서 론
최근 대규모의 임상 데이터들이 축적되면서 이를 분석한 연구들 이 이루어지고 있고 특히 건강보험 청구자료를 이용한 연구들이 많 이 이루어지고 있다. 한국은 저소득층을 포함한 일부를 제외하고 대 한민국 국민의 98%가 국민건강보험에 가입되어 있으며 건강보험 청 구자료는 남한 인구의 90%에 달하는 4천 6백만 인구의 의료이용에 대한 정보를 포함하고 있다.
건강보험 청구자료는 대부분의 국민을 대상으로 한 대표성 있는 자료이며 실제 진료현장을 반영하는 자료로 역학연구 및 다양한 임
상과 관련된 연구에 이용되고 있다. 청구자료에는 주상병을 포함하 여 한 개 이상의 청구상병이 입력되며 건강보험 청구자료를 이용한 연구에서 특정 질환이나 건강상태를 가진 대상을 정의할 때 청구자 료의 상병을 이용하는 경우가 많다. 연구 대상이 되는 질병의 특성 이나 연구 디자인에 따라서 질병이나 건강상태에 대한 정의를 할 때 청구상병의 이용에 차이가 있는데 이는 질병의 특성, 또는 진료행태 에 따라 주로 주상병으로 입력되는 상병들이 있는 반면에 또는 청구 상병으로 입력은 되지만 주로 주상병으로 입력되지 않는 상병들도 있기 때문이다. 연구마다 청구상병의 주상병만을 사용하는 경우, 주상병, 부상병을 사용하는 경우,1,2) 일부 상병,3,4) 그리고 전체 상병
Original Article
건강보험 청구상병의 상대적, 절대적 순위 분석
김진희, 윤재문*, 정의헌, 강미소
서울대학교병원 가정의학과, 서울대학교병원 건강검진센터
Relative and Absolute Rankings of Diagnosis Codes in Claims Data
Jin Hee Kim, Jae Moon Yun*, Eui Heon Chung, Mi So Kang
Department of Family Medicine & Health Promotion Center, Seoul National University Hospital, Seoul, Korea
Background: In recent times, much research has used claims data and diagnosis codes in claims data to define medical conditions or diseases that are the objects of studies. In this study, we analyzed relative and absolute rankings of diagnosis codes and principal diagnosis code selections in claims data.
Methods: We used claims data from the Health Insurance Review and Assessment Service-National Patient Sample (HIRA-NPS) for the year 2011. We calculated relative and absolute ranking of diagnosis codes representing locations of each diagnosis code on the diagnosis code list. We also calculated the priority index as principal diagnosis to investigate the principal diagnosis code selections. The analysis was conducted according to healthcare facilities, and inpatient and outpatient circumstances.
Results: We presented high-ranked and low-ranked diagnosis codes according to healthcare facilities, and inpatient and outpatient circumstances.
There were differences among diagnosis codes by disease nature, severity, and diagnosis code categories. There were also differences among the healthcare facilities and between inpatient and outpatient circumstances that reflected differences in patient groups and medical practice in clinical settings.
Conclusion: To increase the sensitivity and specificity of medical conditions or diseases that are the objects of studies, it is necessary to use proper diagnosis codes. Our results can be applied to select proper diagnosis codes for studies using claims data.
Keywords: Diagnosis Codes; Principal Diagnosis; Claims Data; National Patient Samples
http://dx.doi.org/10.21215/kjfp.2016.6.4.331eISSN 2233-9116
Korean J Fam Pract. 2016;6(4):331-338
KJFP
Korean Journal of Family PracticeReceived March 2, 2016 Revised May 5, 2016 Accepted June 1, 2016 Corresponding author Jae Moon Yun
Tel: +82-2-2072-4012, Fax: +82-2-766-3276 E-mail: [email protected]
Copyright © 2016 The Korean Academy of Family Medicine
This is an open-access article distributed under the terms of the Creative Commons At- tribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Jin Hee Kim, et al. Rankings of Diagnosis Codes in Claims Data
Korean Journal of Family Practice
KJFP
을 연구하는 경우로 다양하며 일부 연구에서는 어떤 상병을 사용하 여 조작적 정의를 하였는지 명확히 언급이 되지 않는 경우도 많아 이 런 경우에는 연구의 재현성이나 신뢰도를 낮출 수 있다.5-10) 따라서 청구자료의 상병을 이용한 연구들을 설계할 때 어떤 상병을 이용할 지를 결정하기 위해서는 청구상병들이 청구자료에 등록되는 양상 을 분석해 볼 필요가 있다.
본 연구에서 저자들은 건강보험 청구자료에서 요양기관의 종별, 입원, 외래 환경에 따라 각 청구상병이 청구상병목록 중에서 어느 위치에 위치하며 또한 주상병으로 입력되는 상대적 확률이 높은 상 병들과 그렇지 않은 상병들을 분석하였다.
방 법
1. 연구자료
본 연구는 건강보험심사평가원 국가환자 표본자료(Health Insur- ance Review and Assessment Service-National Patient Sample, HIRA- NPS) 2011년 자료를 이용하였다. HIRA-NPS는 1년간 의료이용을 한 모든 환자들을 대상으로 하여 성별, 연령구간으로 층화 계통 추출한 표본자료로 전체인구의 3%에 해당하는 약 1,400,000명의 환자들을 포 함한다.11) 저자들은 청구자료를 요양기관 종별에 따라 상급종합병원 과 종합병원(general hospitals), 병원(hospitals), 의원(clinics), 세 군으로 나누었으며 입원(inpatient)과 외래(outpatient)로 나누어 분석하였다.
