Korean J Endocr Surg 2015;15:79-85
http://dx.doi.org/10.16956/kaes.2015.15.4.79
Endocrine Surgery
갑상선 결절의 수술 전 세침흡인세포검사 결과에 따라 수술 중 동결절편검사를 생략할 수 있는가?
경희대학교 의과대학 강동경희대학교병원 외과학교실
송정윤ㆍ한상아ㆍ장재훈ㆍ봉준우
Can We Omit Intraoperative Frozen Section According to the Result of the Preoperative Fine-needle Aspiration Cytology of a Thyroid Nodule?
Purpose: Fine needle aspiration (FNA) is a useful preoperative diagnostic tool for thyroid nodule because of the high sensitivity and specificity. The aim of this study is to determine the necessity of intraoperative frozen section (IOFS) after fine needle aspiration.
Methods: Data of 534 patients with a single thyroid nodule who underwent thyroidectomy from June 2006 to August 2013 were reviewed retrospectively. FNA was performed preoperatively in all patients and IOFS was performed selectively according to the intraoperative findings and FNA results. The sensitivity, specificity, positive predictive value, negative predictive value and accuracy of FNA and IOFS for malignant nodules were analyzed.
Results: The sensitivity, specificity, positive predictive value, negative predictive value, and accuracy of FNA for malignant nodules were 100%, 95.5%, 99.8%, 100%, and 99.8%, respectively. All nodules diagnosed as benign by FNA were reaffirmed as benign nodules by permanent sections. When the result of FNA was suspicious for malignancy, specific features of preoperative ultrasound, including hypoechoic, size<10 mm showed high positive predictive value and accuracy (98%, 86.9%, and 100%, 78.7% respectively).
Conclusion: Performance of IOFS was not necessary when the result of FNA was consistent with malignancy or benign. However when the result of FNA was non-diagnostic or atypia, IOFS should be performed for more accurate detection of malignancy. When the result of FNA is suspicious for malignancy, IOFS is restrictively useful for excluding benign nodules using the features of ultrasound. In addition, IOFS is not useful in finding malignant thyroid nodules when the result of FNA is follicular neoplasm.
Key Words: Fine needle aspiration, Intraoperative frozen section, Thyroidectomy, Accuracy 중심 단어: 세침흡인검사, 동결절편검사, 갑상선 절제술, 정확도
Jeong Yoon Song, Sang Ah Han, Jae Hoon Jang, Jun Woo Bong Department of Surgery at Gangdong Kyung Hee University Hospital, Kyung Hee University College of Medicine, Seoul, Korea
All funding sources and support for the research from Gangdong Kyung Hee University Hospital.
Received November 16, 2015, Revised November 24, 2015, Accepted December 2, 2015 Correspondence: Jun Woo Bong
Department of Surgery at Gangdong Kyung Hee University Hospital, 892 Dongnam-ro, Gangdong-gu, Seoul 05278, Korea Tel: +82-2-440-7000
Fax: +82-2-440-8197 E-mail: [email protected]
Copyright © 2015 Korean Association of Thyroid and Endocrine Surgeons; KATES. All Rights Reserved.
cc This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
서 론
세침흡인검사는 갑상선 결절에 대해서 진단적 목적 혹은 수술 범위 결정의 목적으로 시행하며, 악성 종양에 대한 민감도, 특이 도가 높아 선호되는 검사이다. 그러나 세침흡인 검사만으로는
악성세포의 침습도를 정확히 판단하기가 어렵고, 여포세포종양 의 경우에는 선별검사 정도의 역할만 할 경우가 많다. 한편 수술 중 동결절편검사는 수술 범위를 결정하는데 중요한 역할을 하기 도 하나, 비용 및 수술시간 연장, 수술 후 합병증 측면에 있어서 불리하다. 하지만 동결절편검사를 시행하여 불필요한 재수술을
Benign N (%) Malignant N (%)
Nodular hyperplasia 22 (4.1) Papillary carcinoma 488 (91.4)
Follicular adenoma 10 (1.9) Follicular carcinoma 6 (1.1)
Other benign tumor 6 (1.1) Anaplastic carcinoma 2 (0.4)
Total N=38 (7.1%) N=496 (92.9%)
Table 2. Final histologic diagnosis
Characteristics Total (N=534)
Sex (M:F) 97:437 (18.2%:81.8%)
Mean age (years) 47.9 (17∼81)
<45 210 (39.3%)
≥45 324 (60.7%)
Tumor size (mm) 11.0 (1∼90)
T stage
1, 2 205 (41.2%)
3, 4 292 (58.8%)
N stage
0 281 (56.5%)
1a 165 (33.2%)
1b 15 (3.0%)
Operation
Unilateral lobectomy 134 (25.1%) Total thyroidectomy 399 (74.9%)
Isthmectomy 1 (0.1%)
Table 1. Clinicopathological characteristics of patients who underwent operation for a single thyroid nodule
줄이게 되면 결과적으로 비용 효율 측면 및 재수술로 인한 불편 함과 합병증 면에서 유리한 경우도 있다.(1) 따라서 동결절편검 사가 유용성을 갖는 경우를 알아보고 반드시 시행해야 할 때만 시행하는 것이 치료의 효율성을 높이는 방법이 될 것이다.
