서 배양 증식된 자가 중간엽줄기세포를 조 혈모세포와 함께 이식할 때 골수기능 회복이 의미 있게 단 축되었으며, 주요 부작용은 없었다. 그러나 동종 조혈모세 포이식 분야에서 골수기능의 조기 회복에 대한 중간엽줄기 세포의 역할은 아직 확인되지 않았으며, 대부분의 연구들 이 결론을 얻기에는 연구 규모가 작고, 무작위 연구가 아니 며, 전 처치 방법들이 차이를 보이고 있어 향후 중간엽줄기 세포가 동종 조혈모세포이식 후에 골수기능을 조기에 회복 시킬 수 있는지 여부에 대한 대규모의 무작위 연구가 필요 하다.
2) 면역계에 대한 중간엽줄기세포의 역할
이식편대숙주병은 동종 조혈모세포이식의 성공을 저해 하는 가장 중요한 요인으로 지금까지 다양한 면역억제제의
도입에도 불구하고 이식분야에서 극복해야 할 우선 과제로 인식되고 있다. 최근, 중간엽줄기세포의 면역억제 기능을 이용하여 이식편대숙주병을 조절하고자 하는 노력이 있었 으며, 초기 동물연구에 이어 임상연구까지 진행되고 있다.
중간엽줄기세포의 면역조절능력에 대한 정확한 작용기 전이 알려지지 않았다. 사람, 쥐, 영장류를 대상으로 한 연 구들에서 공통적으로 나타나는 중간엽줄기세포의 성격은 mitogen과 다클론성 항원 또는 자극에 대한 T 림프구의 반 응을 억제하는 것이다.(37,38) 이런 반응은 항원에 대한 특 이 반응이 아니며 비선택적이다. 중간엽줄기세포에 의한 증식억제 측면에서 memory T 세포나 naive T 세포가 동일 한 정도로 억제되고, CD4 양성세포나 CD8 양성세포에서도 비슷한 영향을 받으며, B 세포의 증식에도 유사한 효과를 나타내는 것(39)으로 보아 이를 추정할 수 있다. 또한, 중간 엽줄기세포는 interleukin-2에 의해 유도된 자연 살해(natural killer, NK) 세포의 증식도 억제시킬 수 있다.(40)
최근 중간엽줄기세포가 면역관용을 유도하는 작용기전 을 추정할 만한 몇 가지 근거들이 제시되었다. 첫째, 중간엽 줄기세포는 항원제시세포(antigen presenting cell)를 억제하 는 효과가 있다. 비록 연구 초기에 항원제시세포는 중간엽 줄기세포와 관련된 면역억제 효과에 필요하지 않은 것으로 보였으나, 일부 특정 조건에서 배양과정 중 첨가된 단핵구 수에 비례하여 면역반응 정도가 변하는 것으로 보아 결국 단 핵구가 면역억제효과에 관여하는 것으로 추정된다.(41,42) 중간엽줄기세포와 함께 배양되는 단핵구들은 GM-CSF (granulocyte macrophage colony stimulating factor)와 interleu- kin-4에 의하여 자극되었을 때 수지상세포로 분화되지 않는 데, 이들 세포들은 항원제시세포로서 기능을 상실하게 된 다. 사이토카인 분비에 있어 이런 단핵구들은 regulatory T 세포를 유도하는 강력한 물질인 interleukin-10을 생산함으 로써 면역관용을 유도하게 된다. 따라서 근래에 중간엽줄 기세포에 의한 면역관용 유도의 작용기전으로 관심을 끌었 던 regulatory T 세포의 중요성은 상대적으로 감소되고 있 다. 더욱이 중간엽줄기세포가 CD4+/CD25+ regulatory T 세포나 항원제시세포 없이도 직접적으로 T 세포에 억제효 과를 나타낸다는 보고가 있어 주요 작용기전이 아닌 것으 로 생각된다.(43)
둘째 기전으로 중간엽줄기세포가 T 세포의 증식속도를
조절함으로써 면역억제 효과를 나타내는 것으로 보인다. T
세포를 중간엽줄기세포와 함께 배양하는 경우 cyclin D2가
억제됨에 따라 T 세포가 세포주기 중 G0/G1 시기에 머물러
더 이상 증식하지 않는다. 설사 중간엽줄기세포를 제거한
다 하더라도 증식능력은 지속적으로 저하되어 있다.(44) 그
러나 여러 자극에 반응하여 인터페론감마를 생산하는 T 세