2. 연구방법
1) 청구상병(diagnosis code)
HIRA-NPS-2011의 청구상병은 한국표준질병사인분류 6차(Kore- an Standard Classification of Diseases, KCD-6)에 따라 입력되어 있으 며 저자들은 KCD-6에 따라 입력된 청구상병의 앞 세 자리만 이용하 여 2,093개의 소분류 질병코드를 이용하여 분석하였다. 청구건수가 100건 이상이 되는 상병들을 대상으로 상병코드목록 상에서의 상 대적, 절대적 입력 위치와 주상병으로 입력될 상대적 확률에 대해 상위, 하위에 위치하는 청구상병들을 분석하였다.
2) 청구상병의 상대적 상병 순위(relative ranking of diagnosis code, rankp) 청구자료의 상병테이블에는 입력된 청구상병들과 함께 각 청구 상병의 일련번호가 입력되어 있으며 N개의 청구상병이 입력되어 있 는 경우 일련번호는 1에서부터 N까지이다. 일련번호가 1인 경우가 주 상병에 해당한다. 청구상병목록에서 청구상병의 상대적 상병 순위 를 정의하기 위하여 청구상병이 상병목록의 앞에 있을수록 0에 가 깝고 뒤에 있을수록 1에 가까운 것으로 정의하였고 각 청구상병이 0 과 1사이에서 어느 위치에 위치하는지를 나타내기 위하여 청구상병 의 상대적 상병 순위(relative ranking of diagnosis code, rankp)를 다음 과 같이 정의하였다.
rankp= rank-0.5 N
rank: 상병테이블의 각 청구상병의 일련번호, 절대적 상병 순위 (absolute ranking of diagnosis code)
N: 상병테이블의 청구상병의 개수
예를 들어 청구상병이 주상병 하나밖에 없는 경우, 위와 같이 계 산한 상대적 상병 순위는 rankp=0.5로 0과 1사이에 한가운데에 위치 한다고 할 수 있다.
3) 주상병 우선도(priority index as principal diagnosis, PIPD)
한 개의 청구건에서 청구상병이 N개인 경우 각 청구상병이 주상 병명이 될 확률이 동일하다고 가정하였을 때 하나의 청구상병이 주 상병명이 될 확률은 1/N이다. 전체 청구건에 대하여 이를 계산하여 평균을 내었고 이를 청구상병의 주상병 기대값(expected value as principal diagnosis, EVPD)이라고 정의하였다. 또한 전체 청구건에서 각 청구상병들이 실제로 주상병명으로 입력된 분율을 계산하였고 이를 청구상병의 주상병 분율(principal diagnosis rate, PDR)이라고 정의하였다. 각 청구상병들에 대해 주상병 분율에서 주상병 기대값 을 뺀 값을 주상병 우선도(priority index as principal diagnosis [PIPD]=PDR-EVPD)라고 정의하였으며 주상병 우선도 값이 클수록 상대적으로 주상병이 될 확률이 크다고 할 수 있다.
모든 분석은 STATA ver. 14.0 (Stata Co., College Station, TX, USA)을 이용하여 시행하였다.
Table 1. Baseline characteristics of claims data
Medical institution Number of claim Mean of number of diagnosis codes per claim
Inpatient Outpatient Subtotal Inpatient Outpatient Subtotal
General hospital 146,882 (6.6%) 2,064,614 (93.4%) 2,211,496 5.24 2.71 2.88
Hospital 92,968 (8.3%) 1,027,758 (91.7%) 1,120,726 4.76 2.69 2.86
Clinic 50,850 (0.3%) 15,669,623 (99.7%) 15,720,473 2.61 2.61 2.61
Subtotal 290,700 (1.5%) 18,761,995 (98.5%) 19,052,695 4.63 2.63 2.66
김진희 외. 건강보험 청구상병의 순위 분석 Korean Journal of Family Practice
KJFP
결 과
1. 청구자료의 자료 기초 특성
요양기관 종별, 입원, 외래별 청구명세서 건수, 명세서 1건당 평균 청구상병 개수는 Table 1과 같다. 총 명세서 건수는 19,052,695건이며 그 중 290,700건(1.5%)은 입원, 18,761,995건(98.5%)이 외래에서 발행되 었다. 명세서 1건당 평균 청구상병은 전체 2.66개로 입원의 경우 4.63 개, 외래의 경우 2.63개였다.
