Address reprint requests to Hoo Young Lee, M.D.
Department of Rehabilitation Medicine and Rehabilitation, Gangnam Severance Hospital, 211 Eonju-ro, Gangnam-gu, Seoul 135-720, Korea
TEL: 82-2-2227-2576, FAX: 82-2-2228-7877, E-mail: [email protected]
투고일: 2014년 7월 2일, 1차 수정일: 2014년 8월 6일, 2차 수정일: 2014년 8월 31일, 게재확정일: 2014년 8월 31일
INTRODUCTION
Diabetic thoracic polyradiculopathy (DTP) is an uncommon complication of diabetes mellitus, of which onset is abrupt or gradual and pain or dysesthesia is pre- dominantly unilateral in a radicular distribution.1Since
comprehensive epidemiological data on DTP are lack- ing, physicians must rely on the case reports for informa- tion relevant to practice.2The awareness of multidiscipli- nary approach to DTP is rather poor. Hence, most of patients are referred late to neurology or rehabilitation specialists after they had undergone several tests for dif-
양측성 당뇨병성 흉추부 다발신경근병증으로 진단된 아급성 상부 복통 1예
1국민건강보험 일산병원 재활의학과, 2연세대학교 의과대학 강남세브란스병원 재활의학과
김형섭
1∙김성우
1∙이후영
2– Abstract –
Subacute Upper Abdominal Pain Diagnosed as Bilateral Diabetic Thoracic Polyradiculopathy - A Case Report -
Hyoung Seop Kim, M.D.
1, Seong Woo Kim, M.D.
1, Hoo Young Lee, M.D.
21Department of Rehabilitation Medicine, National Health Insurance Service Ilsan Hospital, Goyang GyeongGi-Do
2Department of Rehabilitation Medicine, Gangnam Severance Hospital, Rehabilitation Institute of Neuromuscular Disease, Yonsei University College of Medicine, Seoul, Korea
Diabetic thoracic polyradiculopathy is characterized by abrupt onset and predominantly unilateral radicular pain in diabetic patients. It is not generally well-recognized, thus leads to misdiagnosis. A 61-year-old female patient visited outpatient clinic for severe right flank and bilateral abdomen pain. The cause of pain was not diagnosed, but uncontrolled blood sugar was revealed. Hence, she was admitted and several diagnostic studies were performed to rule out somatoform disorder, diabetic ketoacidosis, intra-abdominal disorders and polyradiculopathy of inflammation, infection, autoimmune, and neoplastic causes. Then she was consulted on further diagnostic workup and management of pain. We confirmed bilateral diabetic thoracic polyradiculopathy by electromyography and revealed that the pain was not originated from spinal diseases by thorax spine magnetic resonance image. The pain was controlled with tramadol/
acetaminophen without complication. We report this distinctive case with a brief review of the related literatures.
Key Words: diabetic neuropathies, polyradiculopathy, electromyography
ferential diagnosis. To our knowledge, no case on two- sided and symmetric invasion of DTP has been reported so far. Here, we present a case of bilateral DTP which was differentiated from somatoform disorder, diabetic ketoacidosis, kidney stone, and other polyradiculopathy of infectious or autoimmune causes and then confirmed as DTP by electromyography (EMG).
A CASE REPORT
A 61-year-old female patient, who had been diabetic for 15 years, was referred to our clinic for diagnostic workup and further management of the pain. Blood sugar level had not been controlled well for last three months. The pain was ‘stinging, lacinating, and deep’
and invaded bilateral upper abdomen and right flank.
Then it extended to mid back. Pain severity at onset reached 10 out of 10 on visual analogue scale (VAS).
She lost two kilograms in two weeks. She had suffered nausea, constipation, and poor gas passing. First, she vis- ited the outpatient clinic and diagnostic workup was done to rule out kidney stone. Two days before follow- up visit, she visited the emergency room at around three a.m., complaining of debilitating pain and consecutive insomnia. Emergency workup failed to find the source of abdominal pain, so the primary doctor of emergency room could not rule out possibility of somatoform disor- der. She was guided to revisit the clinic and abdominal and pelvic computer tomography (APCT) was per- formed. No significant findings were noted in APCT. In laboratory tests, the postprandial glucose level was 370 mg/dL. Hence, she admitted for blood sugar control and pain management. It took 14 days from the onset of pain to the admission.