방 법
본 연구는 본원에서 2006년 6월부터 2013년 8월까지 갑상선 결절로 수술 받은 총 942명 중 수술 전에 세침흡인검사를 받았으 며, 다발성 및 전이성 결절로 진단된 경우를 제외한 총 534명의 갑상선 단일 결절 환자를 대상으로 이루어졌다.
세침흡인검사의 결과는 Bethesda System에 의해 부적합검 체(non-diagnostic), 양성(benign), 비정형세포(atypia of un- determined significance), 여포세포종양(follicular neoplasm), 악성의심(suspicious malignancy), 악성(malignant)으로 분류 하였다.(2) 또한 수술 중 동결절편검사를 실시한 경우에는 검사 결과를 미실행(Not performed), 부적합검체(deferred), 양성 (benign), 여포세포종양(follicular neoplasm), 악성(malig- nant)으로 분류하였다.
갑상선 악성종양에 대한 민감도(Sensitivity), 특이도(speci- ficity), 양성예측도(positive predictive value), 음성예측도 (negative predictive value) 및 정확도(accuracy)를 최종 병리 진단 결과에 대한 양성(positive) 및 음성(negative)에 근거하여 다음과 같이 민감도=TP/(TP+FN), 특이도=TN/(TN+FP), 양 성예측도=TP/(TP+FP), 음성예측도=TN/(TN+FN), 정확도=
(TP+TN)/(TP+TN+FP+FN), (TP=true positive, TN=true negative, FP=false positive, FN=false negative) 산출하였다.
이 때 검사상 양성(positive)은 악성(malignant)으로 확인된 결 절로 정의하였고, 음성(negative)는 양성(benign)으로 확인된 결절로 정의하였다. 세침흡인검사상 음성이었으나 최종 병리결 과 상 미세유두암이 우연히 발견된 경우는 TN에 포함하였다. 동 결절편검사는 모든 경우에 실시하는 것을 원칙으로 했으며, 임 상적으로 혹은 수술 중 명확한 악성 소견이 관찰된 경우나 일부 여포세포 종양의 경우에 한해서 생략하였다.
결 과
534명의 환자들 가운데 남자는 97명(18.2%), 여자는 437명 (81.8%)이었고, 평균나이는 47.9세(17∼81세)였다. 결절의 평 균 크기는 11 mm (1∼90 mm)였고(Table 1), 최종 병리 결과에 서 양성 결절과 악성 결절로 진단 받은 예는 각각 38예(7.1%), 496예(92.9%)이었다(Table 2). 양성 종양 중 22예는 결절과다 증식(Nodular hyperplasia)이었고 10예는 여포선종(follicular adenoma), 6예는 기타양성종양이었다. 기타양성종양으로는 Chronic lymphocytic thyroiditis with oncocytic cells, gra- nulomatous thyroiditis, fibroinflammatory lesion, lympho- cytic thyroiditis, hyalinizing trabecular tumor 등이었다. 악 성 종양 중 가장 많은 것은 488예를 차지하는 유두암이었고, 미 분화암은 2예, 여포세포암은 6예로 나타났다, T stage는 T1, 2와 T3, 4가 각각 205예(41.2%), 292예(58.8%)였다. N stage는 N0, 1a, 1b가 각각 281예(56.2%), 165예(33.2%), 15예(3.0%) 였다. 수술 방법은 일측엽 절제술 134예(25.1%), 갑상선 전절제 술 399예(74.9%), 협부절제술 1예(0.1%) 시행하였다.