2. 청구상병의 상대적 상병 순위(relative ranking of diagnosis code, rank
p)
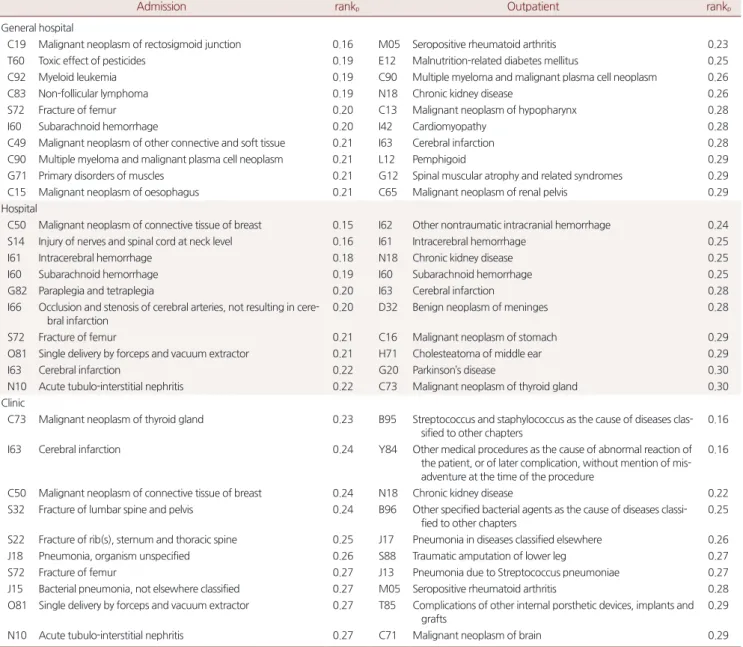
요양기관 종별, 입원, 외래별로 상대적 상병 순위(rankp)가 높은 상 병들은 다르게 나타났는데, 상급종합병원과 종합병원 입원의 경우 직장구불결장암(C19)이 rankp 0.16으로 가장 순위가 높았으며 외래 의 경우 류마티스관절염(M05)이 rankp 0.23으로 가장 높았다. 병원 입원은 유방암(C50; rankp=0.15), 병원 외래는 두개내 출혈(I62;
rankp=0.24), 의원 입원은 갑상선암(C73; rankp=0.23), 의원 외래는 연 쇄구균 및 포도구균(B95; rankp=0.16)이 가장 순위가 높았다. 반면 상 급종합병원과 종합병원 입원에서 당뇨(R81)가 rankp 0.79로 가장 순
Table 2. High ranked diagnosis codes
Admission rankp Outpatient rankp
General hospital
C19 Malignant neoplasm of rectosigmoid junction 0.16 M05 Seropositive rheumatoid arthritis 0.23
T60 Toxic effect of pesticides 0.19 E12 Malnutrition-related diabetes mellitus 0.25
C92 Myeloid leukemia 0.19 C90 Multiple myeloma and malignant plasma cell neoplasm 0.26
C83 Non-follicular lymphoma 0.19 N18 Chronic kidney disease 0.26
S72 Fracture of femur 0.20 C13 Malignant neoplasm of hypopharynx 0.28
I60 Subarachnoid hemorrhage 0.20 I42 Cardiomyopathy 0.28
C49 Malignant neoplasm of other connective and soft tissue 0.21 I63 Cerebral infarction 0.28
C90 Multiple myeloma and malignant plasma cell neoplasm 0.21 L12 Pemphigoid 0.29
G71 Primary disorders of muscles 0.21 G12 Spinal muscular atrophy and related syndromes 0.29
C15 Malignant neoplasm of oesophagus 0.21 C65 Malignant neoplasm of renal pelvis 0.29
Hospital
C50 Malignant neoplasm of connective tissue of breast 0.15 I62 Other nontraumatic intracranial hemorrhage 0.24
S14 Injury of nerves and spinal cord at neck level 0.16 I61 Intracerebral hemorrhage 0.25
I61 Intracerebral hemorrhage 0.18 N18 Chronic kidney disease 0.25
I60 Subarachnoid hemorrhage 0.19 I60 Subarachnoid hemorrhage 0.25
G82 Paraplegia and tetraplegia 0.20 I63 Cerebral infarction 0.28
I66 Occlusion and stenosis of cerebral arteries, not resulting in cere- bral infarction
0.20 D32 Benign neoplasm of meninges 0.28
S72 Fracture of femur 0.21 C16 Malignant neoplasm of stomach 0.29
O81 Single delivery by forceps and vacuum extractor 0.21 H71 Cholesteatoma of middle ear 0.29
I63 Cerebral infarction 0.22 G20 Parkinson’s disease 0.30
N10 Acute tubulo-interstitial nephritis 0.22 C73 Malignant neoplasm of thyroid gland 0.30
Clinic
C73 Malignant neoplasm of thyroid gland 0.23 B95 Streptococcus and staphylococcus as the cause of diseases clas- sified to other chapters
0.16
I63 Cerebral infarction 0.24 Y84 Other medical procedures as the cause of abnormal reaction of the patient, or of later complication, without mention of mis- adventure at the time of the procedure
0.16
C50 Malignant neoplasm of connective tissue of breast 0.24 N18 Chronic kidney disease 0.22
S32 Fracture of lumbar spine and pelvis 0.24 B96 Other specified bacterial agents as the cause of diseases classi- fied to other chapters
0.25
S22 Fracture of rib(s), sternum and thoracic spine 0.25 J17 Pneumonia in diseases classified elsewhere 0.26
J18 Pneumonia, organism unspecified 0.26 S88 Traumatic amputation of lower leg 0.27
S72 Fracture of femur 0.27 J13 Pneumonia due to Streptococcus pneumoniae 0.27
J15 Bacterial pneumonia, not elsewhere classified 0.27 M05 Seropositive rheumatoid arthritis 0.28
O81 Single delivery by forceps and vacuum extractor 0.27 T85 Complications of other internal porsthetic devices, implants and grafts
0.29
N10 Acute tubulo-interstitial nephritis 0.27 C71 Malignant neoplasm of brain 0.29
rankp, relative ranking of diagnosis code.