On the first day of the hospitalization, vital signs were all within the normal range. The complete blood count and blood chemistry test items were within normal limit apart from a random blood glucose measurement of 353 mg/dL and HbA1c of 10.5%. Urinalysis detected only glycosuria without proteinuria or hematuria. On electro- cardiography and chest-abdominal radiography, abnor- malities were not observed.
Fundoscopy showed diabetic retinopathy in the right eye. Esophagogastroduodenoscopy revealed no particu- lar abnormalities other than mild, chronic superficial gastritis in the antrum. Colonoscopy found two 6-cen- timeter-sized polyps, for which an endoscopic polypec- tomy was performed. There were not any other abnor-
malities and complications.
Management included strict glycemic control with oral medication and a compound of tramadol/acetaminophen which began to be administered on the fourth day. Its first dosage was 150 mg/1300 mg. Then, pain severity fell by 2 on VAS. The patient could be released after 7 days of hospital stay.
The patient visited our clinic 3 weeks after discharge.
Neurological examination revealed no diseases of con- sciousness and no cranial nerve disorders. She was grad- ed normal in both upper and lower extremities by manu- al muscle testing method. Abdominal wall was normo- tonic and abdominal muscle bulging was not observed.
Sensory examination showed an area of hyperalgesia and allodynia along bilateral upper abdomen, flank, and tho- racic back which corresponded to bilateral and symmet- rical T3 to T8 dermatomes. Pinprick and vibration senses were normal. Deep tendon reflexes were normal and Babinski reflex was absent. According to her statement, the most severe and the first occurrence of pain was in right flank area. She had no history of herpes zoster. Any cutaneous lesions such as vesicle or crusting were not seen. Moreover, we distinguished polyradiculopathy of inflammatory, infection, neoplastic, and autoimmune causes from her medical history and physical exam results.
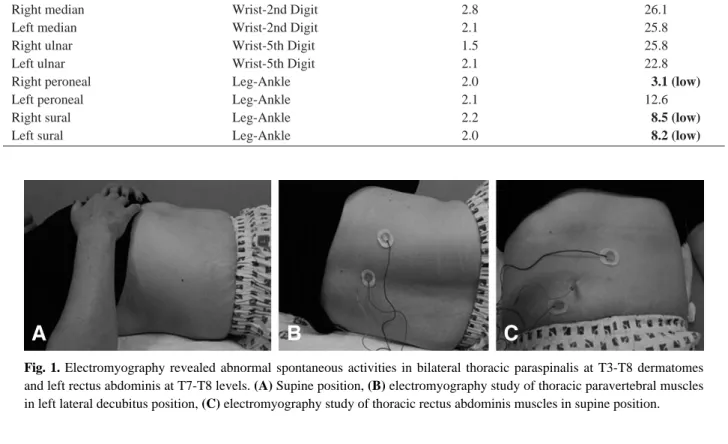
With diagnostic impression of diabetic thoracic polyradiculopathy (DTP), electromyography (EMG) and nerve conduction study (NCS) were performed. Periph- eral nerves conducted normally in motor nerve fibers of bilateral upper and lower extremities. Peripheral sensory nerve conduction study showed distal sensory polyneu- ropathy in both lower extremities (Table 1). And EMG of the thoracic paraspinal musculature confirmed the diagnosis by increased insertional activities and abnor- mal spontaneous activities (positive sharp wave/fibrilla- tion) in the left rectus abdominis and in bilateral T3-T8 paraspinal muscles indicating denervation in the distribu- tion of the affected roots (Fig.1, Table 2). On thorax spine MRI, any abnormal findings such as herniated discs, myelopathy and cancer metastasis were not observed (Fig.2).
The daily dose of tramadol/acetaminophen was slowly reduced by 325 mg/37.5 mg in 3 weeks. The pain severi- ty decreased to 1 on VAS. Hence, she was scheduled to revisit our clinic a month later and consider discontinua- tion of the medication.
DISCUSSION
Diabetic amyotrophy or diabetic lumbosacral radiculo- plexus neuropathy affects lumbosacral nerve roots and peripheral nerves, of which the traditional features include the acute, asymmetric, focal onset of pain fol- lowed by weakness involving the proximal leg, with associated autonomic failure and weight loss. Involve-
ment of similar elements of the nervous system that orig- inate from the thoracic spinal cord causes pain in the abdomen or, in the case of upper thoracic cord disease, the chest, as in DTP.2 Namely, DTP share the same pathophysiology with diabetic amyotrophy but may be distinguished by the affected site.