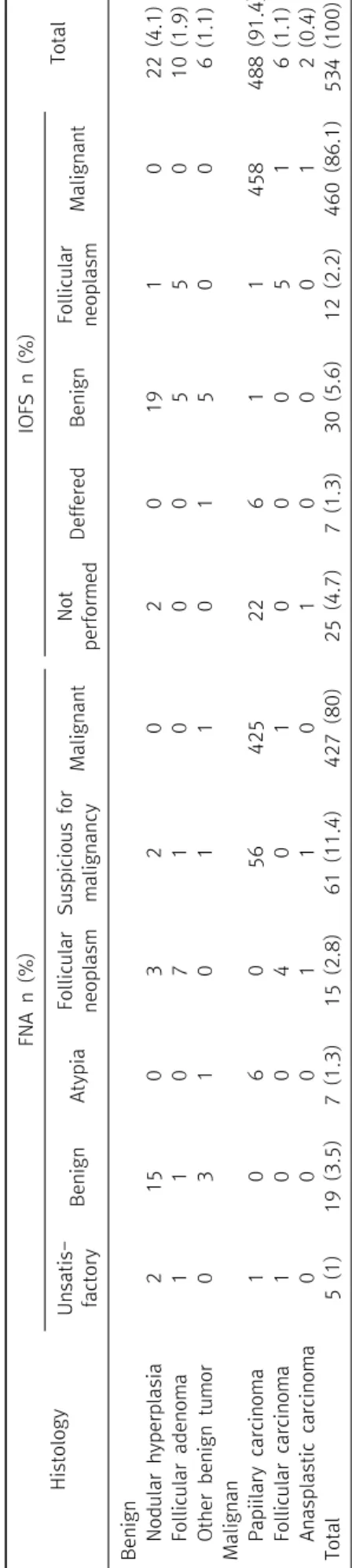
세침흡인검사 상 부적합검체, 양성, 비정형세포, 여포세포종 양이었던 경우는 각각 5예, 19예, 7예, 15예이었고 악성의심결
절과 악성이 각각 61예, 427예로 나타났다(Table 3). 세침흡인 검사에서 양성으로 나온 19예는 모두 최종 병리 검사 결과에서 양성이었으며 결절과다증식, 여포선종, 기타양성종양이 각각 15예, 1예, 3예이었다. 결절과다증식이 나온 군 중 3예는 우연히 최종병리검사상 미세유두상암이 발견되었다. 세침흡인검사에 서 악성으로 나온 427예 가운데 425예가 모두 최종병리검사 결 과에서 유두상암으로 나타났고 1예는 여포세포암이었으며, 1예 는 동결절편검사에서 부적합검체였으며 최종병리검사결과에 서 lymphocytic thyroiditis로 확진 되었다. 세침흡인검사에서 악성의심으로 나온 61예 가운데 4예(6.6%)는 최종 병리검사상 양성종양이었고 이는 모두 수술 중 시행한 동결절편검사에서 양 성종양임이 확인 되었다(Table 4).
세침흡인검사의 악성 종양(malignant)에 대한 민감도, 특이 도, 양성예측도, 음성예측도 및 정확도를 산출했을 때 각각 100%, 95.5%, 99.8%, 100%, 99.8%의 확률을 보이고 있었다.
악성의심결절을 양성(positive)에 포함하여 확률을 산출하면 민 감도, 특이도, 양성예측도, 음성예측도 및 정확도가 각각 100%, 80.8%, 99.6%, 100%, 99.0%으로 나타났다. 동결절편검사의 악 성 종양에 대한 민감도, 특이도, 양성예측도, 음성예측도 및 정확 도를 산출했을 때는 각각 98.5%, 100%, 100%, 96.7%, 99.8%의 확률로 나타났다(Table 5).
세침흡인검사상 악성의심세포였던 61예 중 44예(72.1%)는 크기가 1 cm 미만이었으며 이들은 모두 최종병리검사가 유두상 암으로 일치하였다. 1 cm 이상의 결절 17예(27.9%) 가운데 12 예(19.7%)는 동결절편검사 상 유두상암이었고 최종병리검사에 서 이와 일치하였으나, 나머지 4예(6.6%)에서는 동결절편 검사 상 양성결절이었고, 이는 모두 최종병리검사 결과와 일치하였 다. 그 외의 1예(1.6%)는 동결절편검사를 시행하지 않았고 최종 병리결과 미분화암이었다.