Jin Hee Kim, et al. Rankings of Diagnosis Codes in Claims Data
Korean Journal of Family Practice
KJFP
위가 낮았으며 외래는 치료 시 유해작용을 나타내는 진통제, 해열제 및 항염증제(Y45)가 rankp 0.77로 가장 낮았다. 병원 입원은 암 이외의 병태에 대한 치료 후 추적검사(Z09; rankp=0.84), 병원 외래는 미끄러 짐, 걸림 및 헛디딤에 의한 넘어짐(W01; rankp=0.82), 의원 입원은 권 태 및 피로(R53; rankp=0.76), 의원 외래는 재활처치와 관련된 의료를 위하여 보건서비스와 접하고 있는 사람(Z50; rankp=0.86)이 가장 순 위가 낮았다. 청구상병목록에서 주로 상위, 하위에 위치하는 상위 10 개의 상병들은 Tables 2, 3과 같다.
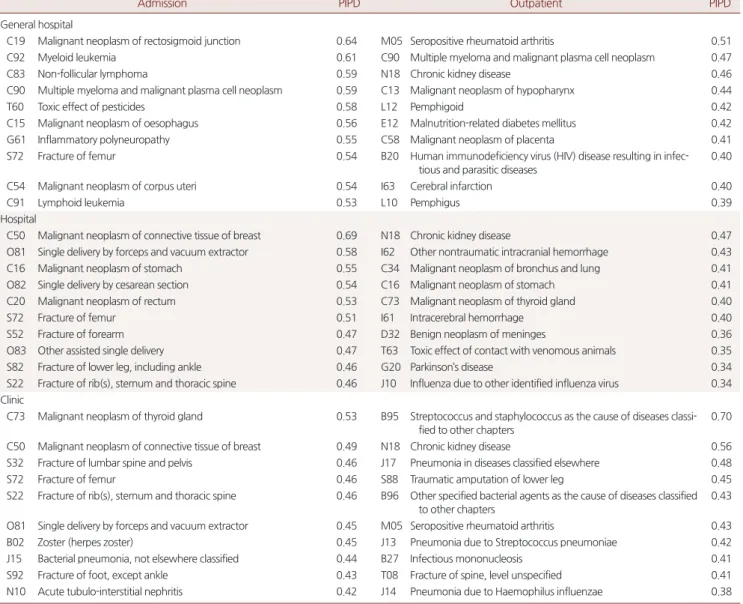
3. 청구상병의 주상병 우선도(priority index as principal diagnosis, PIPD)
주상병 우선도가 높아 주상병으로 입력될 가능성이 높은 상병은 상급종합병원과 종합병원의 경우 입원은 직장구불결장암(C19;
PIPD=0.64), 외래는 류마티스관절염(M05; PIPD=0.51), 병원 입원은 유방암(C50; PIPD=0.69), 병원 외래는 만성 신장질환(N18;
PIPD=0.47), 의원 입원은 갑상선암(C73; PIPD=0.53), 의원 외래는 연 쇄구균 및 포도구균(B95; PIPD=0.70)으로 나타났다. 주상병 우선도 가 낮아 주상병으로 입력될 가능성이 낮은 상병은 상급종합병원과 Table 3. Low ranked diagnosis codes
Admission rankp Outpatient rankp
General hospital
R81 Glycosuria 0.79 Y45 Analgesics, antipyretics and anti-inflammatory drugs causing ad-
verse effects in therapeutic use
0.77
E07 Other disorders of thyroid 0.79 E63 Other nutritional deficiencies 0.75
C26 Malignant neoplasm of other and ill-defined digestive organs 0.79 R81 Glycosuria 0.74
R82 Other abnormal findings in urine 0.77 E46 Unspecified protein-energy malnutrition 0.73
Z03 Medical observation and evaluation for suspected diseases and conditions
0.75 R12 Heartburn 0.72
A53 Other and unspecified syphilis 0.75 Z72 Problems related to lifestyle 0.71
R73 Elevated blood glucose level 0.75 R14 Flatulence and related conditions 0.71
R74 Abnormal serum enzyme levels 0.74 E58 Dietary calcium deficiency 0.71
R94 Abnormal results of function studies 0.73 A07 Other protozoal intestinal diseases 0.71
L22 Diaper[napkin] dermatitis 0.72 E35 Disorders of endocrine glands in diseases classified elsewhere 0.71 Hospital
Z09 Follow-up examination after treatment for conditions other than malignant neoplasm
0.84 W01 Fall on same level from slipping, tripping and stumbling 0.82
R81 Glycosuria 0.81 R12 Heartburn 0.76
E07 Other disorders of thyroid 0.78 R14 Flatulence and related conditions 0.76
L24 Irritant contact dermatitis 0.77 Y88 Sequelae with surgical and medical care as external cause 0.74
E06 Thyroiditis 0.77 R73 Elevated blood glucose level 0.74
R41 Other symptoms and signs involving cognitive functions and awareness
0.77 H57 Other disorders of eye and adnexa 0.74
Z03 Medical observation and evaluation for suspected diseases and conditions
0.76 R81 Glycosuria 0.73
R12 Heartburn 0.76 K30 Dyspepsia 0.73
R73 Elevated blood glucose level 0.76 R79 Other abnormal findings of blood chemistry 0.72
A53 Other and unspecified syphilis 0.75 Z04 Examination and observation for other reasons 0.71
Clinic
R53 Malaise and fatigue 0.76 Z50 Care involving use of rehabilitation procedures 0.86
L30 Other dermatitis 0.76 Z27 Need for immunization against combinations of infectious dis-
eases
0.84
E07 Other disorders of thyroid 0.75 T50 Poisoning by diuretics and other and unspecified drugs, medica- ments and biological substances
0.83
K30 Dyspepsia 0.73 R13 Dysphagia 0.78
F42 Obsessive-compulsive disorder 0.73 Y88 Sequelae with surgical and medical care as external cause 0.76
R05 Cough 0.73 B47 Mycetoma 0.74
L50 Urticaria 0.72 R12 Heartburn 0.74
R30 Pain associated with micturition 0.72 F54 Psychological and behavioral factors associated with disorders or diseases classified elsewhere
0.73
R12 Heartburn 0.72 R77 Other abnormalities of plasma proteins 0.73
L29 Pruritus 0.71 K30 Dyspepsia 0.72
rankp, relative ranking of diagnosis code.