DTP usually occurs in middle-aged or elderly patients with type II diabetes, and there is no sex predominance.
Fig. 1. Electromyography revealed abnormal spontaneous activities in bilateral thoracic paraspinalis at T3-T8 dermatomes and left rectus abdominis at T7-T8 levels. (A) Supine position, (B) electromyography study of thoracic paravertebral muscles in left lateral decubitus position, (C) electromyography study of thoracic rectus abdominis muscles in supine position.
A B C
Table 1. Results of Sensory Nerve Conduction Studies
Nerve Segment Latency (msec) Amplitude (μV)
Right median Wrist-2nd Digit 2.8 26.1
Left median Wrist-2nd Digit 2.1 25.8
Right ulnar Wrist-5th Digit 1.5 25.8
Left ulnar Wrist-5th Digit 2.1 22.8
Right peroneal Leg-Ankle 2.0 3.1 (low)
Left peroneal Leg-Ankle 2.1 12.6
Right sural Leg-Ankle 2.2 8.5 (low)
Left sural Leg-Ankle 2.0 8.2 (low)
Table 2. Results of Needle Electromyography Muscles
Insertional
PSW/Fib MUAP
Interference
Activity Pattern
Rt.& Lt. paraspinalis (C5-C6, C7-C8, T1-T2) NMU -
Rt.& Lt. paraspinalis (T3-T4) Increased ++ NMU -
Rt.& Lt. paraspinalis (T5-T6) Increased ++ NMU -
Rt.& Lt. paraspinalis (T7-T8) Increased ++ NMU -
Rt.& Lt. paraspinalis (T9-T10, T11-T12) NMU -
Rt.& Lt. paraspinalis (L1-L2, L3-L4, L5-S1) NMU -
Rt.& Lt. rectus abdominis (T6) NMU Complete
Rt. rectus abdominis (T7) Increased NMU Complete
Lt. rectus abdominis (T7) Increased ++ NMU Complete
Rt. rectus abdominis (T8) Increased NMU Complete
Lt. rectus abdominis (T8) Increased ++ NMU Complete
Rt.& Lt. rectus abdominis (T9, T10, T11) NMU Complete
PSW, Positive sharp wave, Fib, Fibrillation, MUAP, Motor unit action potential, NMU, Normal motor unit
Other diabetic complications, including retinopathy, nephropathy, and other forms of neuropathy are com- mon. DTP is easily accompanied by autonomic disorders such as orthostatic hypotension, but rarely, there is simultaneous lumbosacral polyradiculopathy. Concomi- tant weight loss and nausea are common, so it needs to be differentiated from an intraabdominal and retroperi- toneal malignancy, especially pancreatic carcinoma.
Weakness of abdominal muscles due to denervation may lead to protrusion of the abdominal wall as a hernia.2 Also, it may accompany diabetic gastroparesis which is similar to paralytic ileus of diabetic ketoacidosis. Thus, acidosis, hypokalemia and signs of absent bowel sound should be checked. Postherpetic neuralgia is likely to be confused with DTP because unilateral, radicular pain invades certain dermatomes and it may persist after dis- appearance of the rash. In case of zoster sine herpete, that is varicella zoster virus reactivation without rash, differential diagnosis become more difficult. Further- more, it should be differentiated from intervertebral discs
or adjacent tumors which may also accompany weight loss and denervation along affected nerve roots. They can be identified on thoracic MRI.1-3 Polyradiculopathy by autoimmune disorders such as acute inflammatory demyelinating polyradiculopathy, chronic inflammatory demyelinating polyradiculopathy, and paraprotein-relat- ed syndromes and by infectious or neoplastic causes should be distinguished as well.
Recent studies suggest that the pathological abnormali- ties are immune-mediated. Inflammation surrounding epineural microvessels and other changes consistent with vasculitic ischemic injury has been revealed in skin biop- sies, offering hope that plasma exchange, intravenous immunoglubin and corticosteroid therapy may be effec- tive. There is no clear relationship between blood sugar control and the disorder.2
A definite diagnosis can be made through paraspinal EMG after ruling out other compounding disorders with similar abdominal pain. As in diabetic amyotrophy which is the most common form of asymmetric diabetic neuropathy, DTP is predominantly asymmetric and uni- lateral.2,4 It is of diagnostic value as distribution of the pain corresponds to the involved thoracic nerve roots and displayed abnormal spontaneous activities.3 Meanwhile, authors recommend EMG of rectus abdominis muscle to distinguish from malignancy that invades only posterior ramus segment.5
So far, the mainstay of treatment is symptomatic therapy.