포의 능력은 회복될 수 있다. 이런 효과는 NK 세포의 세포
독성에 영향을 주지 못하는 것으로 보이며,(40) 다른 조직
에서 유래한 세포들에서도 유사한 효과가 나타난다. 이상
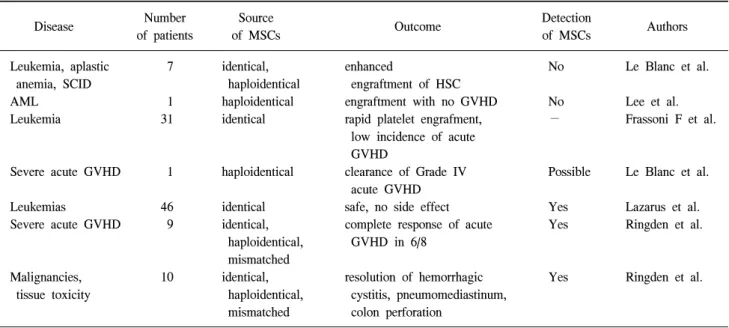
Table 1. In vivo experience of human mesenchymal stem cells (MSCs)
Number Source Detection
Disease Outcome Authors
of patients of MSCs of MSCs
Leukemia, aplastic 7 identical, enhanced No Le Blanc et al.
anemia, SCID haploidentical engraftment of HSC
AML 1 haploidentical engraftment with no GVHD No Lee et al.
Leukemia 31 identical rapid platelet engrafment, − Frassoni F et al.
low incidence of acute GVHD
Severe acute GVHD 1 haploidentical clearance of Grade IV Possible Le Blanc et al.
acute GVHD
Leukemias 46 identical safe, no side effect Yes Lazarus et al.
Severe acute GVHD 9 identical, complete response of acute Yes Ringden et al.
haploidentical, GVHD in 6/8 mismatched
Malignancies, 10 identical, resolution of hemorrhagic Yes Ringden et al.
tissue toxicity haploidentical, cystitis, pneumomediastinum, mismatched colon perforation
GVHD = graft-versus-host disease; SCID = severe combined immunodeficiency; AML = acute myelogenous leukemia; HSC = hematopoietic stem cell.
의 결과로 보아 중간엽줄기세포의 면역억제효과는 주로 비 특이적인 증식억제효과에 의한 현상으로 보이며, 이에 관 련한 기전은 아직 명확하게 규명되지 않았다. 몇몇 동물연 구와 임상연구에서 증식억제효과에 관여하는 TGF-β, indoleamine deoxydase, prostaglandin-E2, nitric oxide, insulin- like growth factor binding proteins 등의 soluble factor들이 알 려져 있으며,(45) 이들 물질의 분비는 간질세포를 포함하는 미세 환경에 의하여 영향을 받을 수 있기 때문에 결국 미세 환경의 변화가 중간엽줄기세포의 분화능력뿐만 아니라 그 들의 증식억제효과에도 영향을 미치는 가장 근본적인 요인 이라고 할 수 있다.
중간엽줄기세포의 면역억제 효과는 자가 면역성 질환의 동물모델을 통하여 성공적으로 평가되었으나 모든 경우에 서 일관된 효과가 나타나지는 않았다. 초기 연구에서 중간 엽줄기세포의 투입은 동종 조혈모세포이식 후 공여자의 조 혈모세포의 생착을 도왔을 뿐만 아니라 이식편대숙주병 (graft-versus-host disease; GVHD)을 억제하는 효과가 있다고 보고하였으나,(46,47) 다른 연구에서는 의미 있는 효과를 확 인할 수 없었다.(48) 이후 진행된 연구(49)에서 중간엽줄기 세포의 효과는 반복하여 투여한 경우에서 보다 두드러지게 나타남으로써 투여한 중간엽줄기세포의 용량이 치료 성공 여부를 판가름하는 중요한 요인으로 판단되었다.