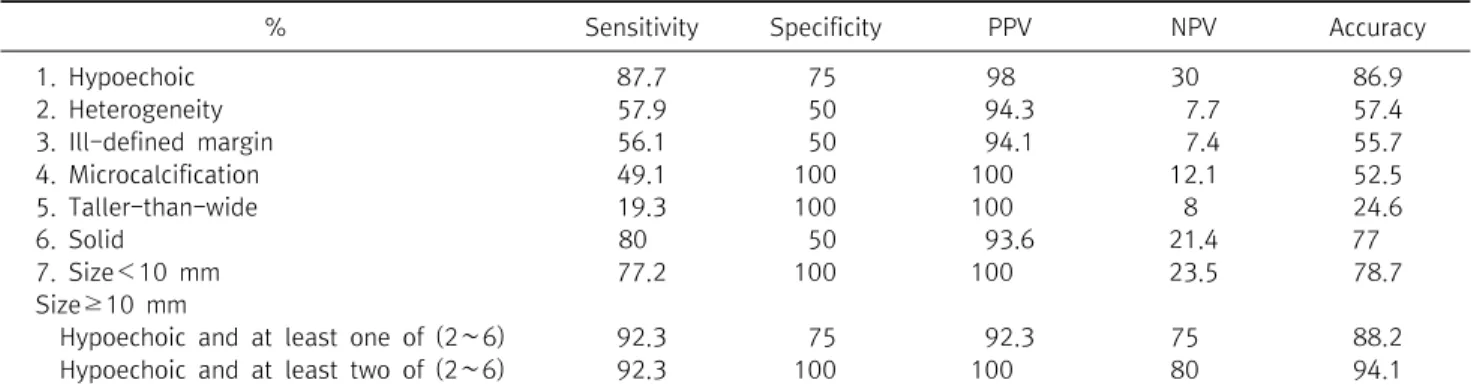
이들 세침흡인 검사상 악성의심세포였던 61예들의 초음파검 사 결과를 분석해보았을 때 악성을 시사하는 소견들로 저반향 (hypoechoic), 이질성(heterogeneity), 불분명한 경계(ill-de- fined margin), 미세석회화(microcalcification), taller-than- wide, 고형(solid) 등이 관찰되었다. 저반향 소견의 민감도, 특이 도, 정확도를 산출했을 때 각각 87.7%, 75%, 86%를 나타내었고, 고형의 민감도, 정확도는 각각 80%, 77%였으나 특이도는 50%였 다, 그 외의 이질성, 불분명한 경계, 미세석회화, taller-than- wide 등의 민감도는 19∼57%, 특이도는 50∼100%, 정확도는 24∼57%로 나타났다. 초음파상 크기가 1 cm 이상의 종양에서는 저반향의 특징을 보이면서 기타 악성을 시사하는 소견들을 2개 이상 포함할 경우에 민감도, 특이도, 양성예측도, 음성예측도, 정 확도가 각각 92%, 100%, 100%, 80%, 94%로 나타났다(Table 6).
Histology
FNA n (%)IOFS n (%) TotalUnsatis- factoryBenignAtypiaFollicular neoplasmSuspicious for malignancyMalignantNot performedDefferedBenignFollicular neoplasmMalignant Benign Nodular hyperplasia215032020191022 (4.1) Follicular adenoma1107100055010 (1.9) Other benign tumor031011015006 (1.1) Malignan Papiilary carcinoma10605642522611458488 (91.4) Follicular carcinoma100401000516 (1.1) Anasplastic carcinoma000110100012 (0.4) Total5 (1)19 (3.5)7 (1.3)15 (2.8)61 (11.4)427 (80)25 (4.7)7 (1.3)30 (5.6)12 (2.2)460 (86.1)534 (100) FNA = fine needle aspiration; IOFS = intraoperative frozen section.
Table 3. Final result of fine needle aspiration, frozen section and histologic findings
IOFS (n) Histologic finding (n)
FNA (n) Unsatisfactory (5) Benign (2) NH* (2)
Follicular neoplasm (2) FC* (1)/FA* (1)
Malignant (1) PTC* (1)
Benign (19) Benign (18) NH (15)/other benign* (3)
Follicular neoplasm (1) FA (1)
Atypia (7) Benign (1) Other benign (1)
Follicular neoplasm (1) PTC (1)
Malignant (5) PTC (5)
Follicular neoplasm (15) Not performed (2) NH (2)
Benign (4) FA (4)
Follicular neoplasm (8) FA (3)/FC (4)/NH (1)
Malignant (1) UC* (1)
Suspicious for malignancy (61) Not performed (1) UC (1) Differed to permanent (1) PTC (1)
Benign (4) NH (2)/other benign (2)
Malignant (55) PTC (55)
Malignant (427) Not performed (22) PTC (22)
Deffered to permanent (5) PTC (4)/NH (1)
Benign (2) PTC (2)
Malignant (398) PTC (397)/FC (1)
NH = Nodular hyperplasia; FC = Follicular carcinoma; FA = follicular adenoma; PTC = Papillary thyroid carcinoma; UC = undifferentiated carcinoma; FNA = fine needle aspiration; IOFS = intraoperative frozen section. *Other benign includes Chronic lymphocytic thyroiditis with oncocytic cells, granulomatous thyroiditis, fibroinflammatory lesion, lymphocytic thyroiditis, hyalinizing trabecular tumor.
Table 4. Correlation of fine needle aspiration and frozen section with final histologic findings
% FNA IOFS
Sensitivity 100 98.5
Specificity 95.5 100
Positive predictive value 99.8 100 Negative predictive value 100 96.7
Accuracy 99.8 99.8
Positive results include cases diagnosed as malignant by FNA or IOFS and negative results include cases diagnosed as benign by FNA or IOFS. FNA = fine needle aspiration; IOFS = intraoperative frozen section.