김진희 외. 건강보험 청구상병의 순위 분석 Korean Journal of Family Practice
KJFP
종합병원 입원에서 처치 후의 내분비 및 대사장애(E89; PIPD=-0.25), 외래에서 포함된 신체표면의 정도에 따라 분류된 화상(T31; PIPD=
-0.34), 병원 입원은 태위장애의 산모관리(O32; PIPD=-0.35), 병원 외 래는 암의 치료 후 추적검사(Z08; PIPD=-0.38), 의원 입원은 강박장 애(F42; PIPD=-0.46), 의원 외래는 혈액 및 조혈기관의 기타 장애(D77;
PIPD=-0.43)였다. 청구상병목록에서 상대적으로 주상병으로 입력 될 가능성이 높은 상병, 낮은 상병 10개는 Tables 4, 5와 같다.
요양기관 종별, 입원, 외래별 모든 분석결과는 Supplementary ma- terials에 실었다.
고 찰
본 연구결과에서 주상병 우선도(PIPD)가 높다는 것은 주상병으 로 채택될 확률이 동일하다고 가정하였을 때의 기대값에 비해서 실 제로 더 많이 주상병으로 채택되었다는 것을 의미하며 단순히 주상 병으로 많이 입력되는 청구상병으로 오해하지 말아야 한다. 각 청구 상병이 청구건에서 주상병으로 입력되는 분율(PDR)만으로 비교하 지 않고 주상병 기대값(EVPD)과의 차이로 비교를 한 이유는 질병마 다 동반질환이나 함께 입력되는 청구상병의 개수가 다르기 때문이 다. 안과, 이비인후과, 피부과 질환 등 주상병 분율이 높아도 함께 입 력되는 상병의 개수가 적어 주상병 기대값도 함께 높아 주상병 우선 도가 낮아지는 경우들이 있다. 예로 의원 외래의 분석결과에서 백반
Table 4. High ranked principal diagnosis codes
Admission PIPD Outpatient PIPD
General hospital
C19 Malignant neoplasm of rectosigmoid junction 0.64 M05 Seropositive rheumatoid arthritis 0.51
C92 Myeloid leukemia 0.61 C90 Multiple myeloma and malignant plasma cell neoplasm 0.47
C83 Non-follicular lymphoma 0.59 N18 Chronic kidney disease 0.46
C90 Multiple myeloma and malignant plasma cell neoplasm 0.59 C13 Malignant neoplasm of hypopharynx 0.44
T60 Toxic effect of pesticides 0.58 L12 Pemphigoid 0.42
C15 Malignant neoplasm of oesophagus 0.56 E12 Malnutrition-related diabetes mellitus 0.42
G61 Inflammatory polyneuropathy 0.55 C58 Malignant neoplasm of placenta 0.41
S72 Fracture of femur 0.54 B20 Human immunodeficiency virus (HIV) disease resulting in infec-
tious and parasitic diseases
0.40
C54 Malignant neoplasm of corpus uteri 0.54 I63 Cerebral infarction 0.40
C91 Lymphoid leukemia 0.53 L10 Pemphigus 0.39
Hospital
C50 Malignant neoplasm of connective tissue of breast 0.69 N18 Chronic kidney disease 0.47
O81 Single delivery by forceps and vacuum extractor 0.58 I62 Other nontraumatic intracranial hemorrhage 0.43
C16 Malignant neoplasm of stomach 0.55 C34 Malignant neoplasm of bronchus and lung 0.41
O82 Single delivery by cesarean section 0.54 C16 Malignant neoplasm of stomach 0.41
C20 Malignant neoplasm of rectum 0.53 C73 Malignant neoplasm of thyroid gland 0.40
S72 Fracture of femur 0.51 I61 Intracerebral hemorrhage 0.40
S52 Fracture of forearm 0.47 D32 Benign neoplasm of meninges 0.36
O83 Other assisted single delivery 0.47 T63 Toxic effect of contact with venomous animals 0.35
S82 Fracture of lower leg, including ankle 0.46 G20 Parkinson’s disease 0.34
S22 Fracture of rib(s), sternum and thoracic spine 0.46 J10 Influenza due to other identified influenza virus 0.34 Clinic
C73 Malignant neoplasm of thyroid gland 0.53 B95 Streptococcus and staphylococcus as the cause of diseases classi- fied to other chapters
0.70
C50 Malignant neoplasm of connective tissue of breast 0.49 N18 Chronic kidney disease 0.56
S32 Fracture of lumbar spine and pelvis 0.46 J17 Pneumonia in diseases classified elsewhere 0.48
S72 Fracture of femur 0.46 S88 Traumatic amputation of lower leg 0.45
S22 Fracture of rib(s), sternum and thoracic spine 0.46 B96 Other specified bacterial agents as the cause of diseases classified to other chapters
0.43
O81 Single delivery by forceps and vacuum extractor 0.45 M05 Seropositive rheumatoid arthritis 0.43
B02 Zoster (herpes zoster) 0.45 J13 Pneumonia due to Streptococcus pneumoniae 0.42
J15 Bacterial pneumonia, not elsewhere classified 0.44 B27 Infectious mononucleosis 0.41
S92 Fracture of foot, except ankle 0.43 T08 Fracture of spine, level unspecified 0.41
N10 Acute tubulo-interstitial nephritis 0.42 J14 Pneumonia due to Haemophilus influenzae 0.38
PIPD, priority index as principal diagnosis.