조혈모세포이식 모델의 경우(50)에서 주조직적합항원이 불일치하는 쥐에 조혈모세포와 함께 중간엽줄기세포를 이 식하는 경우, 치명적인 이식편대숙주병의 예방과 장기 생 존이 가능한지 여부를 평가하는 연구가 진행되었다. 중간
엽줄기세포가 이식된 경우에서 이식편대숙주병의 빈도와 정도가 경감되어 장기 생존이 가능하였으며, 인터페론감마 의 혈중 농도가 의미 있는 차이를 보였다. 결론적으로 중간 엽줄기세포의 투여가 치명적인 이식편대숙주병을 예방하 는 것으로 보아 중간엽줄기세포의 면역조절 능력을 확인할 수 있었다.
현재까지 진행된 임상연구들은 대부분 소규모이고, 다양 한 환자를 대상으로 여러 치료법들이 사용되었기 때문에 중간엽줄기세포의 효과에 대하여 객관적인 평가에 어려움 이 있다. 주요 임상연구를 정리하면 Table 1과 같다.(51) 다 기관 연구로 진행된 Lazarus 등의 연구(48)에서 46명을 대상 으로 혈연간 공여자의 중간엽줄기세포를 배양 증폭시킨 후 조혈모세포이식과 동시에 투여하였을 때 급성 이식편대숙 주병은 13명(28%)에서 발생하였으며, 만성의 경우는 22명 (61%)에서 발생하였다. 2년 무병생존률은 53%이었으며, 중 간엽줄기세포 투여에 따른 부작용은 없었다. 검사가 가능 하였던 19명 중 2명에서 간질세포의 chimerism이 확인되었 다.
이상의 연구에서 종합해 보면, 중간엽줄기세포의 효과는
일관되게 나타나지 않았으며, 중간엽줄기세포에 관련된 대
부분의 정보가 in vitro 연구를 통하여 얻어진 것이기 때문
에 임상적 응용에 한계가 있었다. 따라서 중간엽줄기세포
의 효과를 극대화하기 위한 이상적인 조건, 즉 세포 수와
투여의 회수 및 다른 면역억제제와의 이상적인 조합 등에
대한 추가적인 연구가 필요하다.
결 론
중간엽줄기세포의 다중분화능과 면역조절 능력은 조혈 모세포이식 분야에서 치료에 연관된 주요 사망원인인 이식 편대숙주병과 골수기능부전을 극복할 수 있는 유용한 치료 대안이 될 수 있다. 향후 in vitro 실험과 실험적인 동물연구 및 다양한 임상연구들을 통하여 축적된 정보와 경험을 바 탕으로 잘 계획된 임상연구들이 기대된다.
REFERENCES
1) Majumdar MK, Thiede MA, Mosca JD, Moorman M, Gerson SL. Phenotype and functional comparison of cultures of marrow-derived mesenchymal stem cells (MSCs) and stromal cells. J Cell Physiol 1998;176:57-66.
2) Friedensen A. Stromal mechanism of bone marrow; cloning in vitro and retransplantation in vivo. Immunology of Bone Marrow Transplantation. Berlin, Splinger-Verlag; 1980. p19-20.
3) De Ugarte DA, Morizono K, Elbarbary A, Alfonso Z, Zuk PA, Zhu M, Dragoo JL, Ashjian P, Thomas B, Benhaim P, Chen I, Fraser J, Hedrick MH. Comparison of multilineage cells from human adipose tissue and bone marrow. Cells Tissues Organs 2003;174:101-9.
4) Campagnoli C, Roberts IA, Kumar S, Bennett PR, Bellantuono I, Fisk NM. Identification of mesenchymal stem/progenitor cells in human first-trimester fetal blood, liver, and bone marrow.
Blood 2001;98:2396-402.
5) Noort WA, Kruisselbrink AB, in't Anker PS, Kruger M, van Bezooijen RL, de Paus RA, Heemskerk MH, Löwik CW, Falkenburg JH, Willemze R, Fibbe WE. Mesenchymal stem cells promote engraftment of human umbilical cord blood- derived CD34cells in NOD/SCID mice. Exp Hematol 2002;
30:870-8.
6) Haynesworth SE, Goshima J, Goldberg VM, Caplan AI.
Characterization of cells with osteogenic potential from human marrow. Bone 1992;13:81-8.