Table 5. Sensitivity, specificity, positive predictive value, negative predictive value and accuracy of fine needle aspiration and intraoperative frozen section for a single malignant thyroid nodule
세침흡인검사 결과 비정형세포로 나온 7예들 중 85.7%인 6예 는 최종 병리검사 결과 악성종양이었고 나머지 1예는 기타양성 종양(lymphocytic thyroiditis)으로 확인되었다. 악성종양으로 진단된 6예 중 5예에서는 수술 중 시행한 동결절편검사에서 악 성종양임이 확인되었고, 이 가운데 3예에서는 갑상선전절제로 수술전환이 이루어졌다. 기타양성종양으로 확인된 1예는 동결 절편검사 상에서 기타양성종양임이 확인 되어 최종병리검사와 일치하였다. 그리고 세침흡인검사 결과 여포세포종양으로 나온 15예들 중에 동결절편검사에서 양성으로 확인된 것은 4예 (30.8%)였으며 이는 모두 최종병리검사상 여포선종이었다. 1예
(7.7%)에서는 동결절편검사에서 미분화암임이 확인되어 갑상 선전절제를 시행하였고 최종병리검사에서도 미분화암이 나왔 다. 나머지 8예(61.5%)는 동결절편검사에서도 여포세포종양이 었고, 2예에서는 동결절편검사를 시행하지 않았다.
세침흡인검사상 부적합검체였던 5예는 동결절편검사를 통 해 유두상암 1예, 여포세포종양 2예, 양성종양 2예였고, 이 가운 데 유두상암과 양성종양의 경우는 최종병리검사 결과와 일치하 였고 여포세포종양이었던 2예는 각각 여포세포암과 여포선종 이었다.
동결절편검사가 수술 방법에 영향을 주었던 경우는 세침흡인 검사상 부적합검체 5예 중 동결절편검사상 유두상암과 양성종 양이었던 3예와 세침흡인검사상 비정형세포 7예중 동결절편검 사에서 유두상암과 양성종양이었던 6예, 그리고 세침흡인검사 상 여포세포종양이었던 13예 중 동결절편검사에서 미분화암이 었던 1예, 세침흡인검사상 악성의심종양 61예 중 동결절편검사 상 양성이었던 4예 총 14예(2.8%)였다.
고 찰
갑상선 결절은 유병률 5∼10%에 달하는 임상적으로 비교적 흔하게 접할 수 있는 질환으로서 이중 대부분은 양성 결절이나 약 30%에 가까운 확률로 악성 결절이 발견되고 있다.(3) 양성일
% Sensitivity Specificity PPV NPV Accuracy
1. Hypoechoic 87.7 75 98 30 86.9
2. Heterogeneity 57.9 50 94.3 7.7 57.4
3. Ill-defined margin 56.1 50 94.1 7.4 55.7
4. Microcalcification 49.1 100 100 12.1 52.5
5. Taller-than-wide 19.3 100 100 8 24.6
6. Solid 80 50 93.6 21.4 77
7. Size<10 mm 77.2 100 100 23.5 78.7
Size≥10 mm
Hypoechoic and at least one of (2∼6) 92.3 75 92.3 75 88.2
Hypoechoic and at least two of (2∼6) 92.3 100 100 80 94.1
PPV = positive predictive value; NPV = negative predictive value; FNA = fine needle aspiration; IOFS = intraoperative frozen section.
Positive results include cases diagnosed as malignant by FNA or IOFS and negative results include cases diagnosed as benign by FNA or IOFS.
Table 6. Sensitivity, specificity, positive predictive value, negative predictive value, accuracy and odd ratio of ultrasound findings of suspicious malignant nodules by FNA for a single thyroid nodule
경우 대부분은 수술적 제거 없이 경과 관찰하면 되나 초음파검사 에서 악성이 의심스러운 결과가 보인다거나 기도 압박으로 인한 불편감 또는 통증이 있다거나 크기가 갑자기 커지거나 환자가 원 하는 경우 등에 한해서 양성인 경우에도 수술을 시행할 수 있 다.(4) 그러나 악성 종양인 경우에는 적극적인 수술적 제거가 필 요하며, 대부분의 갑상선 결절은 초음파 세침흡인검사를 통해 수술 전 악성도를 확인한 후 수술 여부를 정하게 된다.