Jin Hee Kim, et al. Rankings of Diagnosis Codes in Claims Data
Korean Journal of Family Practice
KJFP
증(L80)의 주상병 분율은 0.94로 높지만 주상병 기대값도 0.82로 높 아 주상병 우선도는 0.12로 낮아진다. 반면에 동반질환이나 합병증 등이 많아 함께 입력된 청구상병들이 많은 폐렴(J17)의 경우 주상병 분율은 0.76으로 백반증보다 낮지만 주상병 기대값도 0.28로 낮아 주상병 우선도는 0.48로 백반증보다 더 높아진다. 즉 주상병 우선도 가 높다는 것은 여러 개의 입력된 청구상병들 중에서 상대적으로 주상병으로 채택될 확률이 높다는 의미이다.
의무기록을 작성하거나 청구상병을 입력할 때 입원이나 치료를
받게 되는 주된 원인을 주상병으로 선정하며 증상이나 징후, 병태 등은 진단된 질병명이 있는 경우 주상병으로 선정하지 않는 것이 원 칙이다.12) 본 연구결과도 이 원칙에 따라 나타났는데 악성 신생물이 나 뇌졸중, 골절, 폐렴 등과 같이 중증도가 높고 입원이나 외래 방문 의 원인이 되는 질환에 대한 상병들이 청구상병목록 상에서 주로 상위에 위치하고 상대적으로 주상병으로 입력될 확률이 높았다. 반 면에 입원과 외래 방문의 이유가 되는 질환과 동반될 수 있는 증상 과 징후, 검사소견의 이상, 치료과정에서 발생할 수 있는 합병증, 보 Table 5. Low ranked principal diagnosis codes
Admission PIPD Outpatient PIPD
General hospital
E89 Postprocedural endocrine and metabolic disorders, NEC -0.25 T31 Burns classified according to extent of body surface involved -0.34 Z90 Acquired absence of organs, NEC -0.23 P91 Other disturbances of cerebral status of newborn -0.33 O68 Labor and delivery complicated by fetal stress (distress) -0.22 Z51 Persons encountering health services for other medical care -0.32 O99 Other materal diseases classifiable elsewhere but complicating
pregnancy, childbirth and the puerperium
-0.21 Z48 Persons encountering health services for other surgical follow- up care
-0.32
C77 Secondary and unspecified malignant neoplasm of lymph nodes -0.20 Z98 Other postsurgical states -0.30 Z35 Supervision of high-risk pregnancy -0.20 E35 Disorders of endocrine glands in diseases classified elsewhere -0.30
Z96 Persence of other functional implants -0.20 T79 Certain early complications of trauma -0.28
N72 Inflammatory disease of cervix uteri -0.20 E58 Dietary calcium deficiency -0.27
Z34 Supervision of normal pregnancy -0.19 E89 Postprocedural endocrine and metabolic disorders, NEC -0.27
O42 Premature rupture of membranes -0.19 K10 Other diseases of jaws -0.27
Hospital
O32 Maternal care for known or suspected malpresentation of fetus -0.35 Z08 Follow-up examination after treatment for malignant neoplasm -0.38 O33 Maternal care for known or suspected disproportion -0.32 W45 Foreign body or object entering through skin -0.37
H52 Disorders of refraction and accommodation -0.30 W54 Bitten or struck by dog -0.36
O34 Maternal care for known or suspected abnormality of pelvic or- gans
-0.30 Z23 Need for immunization against single bacterial diseases -0.33
Z35 Supervision of high-risk pregnancy -0.30 X23 Contact with hornets, wasps and bees -0.33
O24 Diabetes mellitus in pregnancy -0.26 T31 Burns classified according to extent of body surface involved -0.31 O42 Premature rupture of membranes -0.26 Y45 Analgesics, antipyretics and anti-inflammatory drugs causing
adverse effects in therapeutic use
-0.31
O70 Perineal laceration during delivery -0.25 Z36 Antenatal screening -0.29
O68 Labor and delivery complicated by fetal stress (distress) -0.24 B98 Other sprcified infectious agents as the cause of disease classi- fied to other chapters
-0.29
O99 Other materal diseases classifiable elsewhere but complicating pregnancy, childbirth and the puerperium
-0.24 Z51 Persons encountering health services for other medical care -0.29
Clinic
F42 Obsessive-compulsive disorder -0.46 D77 Other disorders of blood and blood-forming organs in diseases classified elsewhere
-0.43
O70 Perineal laceration during delivery -0.33 M36 Systemic disorders of connective tissue in diseases classified elsewhere
-0.34
O71 Other obstetric trauma -0.33 Z55 Problems related to education and literacy -0.32
Z35 Supervision of high-risk pregnancy -0.31 R12 Heartburn -0.31
Z96 Persence of other functional implants -0.31 O12 Gestational [pregnancy-induced] edema and proteinuria with- out hypertension
-0.31
O72 Postpartum hemorrhage -0.28 G60 Hereditary and idiopathic neuropathy -0.31
H40 Glaucoma -0.27 K30 Dyspepsia -0.30
H16 Keratitis -0.27 Q04 Other congenital malformations of brain -0.29
F51 Nonorganic sleep disorders -0.27 Y88 Sequelae with surgical and medical care as external cause -0.29 Z98 Other postsurgical states -0.26 F54 Psychological and behavioral factors associated with disorders
or diseases classified elsewhere
-0.29
PIPD, priority index as principal diagnosis; NEC, not elsewhere classified.