7) Pittenger MF, Mackay AM, Beck SC, Jaiswal RK, Douglas R, Mosca JD, Moorman MA, Simonetti DW, Craig S, Marshak DR. Multilineage potential of human mesenchymal stem cells.
Science 1999;284:143-7.
8) Prockop DJ. Marrow stromal cells as stem cells for nonhema- topoietic tissues. Science 1997;276:71-4.
9) Krabbe C, Zimmer J, Meyer M. Neural transdifferentiation of mesenchymal stem cells-a critical review. Apmis 2005;113:
831-44.
10) Laflamme MA, Murry CE. Regenerating the heart. Nat Biotechnol 2005;23:845-56.
11) Jiang Y, Jahagirdar BN, Reinhardt RL, Schwartz RE, Keene CD, Ortiz-Gonzalez XR, Reyes M, Lenvik T, Lund T, Blackstad M, Du J, Aldrich S, Lisberg A, Low WC, Largaespada DA,
Verfaillie CM. Pluripotency of mesenchymal stem cells derived from adult marrow. Nature 2002;418:41-9.
12) Tögel F, Hu Z, Weiss K, Isaac J, Lange C, Westenfelder C.
Administered mesenchymal stem cells protect against ischemic acute renal failure through differentiation-independent mecha- nisms. Am J Physiol Renal Physiol 2005;289:F31-F42.
13) Shake JG, Gruber PJ, Baumgartner WA, Senechal G, Meyers J, Redmond JM, Pittenger MF, Martin BJ. Mesenchymal stem cell implantation in a swine myocardial infarct model: engra- ftment and functional effects. Ann Thorac Surg 2002;73:
1919-25.
14) Devine SM, Cobbs C, Jennings M, Bartholomew A, Hoffman R. Mesenchymal stem cells distribute to a wide range of tissues following systemic infusion into nonhuman primates. Blood 2003;101:2999-3001.
15) Dominici M, Le Blanc K, Mueller I, Slaper-Cortenbach I, Marini F, Krause D, Deans R, Keating A, Prockop Dj, Horwitz E. Minimal criteria for defining multipotent mesenchymal stromal cells. The International Society for Cellular Therapy position statement. Cytotherapy 2006;8:315-7.
16) Bruder SP, Kurth AA, Shea M, Hayes WC, Jaiswal N, Kadiyala S. Bone regeneration by implantation of purified, culture- expanded human mesenchymal stem cells. J Orthop Res 1998;
16:155-62.
17) Grande DA, Southerland SS, Manji R, Pate DW, Schwartz SE, Lucas PA. Repair of articular cartilage defects using mesen- chymal stem cells. Tissue Eng 1995;1:345-53.
18) Young RG, Butler DL, Weber W, Gordon SL, Fink DJ.
Mesenchymal stem cell-based repair of rabbit Achilles tendon.
Trans Orthop Res Soc 1997;22:249.
19) Horwitz EM, Gordon PL, Koo WK, Marx JC, Neel MD, McNall RY, Muul L, Hofmann T. Isolated allogeneic bone marrow- derived mesenchymal cells engraft and stimulate growth in children with osteogenesis imperfecta: implications for cell therapy of bone. Proc Natl Acad Sci USA 2002;
99:8932-7.
20) Ortiz LA, Dutreil M, Fattman C, Pandey AC, Torres G, Go K, Phinney DG. Interleukin 1 receptor antagonist mediates the antiinflammatory and antifibrotic effect of mesenchymal stem cells during lung injury. Proc Natl Acad Sci USA 2007;104:
11002-7.
21) Berry MF, Engler AJ, Woo YJ, Pirolli TJ, Bish LT, Jayasankar V, Morine KJ, Gardner TJ, Discher DE, Sweeney HL. Mesenchymal stem cell injection after myocardial infarction improves myocardial compliance. Am J Heart Circ Physiol 2006;290:2196-203.
22) Dazzi F, Ramasamy R, Glennie S, Jones SP, Roberts I. The role of mesenchymal stem cells in haemopoiesis. Blood Rev 2006;20:161-71.
23) Brendel C, Kuklick L, Hartmann O, Kim TD, Boudriot U, Schwell D, Neubauer A. Distinct gene expression profile of human mesenchymal stem cells in comparison to skin fibro-
blasts employing cDNA microarray analysis of 9600 genes.