기존의 연구들에 따르면 세침흡인검사는 선별검사로 현재까 지 좋은 방법으로 선호되고 있다. Duek 등(3)은 갑상선결절로 수술 받은 총 206 예를 분석한 결과 세침흡인검사상 악성으로 나 온 53예 가운데 48예가 최종 병리 검사 결과 악성으로 나와 민감 도 78.1%, 특이도 96.5%, 양성예측도 90.5%, 정확도 91.2%에 달한다고 하였고, Gibb와 Pasieka (5)도 세침흡인검사에서 악 성종양이 나온 경우 정확도는 91%로 보고하였다. 이와 같은 세 침흡인검사를 통해 악성결절로 진단된 결절의 수술적 절제에 있 어서 수술 중 동결절편검사의 유용성에 대해 많은 연구가 이루어 지고 있다. Peng과 Wang (6)은 세침흡인검사를 통해 세포 검사 (cytology)상 악성 종양의 특징적(well-characterized) 핵 성상 을 관찰하는 것이 가능하기 때문이며, 갑상선 악성 결절의 대부 분을 차지하는 유두상암이 이와 같은 방법으로 진단할 수 있기 때문이라고 설명하였다. Wong 등(7)은 세침흡인검사상 악성의 심인 경우에서 민감도, 특이도, 양성예측도, 음성예측도가 각각 63.6%, 98%, 87.5%, 92.3%로 동결절편검사를 통해 악성종양이 나올 가능성을 확인하는 것이 필요하나, 세침흡인검사에서 악성 이 나온 경우는 민감도, 정확도, 양성예측도 모두 100%이므로 이 경우에는 동결절편검사가 생략될 수 있다고 주장하였다. 본 연구에서도 세침흡인검사와 동결절편검사 간의 민감도(100%
vs 98.5%), 특이도(95.5% vs 100%), 양성예측도(99.8% vs 100%), 음성예측도(100% vs 96.7%), 정확도(99.8% vs 99.8%)가 큰 차
이가 없어 이와 같은 사실을 뒷받침하고 있었다.
동결절편검사는 세침흡인검사 상 부적합검체 혹은 미결정세 포의 경우에서 유용할 수 있다. Chang 등(8)은 세침흡인검사와 동결절편검사가 불일치 할 경우 동결절편검사가 세침흡인검사 보다 더 높은 정확도(78.9%>21.1%)를 보인다고 하며, 특히 세 침흡인 검사에서 미결정(indeterminate or unsatisfactory)인 결절에서 정확도가 92.6%로 나타난다고 하였다. Lee와 Cho (9) 는 세포흡인검사상 미결정이었으나 동결절편검사에서 양성으 로 나온 예가 34예 가운데 16예(47.1%)로 이 경우 수술의 방법 이 달라졌음을 근거로 동결절편의 유용성을 주장하였다. 본 연 구에서는 세침흡인검사상 부적합검체, 비정형세포에서는 각각 3예(60%), 6예(85.7%)에서 동결절편검사가 수술방법에 영향을 주었다.
세침흡인검사상 여포세포종양인 경우에는 동결절편검사의 유용성이 높지 않다. 세침흡인검사에서 여포세포종양으로 진단 되었던 결절 중에 최종병리검사에서 악성으로 진단될 확률은 약 20%로 보고 있는데, 여포세포암의 경우에는 캡슐과 혈관의 침 범도를 관찰하는 것이 중요하나 세침흡인검사만으로는 이와 같 은 특성을 관찰하기가 어려워서 최종병리검사 결과에 의해서만 진단이 가능한 경우가 있다.(1,10) 특히 여포변이성 유두상암 (follicular variant of papillary thyroid carcinoma)의 경우에 는 세침흡인검사상 여포세포종양으로만 나와 위음성일 가능성 이 높다.(5,10,11) Chen 등(12)은 세침흡인검사에서 여포세포 종양이 나온 환자들 중에 동결절편 검사를 시행한 경우 87%는 불필요하였으며, 5%에서는 최종병리검사와 다른 결과를 나타 냈다고 하였다. Boyd 등(13)은 세침흡인검사에서 여포세포종양 으로 나온 49예 중 3예는 동결절편검사를 통해 악성의심 또는 악 성으로 진단되었고, 21예는 양성종양으로 진단되어 24예에서 수술 방향 결정에 영향을 주었으나, 22예에서는 여전히 여포세
Fig. 1. Flow chart for the diagnosis of a single thyroid nodule.
Suspicious features include hypoechoic, heterogeneity, ill-defined margin, microcalcification, taller-than- wide and solid, FNA = fine needle aspiration; IOFS = intra- operative frozen section; US = ultrasound.