김진희 외. 건강보험 청구상병의 순위 분석 Korean Journal of Family Practice
KJFP
험청구를 위한 상병코드들은 주로 하위에 위치하고 상대적으로 주 상병명으로 입력될 확률이 낮았다.
분석결과는 요양기관 종별에 따라 다소 차이가 있었다. 의원은 주 로 외래환자를, 병원은 주로 입원환자를 대상으로 하며 상급종합병 원은 중증질환을 대상으로 하도록 하고 있다.13) 본 연구결과에서 종 합병원의 경우 혈액암 및 희귀암을 포함한 다양한 암, 병원은 분만과 다양한 부위의 골절, 의원은 세균 및 바이러스 감염, 폐렴 등 감염성 질환에 대한 상병이 다른 종류의 요양기관과 비교하여 상위에 위치 하고 상대적으로 주상병이 될 확률이 높았다. 또한 입원과 외래를 나누어 분석하였을 때 입원의 경우 악성 신생물, 분만, 골절, 폐렴 등 수술이 필요하거나 급성기 치료가 중요한 질환명이 상위에 위치하 고 상대적으로 주상병명으로 입력될 확률이 높았으며 외래의 경우 당뇨, 만성 신장질환, 류마티스관절염과 같은 만성 질환들, 뇌졸중과 같이 급성기를 지난 후에 외래를 통해 관리가 가능한 질환들이 상 위에 위치하며 상대적으로 주상병이 될 확률이 높았다. 요양기관 종 별, 입원, 외래 환경에 따라 상위에 위치하는 상병과 상대적으로 주 상병으로 입력될 확률이 높은 청구상병들이 다른 것은 진료 환경에 따른 환자군과 진료패턴의 차이를 반영한다.
청구자료를 이용한 연구에서 연구 대상이 되는 건강상태, 또는 질 병을 정의 할 때 적절한 청구상병을 이용하는 것은 실제 질병상태를 얼마나 정확히 반영하는지, 즉 민감도, 특이도와 연관되어 있다. 질 병에 따라 청구자료의 청구상병을 이용하였을 때의 민감도와 특이 도에는 차이가 있지만14,15) 많은 청구상병을 이용할수록 민감도는 상 승하나 특이도가 떨어지며 주상병만 사용하는 경우 주상병 우선도 가 민감도와 연관되어 있다고 볼 수 있다. 주상병 우선도가 높은 질 병으로 대상으로 연구를 할 때는 주상병명만 이용하여도 민감도가 많이 떨어지지 않지만 당뇨, 고지혈증과 같이 동반질환이 많고 주상 병 우선도가 낮은 질병의 경우 주상병명만 이용하거나 적은 숫자의 상병코드만 사용하면 민감도가 낮아진다. 따라서 연구 대상의 민감 도와 특이도를 높이기 위해서는 연구대상에 따라 적절한 범위의 청 구상병을 정하는 것이 필요하고 추가로 진료행위나 투약내역 등을 이용한 조작적 정의의 보완이 필요하다.
건강보험 청구상병은 청구를 목적으로 입력되는 것이기 때문에 청구상병과 의무기록의 불일치도가 있을 수 있으며16,17) 주상병 입력 원칙에 따라 주상병 선정이 되지 않았을 가능성이 있다. 본 연구에 서는 의무기록 검토를 하지 않았기 때문에 상병코드 입력과 주상병 선정이 적절하게 되었는지를 판단할 수 없었고 어느 정도의 상병코 드를 이용하는 것이 적절한지에 대해서는 결정을 할 수 없었으나 연 구 대상이 되는 질병에 따라 본 연구의 결과를 참고하여 연구에 이 용하기에 적절한 상병코드의 개수를 유추해 볼 수 있을 것이다. 본
연구와는 다른 방법이지만 연구의 신뢰도를 높이기 위해서 연구에 적절한 상병코드의 개수를 결정하고 몇 번째까지의 청구상병을 사 용하였을 때의 유병률이 해당 집단의 알려진 유병률과 가장 유사한 지를 비교해볼 수 있겠다. 또한 연구에서 몇 번째까지의 청구상병을 사용하였는지 언급을 하는 것이 연구의 재현성을 향상시키는 데 도 움이 되겠다.
본 연구는 요양기관 종별, 외래, 입원 별로 청구상병 입력의 우선순 위와 주상병명으로 입력되는 상병을 분석한 탐색적 연구로 청구자료 의 청구상병을 이용하는 연구설계에 참고할 수 있는 결과를 제공한다.