Gene Expr 2005;12:245-57.
24) Calvi LM, Adams GB, Weibrecht KW, Weber JM, Olson DP, Knight MC, Martin RP, Schipani E, Divieti P, Bringhurst FR, Milner LA, Kronenberg HM, Scadden DT. Osteoblastic cells regulate the haematopoietic stem cell niche. Nature 2003;425:
841-6.
25) Duncan AW, Rattis FM, DiMascio LN, Congdon KL, Pazianos G, Zhao C, Yoon K, Cook JM, Willert K, Gaiano N, Reya T. Integration of Notch and Wnt signaling in hematopoietic stem cell maintenance. Nat Immunol 2005;6:314-22.
26) Arai F, Hirao A, Ohmura M, Sato H, Matsuoka S, Takubo K, Ito K, Koh GY, Suda T. Tie2/angiopoietin-1 signaling regulates hematopoietic stem cell quiescence in the bone marrow niche.
Cell 2004;118:149-61.
27) Domenech J, Gihana E, Dayan A, Truglio D, Linassier C, Desbois I, Lamagnere JP, Colombat P, Binet C. Haemopoiesis of transplanted patients with autologous marrows assessed by long-term marrow culture. Br J Haematol 1994;88:488-96.
28) O’Flaherty E, Sparrow R, Szer J. Bone marrow stromal func- tion from patients after bone marrow transplantation. Bone Marrow Transplant 1995;15:207-12.
29) Galotto M, Berisso G, Delfino L, Podesta M, Ottaggio L, Dalloroso S, Dudour C, Ferrara GB, Abbondandolo A, Dini G, Bacigalupo A, Cancedda R, Quarto R. Stromal damage as consequence of high-dose chemo/radiotherapy in bone marrow transplant recipients. Exp Hematol 1999;27:1460-6.
30) Koç ON, Peters C, Aubourg P, Raghavan S, Dyhouse S, DeGasperi R, Kolodny EH, Yoseph YB, Gerson SL, Lazarus HM, Caplan AI, Watkins PA, Krivit W. Bone marrow-derived mesenchymal stem cells remain host-derived despite successful hematopoietic engraftment after allogeneic transplantation in patients with lysosomal and peroxisomal storage diseases. Exp Hematol 1999;27:1675-81.
31) Stute N, Fehse B, Schröder J, Arps S, Adamietz P, Held KR, Zander AR. Human mesenchymal stem cells are not of donor origin in patients with severe aplastic anemia who underwent sex-mismatched allogeneic bone marrow transplant. J Hema- tother Stem Cell Res 2002;11:977-84.
32) Noort WA, Kruisselbrink AB, in't Anker PS, Kruger M, van Bezooijen RL, de Paus RA, Heemskerk MH, Löwik CW, Falkenburg JH, Willemze R, Fibbe WE. Mesenchymal stem cells promote engraftment of human umbilical cord blood- derived CD34 (+) cells in NOD/SCID mice. Exp Hematol 2002;30:870-8.
33) Park SK, Won JH, Kim HJ, Bae SB, Kim CK, Lee KT, Lee NS, Lee YK, Jeong DC, Chung NG, Kim HS, Hong DS, Park HS. Co-transplantation of human mesenchymal stem cells promotes human CD34+ cells engraftment in a dose-dependent fashion in NOD/SCID mice. J Korean Med Sci 2007;22:
412-9.
34) Dexter TM, Allen TD, Lajtha LG. Conditions controlling the
proliferation of haemopoietic stem cells in vitro. J Cell Physiol 1977;91:335-44.
35) Sugiura K, Hisha H, Ishikawa J, Adachi Y, Taketani S, Lee S, Nagahama T, Ikehara S. Major histocompatibility complex restriction between hematopoietic stem cells and stromal cells in vitro. Stem Cells 2001;19:46-58.
36) Koç ON, Gerson SL, Cooper BW, Dyhouse SM, Haynesworth SE, Caplan AI, Lazarus HM. Rapid hematopoietic recovery after co-infusion of autologous-blood stem cells and culture- expanded marrow mesenchymal stem cells in advanced breast cancer patients receiving high-dose chemotherapy. Clin Oncol 2000;18:307-16.