포종양으로 진단되었고, 동결절편검사의 최종 양성예측도는 7%로 세침흡인검사의 6%와 큰 차이가 없다고 하였다. 본 연구에 서는 세침흡인검사로 여포세포종양이 총 13예 진단되었고 이 중 5예(38.5%)에서 동결절편검사가 최종병리검사와 일치하였지 만 실제 수술방법에 영향을 준 경우는 1예(7.8%)만 있었다. 따라 서 세침흡인 검사 결과 여포세포종양이 나온 경우 동결절편검사 결과는 수술 범위를 정하는데 도움을 주지 못하는 경우가 많고, 환자의 나이나 종양의 크기, 경부방사선조사여부, Hurthle cell neoplasm 여부 등의 기타 다른 정보를 종합하여 수술의 정도를 결정하게 된다.(11,12)
세침흡인검사상 악성의심의 경우에는 동결절편검사가 제한 적으로 유용할 수 있다. 세침흡인검사는 결절의 크기가 클수록 정확도가 감소하는 것으로 알려져 있는다. Agcaoglu 등(14)은 결절의 크기가 2∼4 cm인 경우는 위음성도가 4.9∼5배 증가한 다고 분석하고 있고, Siddiqui 등(15)은 위음성률을 나타낸 그룹 에서는 그렇지 않은 그룹보다 절제 후 악성 종양의 크기와 초음 파 검사상 임상적 결절의 크기의 차이가 더 크며 이는 결절의 크 기가 증가할수록 이질성(heterogeneity)이 증가하기 때문이라 고 하였다. McCoy 등(16)은 4 cm 이상의 결절에서는 세침흡인 검사의 위음성도가 높기 때문에 결과에 상관 없이 진단적 목적의 절제술이 필요하다고 하였다. Degirmenci 등(17)은 크기가 1 cm 미만의 결절에서는 약 76.4%에서 진단에 충분한 검체가 검 출될 수 있었으나 1∼3 cm의 결절에서는 65.9%, 3 cm 이상의 결절에서는 56.8%로 결절의 크기가 증가할수록 혈관분포, 결절 내 혈관 직경, 결절 내 괴사성 영역의 비율이 증가하기 때문에 결 과에 오류를 가져올 수 있다고 설명하였다. 본 연구에서는 세침 흡인검사상 악성의심세포였던 61예 중 1 cm 미만의 44예는 모 두 동결절편검사와 최종병리검사결과가 악성으로 일치하였으 나, 악성의심세포이면서 1 cm 이상의 결절 17예에서는 4예에서 동결절편 검사상 양성결절이었고, 이는 최종병리검사 결과와 일 치하였다.
이러한 세침흡인검사의 정확도를 높일 수 있다면 더 효율적인 치료가 이루어질 수 있겠으나 이는 세침흡인검사의 방법적인 한 계점으로 쉽게 극복되지 않을 것으로 보인다. 다만 임상적 초음 파검사에서 악성을 시사하는 특징을 보이는 결절에서는 세침흡 인검사 결과가 양성일지라도 위음성 가능성이 높을 것으로 추정 할 수 있다. Yoon 등(18)은 3 cm 이상의 결절에서 최종병리검사 결과상 양성과 악성이었던 결절들의 특징을 분석한 결과 악성 결 절에서 경계가 불분명한(ill defined), 저반향의(hypoechoic), 석회화(calcification)가 동반된 특징들이 더 높게 나타난다고 하였다. 그 외의 많은 연구에서 고형(solid), 저반향, 석회화, 불 분명한 경계, 이질성, 종양내 혈관분포(intranodular vasculari-
zation), 모양(taller than wide) 등의 소견을 초음파상 악성을 시사하는 특징적인 소견으로 분류하였다.(19-21) Cappelli 등 (19)은 이 가운데 둘 이상의 조합으로 판단할 경우에 만족할 만 한 예측도를 보인다고 하였고, Papini 등(21)은 저반향의 특징을 포함한 최소한 두 개 이상의 특징을 보이는 조합에서 만족할 만 한 악성 예측도를 보인다고 하였다. 본 연구에서는 세침흡인검 사상 악성의심세포였던 결절들의 초음파 검사상 크기 1 cm 미 만 결절의 특이도 및 양성예측도는 모두 100%였고, 크기가 1 cm 이상의 결절들 가운데 저반향의 특징과 함께 다른 악성을 시 사하는 특징적 소견을 2개 이상 보이는 경우에 민감도, 특이도와 정확도가 각각 92.3%, 100%, 94.1%를 보였다. 따라서 세침흡인 검사상 악성의심세포인 경우에 이와 같은 결절의 크기와 임상적 초음파결과를 고려하여 일부의 결절에 한해서 동결절편검사를 시행해 볼 수 있을 것이다(Fig. 1). 그러나 이는 충분한 만큼의 규 모에서 도출된 결론이 아니며 유두상암의 초음파소견만을 활용 한 것이므로 한계점이라 할 수 있으며, 악성의심결절에 대한 연 구에 대해 향후 계속적인 연구가 뒷받침되어야 할 것이다.
결 론
본 연구에 따르면 세침흡인검사상 악성(benign) 혹은 양성 (malignant) 종양일 경우 수술 중 동결절편검사를 생략할 수 있 을 것으로 생각할 수 있다. 그러나 세침흡인검사의 검사상 부적 합검체 및 비정형세포의 경우에는 동결절편검사가 수술 중 중요 한 역할을 할 수 있으며, 여포세포종양의 경우에는 동결절편검 사가 유용하지 않다고 할 수 있다. 또한 세침흡인검사상 악성의 심세포인 경우에는 동결절편검사가 초음파검사상 결절의 크기 및 특징 등을 고려하여 제한적으로 유용할 수 있다.
REFERENCES
1. LiVolsi VA, Baloch ZW. Use and abuse of frozen section in the di- agnosis of follicular thyroid lesions. Endocr Pathol 2005;16:
285-93.