요 약
연구배경:
최근 건강보험 청구자료를 이용한 연구들이 많이 이루어 지고 있으며 특정 질환이나 건강상태를 정의할 때 청구자료에 입력 된 청구상병을 이용하는 경우가 많다. 본 연구는 요양기관의 종별, 입원, 외래 환경에 따른 각 청구상병의 상대적, 절대적 순위와 주상 병 선정에 대해 분석하여 적절한 청구상병 이용을 위한 탐색적 연 구를 수행하였다.방법:
건강보험심사평가원 국가환자 표본자료(Health Insurance Re- view and Assessment Service–National Patient Sample, HIRA-NPS) 2011 년 자료를 이용하여 한국표준질병사인분류 6차((Korean Standard Classification of Diseases, KCD-6)에 따라 입력되어 있는 청구상병의 소분류 중 청구건수가 100건 이상인 청구상병들을 대상으로 상병 코드목록 상에서의 입력 위치를 상대적, 절대적 상병 순위로, 주상 병으로 입력될 상대적 확률을 주상병 우선도로 정의하여 계산하였 다. 또한 요양기관 종별에 따라 상급종합병원과 종합병원, 병원, 의 원, 세 군으로 나누었으며 입원과 외래로 나누어 분석하였다.결과:
요양기관 종별, 입원, 외래별 청구상병의 상대적 상병 순위, 주상 병 우선도의 상위, 하위에 위치하는 청구상병들에 대해서 제시하였다.청구상병 카테고리에 따라서, 그리고 특정질환을 나타내는 청구상 병의 경우 질환의 특성과 중증도에 따라서 청구상병목록 상에서의 순위와 주상병명 채택의 차이가 있었다. 또한 요양기관 종별, 입원, 외래 환경에 따라서도 결과의 차이가 나타났고 이는 진료 환경에 따 른 환자군과 진료패턴의 차이를 반영한다.
결론:
연구 대상이 되는 건강상태, 또는 질병의 민감도와 특이도를 높이기 위해 연구대상에 따라 적절한 청구상병을 정하고 진료행위 나 투약내역 등을 이용한 조작적 정의의 보완이 필요하며 적절한 범 위의 청구상병을 정할 때 본 연구의 결과를 참고할 수 있을 것으로 생각한다.Jin Hee Kim, et al. Rankings of Diagnosis Codes in Claims Data
Korean Journal of Family Practice
KJFP
중심단어:
청구상병; 주상병; 청구자료; 국가환자 표본자료REFERENCES
1. Oh H, Boo S. Burns in South Korea: an analysis of nationwide data from the health insurance review and assessment service. Burns 2016; 42: 675-81.
2. Kim J, Lee JH, Kim Y, Kim K, Oh YM, Yoo KH, et al. Association between chronic obstructive pulmonary disease and gastroesophageal reflux disease:
a national cross-sectional cohort study. BMC Pulm Med 2013; 13: 51.
3. Suh HS, Kang HY, Kim J, Shin E. Effect of health insurance type on health care utilization in patients with hypertension: a national health insurance database study in Korea. BMC Health Serv Res 2014; 14: 570.
4. Jung HK, Kim YH, Park JY, Jang BH, Park SY, Nam MH, et al. Estimating the burden of irritable bowel syndrome: analysis of a nationwide Korean data- base. J Neurogastroenterol Motil 2014; 20: 242-52.
5. Choi HJ, Shin CS, Ha YC, Jang S, Jang S, Park C, et al. Burden of osteoporosis in adults in Korea: a national health insurance database study. J Bone Miner Metab 2012; 30: 54-8.
6. Choi HJ, Park C, Lee YK, Ha YC, Jang S, Shin CS. Risk of fractures in subjects with antihypertensive medications: a nationwide claim study. Int J Cardiol 2015; 184: 62-7.
7. Lee CH, Kim K, Hyun MK, Jang EJ, Lee NR, Yim JJ. Use of inhaled cortico- steroids and the risk of tuberculosis. Thorax 2013; 68: 1105-13.
8. Yun JM, Shin DW, Hwang SS, Cho J, Nam YS, Kim JH, et al. Effect of public disclosure on antibiotic prescription rate for upper respiratory tract infec- tions. JAMA Intern Med 2015; 175: 445-7.
9. Ahn E, Shin DW, Yang HK, Yun JM, Chun SH, Suh B, et al. Treatment gap in
the national health-screening program in Korea: claim-based follow-up of statin use for sustained hypercholesterolemia. J Korean Med Sci 2015;30:1266-72.
10. Lee CH, Hyun MK, Jang EJ, Lee NR, Kim K, Yim JJ. Inhaled corticosteroid use and risks of lung cancer and laryngeal cancer. Respir Med 2013; 107:
1222-33.
11. Kim L, Kim JA, Kim S. A guide for the utilization of health insurance review and assessment service national patient samples. Epidemiol Health 2014;
36: e2014008.
12. National Center for Health Statistics. ICD-10-CM official guidelines for coding and reporting. Hyattsville, MD: National Center for Health Statistic;
2014.
13. Medical Service Act Article 3 [Internet]. Sejong: Korea Ministry of Govern- ment Legislation; 2015. [cited 2016 Jan 30]. Available from: http://www.law.
go.kr/lsInfoP.do?lsiSeq=177684&efYd=20160623#0000.
14. Shea AM, Curtis LH, Szczech LA, Schulman KA. Sensitivity of international classification of diseases codes for hyponatremia among commercially in- sured outpatients in the United States. BMC Nephrol 2008; 9: 5.
15. Katz JN, Barrett J, Liang MH, Bacon AM, Kaplan H, Kieval RI, et al. Sensitiv- ity and positive predictive value of medicare part B physician claims for rheumatologic diagnoses and procedures. Arthritis Rheum 1997; 40: 1594- 600.
16. Park BJ, Sung J, Park K, Seo SW, Kim SH. Studying on diagnosis accuracy for health insurance claims data in Korea [dissertation]. Seoul: Seoul National Univ.; 2003. p. 17-29. Korean.
17. O’Malley KJ, Cook KF, Price MD, Wildes KR, Hurdle JF, Ashton CM. Mea- suring diagnoses: ICD code accuracy. Health Serv Res 2005; 40: 1620-39.