37) Bartholomew A, Sturgeon C, Siatskas M, Ferrer K, McIntosh K, Patil S, Hardy W, Devine S, Ucker D, Deans R, Moseley A, Hoffman R. Mesenchymal stem cells suppress lymphocyte proliferation in vitro and prolong skin graft survival in vivo.
Exp Hematol 2002;30:42-8.
38) Krampera M, Glennie S, Dyson J, Scott D, Laylor R, Simpson E, Dazzi F. Bone marrow mesenchymal stem cells inhibit the response of naive and memory antigen-specific T cells to their cognate peptide. Blood 2003;101:3722-9.
39) Corcione A, Benvenuto F, Ferretti E, Giunti D, Cappiello V, Cazzanti F, Risso M, Gualandi F, Mancardi GL, Pistoia V, Uccelli A. Human mesenchymal stem cells modulate B cell functions. Blood 2006;107:367-72.
40) Spaggiari GM, Capobianco A, Becchetti S, Mingari MC, Moretta L. Mesenchymal stem cellnatural killer cell interac- tions: evidence that activated NK cells are capable of killing MSCs, whereas MSCs can inhibit IL-2-induced NK-cell proli- feration. Blood 2006;107:1484-90.
41) Groh ME, Maitra B, Szekely E, Koc ON. Human mesenchymal stem cells require monocyte-mediated activation to suppress alloreactive T cells. Exp Hematol 2005;33:928-34.
42) Beyth S, Borovsky Z, Mevorach D, Liebergall M, Gazit Z, Aslan H, Galun E, Rachmilewitz J. Human mesenchymal stem cells alter antigen-presenting cell maturation and induce T-cell unresponsiveness. Blood 2005;105:2214-9.
43) Aggarwal S, Pittenger MF. Human mesenchymal stem cells modulate allogeneic immune cell responses. Blood 2005;105:
1815-22.
44) Glennie S, Soeiro I, Dyson PJ, Lam EW, Dazzi F. Bone marrow mesenchymal stem cells induce division arrest anergy of activated T cells. Blood 2005;105:2821-7.
45) Dazzi F, Horwood NJ. Potential of mesenchymal stem cell therapy. Curr Opin Oncol 2007;19:650-5.
46) Fouillard L, Chapel A, Bories D, Bouchet S, Costa JM, Rouard H, Hervé P, Gourmelon P, Thierry D, Lopez M, Gorin NC. Infusion of allogeneic-related HLA mismatched mesen- chymal stem cells for the treatment of incomplete engraftment following autologous haematopoietic stem cell transplantation.
Leukemia 2007;21:568-70.
47) Ringdén O, Uzunel M, Rasmusson I, Remberger M, Sundberg
B, Lönnies H, Marschall HU, Dlugosz A, Szakos A, Hassan Z, Omazic B, Aschan J, Barkholt L, Le Blanc K. Mesen- chymal stem cells for treatment of therapy-resistant graft- versus- host disease. Transplantation 2006;81:1390-7.
48) Lazarus HM, Koc ON, Devine SM, Curtin P, Maziarz RT, Holland HK, Shpall EJ, McCarthy P, Atkinson K, Cooper BW, Gerson SL, Laughlin MJ, Loberiza FR Jr, Moseley AB, Bacigalupo A. Cotransplantation of HLA-identical sibling culture-expanded mesenchymal stem cells and hematopoietic stem cells in hematologic malignancy patients. Biol Blood Marrow Transplant 2005;11:389-98.
49) Tisato V, Naresh K, Girdlestone J, Navarrete C, Dazzi F.
Mesenchymal stem cells of cord blood origin are effective at preventing but not treating graft-versus-host disease. Leukemia 2007;21:1992-9.
50) Chung NG, Jeong DC, Park SJ, Choi BO, Cho B, Kim HK, Chun CS, JH Won, Han CW. Cotransplantation of marrow stromal cells may prevent lethal graft- versus-host disease in major histocompatibility complex mismatched murine hemato- poietic stem cell transplantation. Int J Hematol 2004;80: 370-6.
51) Blanc KL, Ringden O. Immunomodulation by mesenchymal stem cells and clinical experience. J Intern Med 2007;262:
509-25.