2. Cibas ES, Ali SZ; NCI Thyroid FNA State of the Science Con- ference. The bethesda system for reporting thyroid cytopa- thology. Am J Clin Pathol 2009;132:658-65.
3. Duek SD, Goldenberg D, Linn S, Krausz MM, Hershko DD. The role of fine-needle aspiration and intraoperative frozen section in the surgical management of solitary thyroid nodules. Surg Today 2002;32:857-61.
4. Kahmke R, Lee WT, Puscas L, Scher RL, Shealy MJ, Burch WM, et al. Utility of intraoperative frozen sections during thyroid surgery. Int J Otolaryngol 2013;2013:496138.
5. Gibb GK, Pasieka JL. Assessing the need for frozen sections: still a valuable tool in thyroid surgery. Surgery 1995;118:1005-9.
6. Peng Y, Wang HH. A meta-analysis of comparing fine-needle aspiration and frozen section for evaluating thyroid nodules.
Diagn Cytopathol 2008;36:916-20.
7. Wong CK, Wheeler MH. Thyroid nodules: rational manage- ment. World J Surg 2000;24:934-41.
8. Chang HY, Lin JD, Chen JF, Huang BY, Hsueh C, Jeng LB, et al.
Correlation of fine needle aspiration cytology and frozen sec- tion biopsies in the diagnosis of thyroid nodules. J Clin Pathol 1997;50:1005-9.
9. Lee YD, Cho HJ. The role of fine-needle aspiration cytology and frozen section in the operative management of thyroid nodule.
Korean J Endocr Surg 2001;1:78-83.
10. Kesmodel SB, Terhune KP, Canter RJ, Mandel SJ, LiVolsi VA, Baloch ZW, et al. The diagnostic dilemma of follicular variant of
papillary thyroid carcinoma. Surgery 2003;134:1005-12.
11. McHenry CR, Thomas SR, Slusarczyk SJ, Khiyami A. Follicular or Hürthle cell neoplasm of the thyroid: can clinical factors be used to predict carcinoma and determine extent of thyroi- dectomy? Surgery 1999;126:798-802.
12. Chen H, Nicol TL, Udelsman R. Follicular lesions of the thyroid.
Does frozen section evaluation alter operative management?
Ann Surg 1995;222:101-6.
13. Boyd LA, Earnhardt RC, Dunn JT, Frierson HF, Hanks JB.
Preoperative evaluation and predictive value of fine-needle as- piration and frozen section of thyroid nodules. J Am Coll Surg 1998;187:494-502.
14. Agcaoglu O, Aksakal N, Ozcinar B, Sarici IS, Ercan G, Kucukyil- maz M, et al. Factors that affect the false-negative outcomes of fine-needle aspiration biopsy in thyroid nodules. Int J Endo- crinol 2013;2013:126084.
15. Siddiqui MA, Griffith KA, Michael CW, Pu RT. Nodule hetero- geneity as shown by size differences between the targeted nod- ule and the tumor in thyroidectomy specimen: a cause for a false-negative diagnosis of papillary thyroid carcinoma on fine- needle aspiration. Cancer 2008;114:27-33.
16. McCoy KL, Jabbour N, Ogilvie JB, Ohori NP, Carty SE, Yim JH.
The incidence of cancer and rate of false-negative cytology in thyroid nodules greater than or equal to 4 cm in size. Surgery 2007;142:837-44.
17. Degirmenci B, Haktanir A, Albayrak R, Acar M, Sahin DA, Sahin O, et al. Sonographically guided fine-needle biopsy of thyroid nodules: the effects of nodule characteristics, sampling techni- que, and needle size on the adequacy of cytologicalmaterial.
Clin Radiol 2007;62:798-803.
18. Yoon JH, Kwak JY, Moon HJ, Kim MJ, Kim EK. The diagnostic accuracy of ultrasound-guided fine-needle aspiration biopsy and the sonographic differences between benign and malig- nant thyroid nodules 3 cm or larger. Thyroid 2011;21:993-1000.
19. Cappelli C, Castellano M, Pirola I, Cumetti D, Agosti B, Gandossi E, et al. The predictive value of ultrasound findings in the man- agement of thyroid nodules. QJM 2007;100:29-35.
20. Frates MC, Benson CB, Doubilet PM, Kunreuther E, Contreras M, Cibas ES, et al. Prevalence and distribution of carcinoma in pa- tients with solitary and multiple thyroid nodules on sonogra- phy. J Clin Endocrinol Metab 2006;91:3411-7.
21. Papini E, Guglielmi R, Bianchini A, Crescenzi A, Taccogna S, Nardi F, et al. Risk of malignancy in nonpalpable thyroid nod- ules: predictive value of ultrasound and color-Doppler features.
J Clin Endocrinol Metab 2002;87:1941-6.