Any controlled trials of treatment for DTP have not been reported, however, it appears that DTP-related pains are partially relieved by symptomatic therapy for diabetic polyneuropathy (DPN).3According to the evidence- based guidelines on DPN, pregabalin is the only level-A recommendation. Tramadol is level-B recommendation.6 However, narcotic analgesics may be necessary because pain associated with DTP is extreme in most cases.2
Tramadol is a centrally acting analgesic in spinal level that relieves pain through combination of weak mu-opi- oid agonist activity and inhibition of norepinephrine and serotonin reuptake.7Acetaminophen is a broad-spectrum analgesic and is known to take a central antinociceptive effect. It is commonly used for concomitant analgesia or analgesic rescue therapy in clinical trials of painful DPN. Tramadol/acetaminophen relieved the pain signif- icantly and had fewer adverse events than tramadol monotherapy.8
This case is unique in two aspects. It is the first and foremost to comprehensively report on bilateral symmet- Fig. 2. T2 weighted thorax spine MRI showed no definite
evidence of thoracic disc herniation and no abnormal sig- nal change on visible spinal cord.
rical DTP including clinical characteristics, differential diagnosis, treatment, and follow-up management. A case series by Streib et al reported electrodiagnostic study of diabetic thoracic radiculopathy.5Among 14 subjects, one subject showed bilateral distribution of fibrillation poten- tials. But chief complaints, physical exam, diagnosis, treatment and prognosis were not reviewed. Another case series report on diabetic radiculopathy by Longstreth et al included a case of a patient who showed denervation potentials in bilateral paraspinal muscle but differential diagnosis was not mentioned overall.9And, it took more than a year to be relieved in the case but treat- ment process was not reviewed. Second, pain was con- trolled almost completely by tramadol/acetaminophen in three weeks. Other reported cases of DTP were treated with anticonvulsants or tricyclic antedepressant includ- ing the most recent review article.2
In conclusion, DTP should be suspected in diabetics with severe pain in bilateral multiple thoracic root distri- bution along with neuropathic cachexia after excluding differential diagnosis. Prompt recognition and proper management are important in two respects: (1) sympto- matic therapy relieves pain significantly in a short period (2) pain runs a clearly defined course and remit, usually completely, within 6~18 months, without recurring at a later time.10
REFERENCES
1. Said G. Diabetic neuropathy-a review. Nature Clinical Practice Neurology 2007;3:331-340
2. Longstreth GF. Diabetic thoracic polyradiculopathy. Best Practice & Research Clinical Gastroenterology 2005;19:
275-281
3. Kikta DG., Breuer AC, Wilbourn AJ. Thoracic root pain in diabetes: the spectrum of clinical and electromyograph- ic findings. Annals of neurology 1982;11:80-85
4. Pasnoor M, Dimachkie MM, Barohn RJ. Diabetic neu- ropathy part 2: proximal and asymmetric phenotypes.
Neurologic clinics 2013;31:447-462
5. Streib EW, Sun SF, Paustian FF, Gallagher TF, Shipp JC, Ecklund RE. Diabetic thoracic radiculopathy: electrodiag- nostic study. Muscle & nerve 1986;9:548-553
6. Bril V, England J, Franklin GM, Backonja M, Cohen J, Toro DD, et al. Evidence-based guideline: Treatment of painful diabetic neuropathy: report of the American Acad- emy of Neurology, the American Association of Neuro- muscular and Electrodiagnostic Medicine, and the Ameri- can Academy of Physical Medicine and Rehabilitation.
PM&R 2011;3:345-352
7. Hollingshead J, Duehmke RM, Cornblath DR. Tramadol for neuropathic pain. Cochrane Database of Systematic Reviews 2006;3:CD003726
8. Freeman R, Raskin P, Hewitt DJ, Vorsanger GJ, Jordan DM, Xiang J, Rosenthal NR. Randomized study of tra- madol/acetaminophen versus placebo in painful diabetic peripheral neuropathy. Current Medical Research and Opinion 2006;23:147-161
9. Longstreth GF, Newcomer AD. Abdominal pain caused by diabetic radiculopathy. Annals of internal medicine:
1977;86:166-168
10. Chaudhuri KR, Wren DR, Werring D, Watkins PJ. Unilat- eral abdominal muscle herniation with pain: a distinctive variant of diabetic radiculopathy. Diabetic medicine 1997;
14:803-807